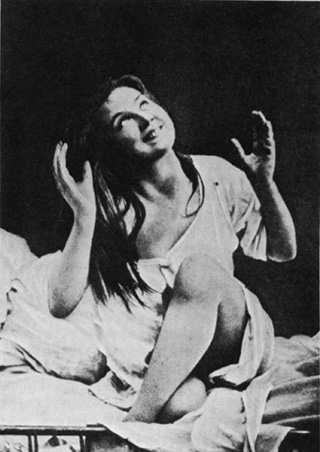
It was Jean-Martin Charcot (1825–93), the august Professor of Pathological Anatomy and later of Diseases of the Nervous System of the Paris Medical Faculty, the leading international neurologist of the nineteenth century, who made hysteria a spectacle and a circus. It was a scandalous circus that attracted the attention of tout Paris, one that regularly featured scantily clad women disporting themselves in unmistakably erotic cataleptic poses, or writhing and moaning in ways that mimicked orgasms on a public stage, before an understandably rapt audience—an audience soon drawn not just from the highest ranks of French society, but also from those attracted to Paris by news of these extraordinary Leçons du Mardi. The photographs of these occasions, captured in carefully staged arrangements before the supposedly objective lens of the camera and thus transmuted into indelible visual representations for a vastly greater virtual audience, have survived for later generations to inspect, and have become the iconic images of a disorder seen as at once sexual and feminine.
Yet Charcot thought of himself, and was acknowledged by his contemporaries, to be no nineteenth-century Mesmer, no marginal charlatan catering to depraved appetites (among patients and audience alike), but on the contrary a sober scientist, a man of genius, one of the leading contributors to the newly emerging science of the brain. His accomplishments first in internal medicine and then as a neurologist were legion, and had brought him czars and princes, great merchants and bankers, as his clients, in the process making him a very rich man. And, while his most famous hysterical patients were women, he personally insisted, as Willis and Sydenham had done two centuries earlier, that hysteria was not solely a female malady, but, on the contrary, could be diagnosed and detected among the male of the species. Hysteria was, he confidently declared, a disorder of the nervous system, not of the female reproductive organs. It was, moreover, as real and as somatic a disease as any of the other neurological catastrophes he had earlier elucidated.
Charcot had been born in humble circumstances, the son of a wagon-maker. He rose to eminence through the competitive examination system that Napoleon had introduced to the French in the aftermath of the Revolution, a poor boy made good. Along the way, he secured a position at the Salpêtrière, a vast warren of buildings on the edge of Paris that Louis XIV had made into “the Versailles of pain,” a receptacle for the (female) sweepings of the city: beggars, adulteresses, prostitutes, the depraved, those afflicted with venereal diseases, the senile, and the insane. An appointment to run some of the dilapidated wards in what Charcot himself called this “great emporium of human misery” might not have seemed a stroke of good fortune, but so it proved to be. For the Salpêtrière’s inhabitants made up an unrivaled collection of neurological specimens, together constituting what he called “a sort of living pathological museum [une sorte de Musée patholigique vivant] whose resources are almost inexhaustible.”1 It was a museum to which Charcot had privileged access, and it was on this foundation that he constructed his career and worldwide fame.
Charcot had been well trained in the clinico-pathological tradition that had emerged in the Paris hospitals in the early nineteenth century, a then-revolutionary approach to disease and debility that emphasized a localized pathology, and the correlation of ante-mortem signs and symptoms with post-mortem findings. Of necessity, this new hospital medicine required a constant supply of patients who would soon turn into corpses, for it was this never-failing availability of previously examined bodies that allowed the comparison of the living and the dead. This inspection in its turn allowed the clinician to uncover the lesions that had produced the earlier signs and symptoms, thus permitting the construction of authoritative portraits of particular diseases. What to the lay outsider must have looked like one of the least desirable portions of Dante’s Inferno was for Charcot a living museum of pathology, and, as its specimens ceased breathing, their poor and friendless status ensured that he had at his disposal the means to investigate and catalogue a vast spectrum of neurological complaints. And, since his appointment lasted decades, he could even follow the sometimes remitting and always complex natural history of neurological illnesses over extended periods of time. From a place to store the stigmatized and unwanted, the Salpêtrière was thus transformed into “a Temple of Science.”
To be sure, it took talent, energy, ambition, and drive to take advantage of these circumstances, but these Charcot possessed in abundance. Through the 1860s, he and his students labored doggedly at their task. By the end of the decade, Charcot could claim credit for a whole string of diagnostic distinctions and clinical advances. Attending only to his neurological triumphs, he had identified disseminated multiple sclerosis; aphasia; amyotrophic lateral sclerosis (for the French, “Charcot’s disease”; for Americans, since the 1930s, Lou Gehrig’s disease, after the great baseball player who died from it); locomotor ataxia (a complication of tertiary syphilis, as would become apparent in the early twentieth century); Tourette’s syndrome (named for one of Charcot’s assistants); Charcot-Marie atrophy; and chorea. These were but the most striking of his accomplishments, a series of scientific triumphs that cemented his reputation at the very peak of neurology, and made his word law. If Charcot diagnosed the patient’s disorder, the matter was settled, and it was the vast reservoir of authority he derived from his expertise in these dismal diseases of the nervous system that gave him license to pronounce and pontificate on the puzzles of hysteria/ mysteria, and to assert that here was another in the array of largely incurable diseases of the nervous system.
