27
Preterm infants and their complications
The preterm infant differs markedly from the term infant in size, appearance and development. Some of these differences are shown schematically in Figs 27.1–27.4.

Fig. 27.1 Maturational changes in appearance, posture and development with age.

Fig. 27.2 Preterm infant at 23 weeks’ gestation, showing thin, gelatinous skin and fused eyelids Legs flexed as nested. Tracheal and gavage (nasogastric) tubes.

Fig. 27.3 Preterm infant at 30 weeks’ gestation, showing medium-thickness skin and ear with cartilage to edge of pinna.

Fig. 27.4 Term infant showing flexed posture and thick skin, and well-formed ear.
Morbidity
Being born preterm has many disadvantages, including stress for the parents and family, prolonged hospitalization and being extremely expensive. After 30 weeks of gestation, most preterm infants in developed countries survive without neurologic or other impairment. However, at lower gestational age there is a considerable complication rate (Fig. 27.5). The rate is highly dependent on gestational age.
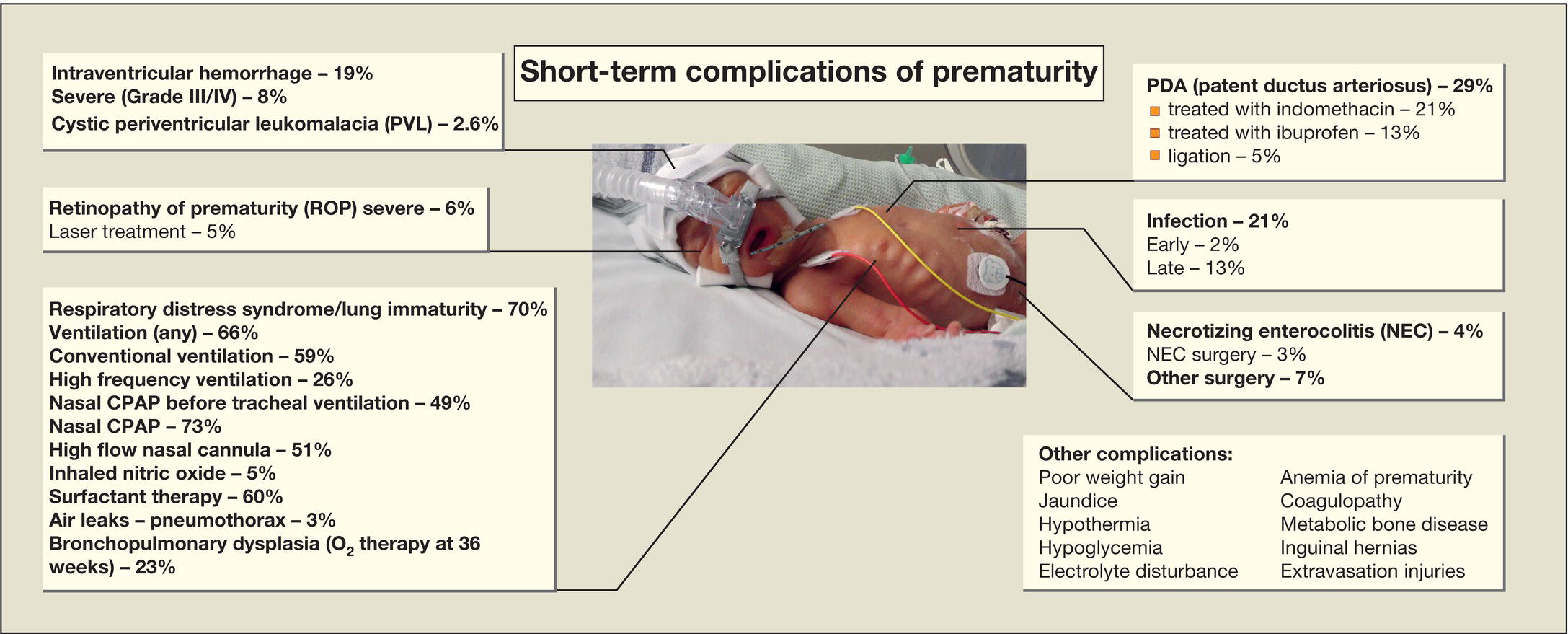
Fig. 27.5 Short-term complications of very low birthweight (<1.5 kg) infants.
(Percentages are based on Vermont–Oxford Network data for 2013.)
Mortality
Mortality is mainly determined by gestational age (Fig. 27.6) and birthweight (Fig. 27.7). They interact with each other as well as with other risk factors:
- gender (males have higher mortality)
- ethnicity
- multiple birth (increases mortality).
Fig. 27.6 Survival by gestational age of very low birthweight (VLBW) infants.
Data from over 900 neonatal units from throughout the world. (Vermont–Oxford Network, 2012.)
Fig. 27.7 Survival by birthweight of very low birthweight (VLBW) infants. Overall survival 88%.
(Vermont–Oxford Network 2012.)
There has been a marked improvement in survival in infants born at the limit of viability, i.e. 23–25 weeks of gestational age. However, mortality, morbidity and adverse neurodevelopmental outcome are highest in these infants. This is considered further in Chapters 8 and 72.