Many French physicians were loathe to admit hysteria to the status of a legitimate disease. Acknowledged as “a wastepaper basket of medicine where one throws otherwise unemployed symptoms,”2 to use the words of the Parisian alienist Charles Lasègue, it was for many doctors a highly suspect category. In the contemptuous language of another physician at the Salpêtrière, Jules Falret, the women who purported to suffer from hysteria were
veritable actresses; they do not know a greater pleasure than to deceive … all those with whom they come in touch. The hysterics who exaggerate their convulsive movement … make an equal travesty and exaggeration of the movements of their souls, their ideas, and their acts … in a word, the life of the hysteric is nothing but one perpetual falsehood; they affect the airs of piety and devotion, and let themselves be taken for saints while at the same time abandoning themselves to the most shameful actions; and at home, before their husbands and children, make the most violent scenes in which they employ the coarsest and often most obscene language and give themselves up to the most disorderly actions.3
Acting, deception, shameful and perpetual falsehood, these are descriptors that are redolent of moral disgust and condemnation, not the neutral tones of the clinician confronting biological infirmity. Charcot, by contrast, was insistent that hysteria was a genuinely organic disorder, a disease rooted firmly in the higher nervous system, and in these respects part of the broader spectrum of neurological disorders.
At first blush, such assertions seem, and must have seemed, paradoxical. Charcot had done more than any of his contemporaries to map out the disorders and lesions of the nervous system, and the tics, the anesthesias, the seizures, and paralyses that were such central elements in hysterical attacks were defined precisely by their failure to correspond to the anatomical realities, the physical topography of the body. Before Charcot, for example, it had been commonplace to confuse the tremblings of the victims of Parkinson’s disease with those of multiple sclerosis. Through careful comparison he had distinguished the two, and linked the tremors of multiple sclerosis to distinctive anatomical lesions of the spinal cord that were observable postmortem. This work involved matching precise clinical observations of patients to what he observed at autopsy, irregular, grey, sclerotic patches that were nonetheless sharply distinguished from adjacent structures and were “disseminated without any apparent rule, and as if at random, over all points of the [spinal] cord”; and then uncovering the distinctive microscopy of the disease. Later, he would correlate similar plaques on the brain to the disorders of vision, speech, and intellect that may manifest themselves as part of the natural history of the disease.
It was precisely on the ability to make increasingly fine diagnostic (and prognostic) distinctions that neurologists’ authority rested, for then, as now, virtually all these neurological disasters were incurable. As the man who had done most to establish the foundations on which the emerging specialty rested its claims to expertise, Charcot enjoyed prestige and professional standing that were without peer. His intellectual pre-eminence, together with the near-autocratic power he came to possess over access to elite positions in the French medical establishment, allowed him to stifle most dissent, and secure overt allegiance to his claims about hysteria, at least during his lifetime.
By contrast with those of multiple sclerosis, the patterns of the observed symptoms in cases of hysteria reflected lay and common-sense understandings of how the body was put together, but explicitly contradicted what professional, specialized knowledge had shown those connections and linkages to be. Hysterical deficits were, more often than not, neuroanatomical impossibilities. Yet Charcot invoked and invested his prestige and standing as “the Napoleon of the neuroses” to insist on their bodily reality. They were, he acknowledged, “morbid states, evidently having their seat in the nervous system, which leave in the dead body no material trace that can be discovered.” Hysteria did not stand alone in this regard: epilepsy and the choreas (degenerative nervous disorders characterized by spasmodic movements of the face, body, and limbs, and a loss of coordination) also “deny the most penetrating anatomical investigations.” All these neurological diseases, in consequence, “do not present themselves to the mind of the physician with that appearance of solidity, of objectivity, which belong to affections connected with an appreciable organic lesion.”4 And yet, Charcot insisted, they were indeed disorders of the nervous system, just as much as multiple sclerosis and the rest. Hysteria, in particular, which some sought to banish “into the category of the unknown,” was the product of an underlying hysterical diathesis, and belonged without question to the same family as the many diseases of the nervous system he had already dissected.
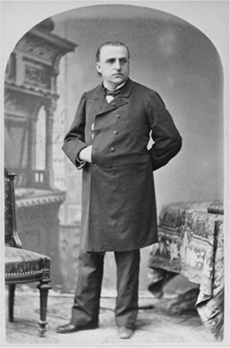
9. Jean-Martin Charcot (1829–93) obviously took his nickname “the Napoleon of the Neuroses” quite seriously. He gave this portrait to his acolyte, Sigmund Freud, with a note in his own hand, on Freud’s departure from Paris on February 24, 1886. A precious possession, it was carefully preserved among Freud’s effects. (Freud Museum, London)
Though his primitive microscopes could detect no lesions on which to pin the disease, hysterical patients, for Charcot, displayed the next best thing: physical stigmata revelatory of the underlying inherited physical inferiority that gave birth to their symptoms. There was an overlooked circularity here: the headaches, the visual problems, the (sometimes migrating) loss of sensation on one side of the body (hemianesthesias), the convulsive fits that resembled (but were clearly not) epileptic seizures, and that Charcot would label “la grande hystérie”—these were at once the signs that signaled the presence of an inherited set of physical deficiencies, and the basis on which hysteria could be diagnosed. Ovarian tenderness, too, marked the female patients out, a sign of the continued hold reflex theory had on Charcot’s thinking. Applying pressure on a hysterical woman’s ovaries by pushing down on her abdomen could modify the symptoms she displayed, just as, Charcot discovered, squeezing a hysterical male’s testicles might provoke changes in his behavior and still greater convulsions. In the case of one 16-year-old girl, for example, pressure on her abdomen in the “ovarian” region had dramatic effects:
Immediately an attack of rhythmic chorea breaks out. The patient remains sitting and her consciousness is preserved. Her head begins suddenly to turn from right to left, and then from left to right, in rhythmic alteration with equal pauses between the individual movements. Simultaneously, the right arm begins going up and down, as a result of which her right hand beats regularly on her knee as though on a drum. The movements of the hand are synchronized with those of the head. Meanwhile the right foot is stamping noisily on the floor. There are approximately 100 beats of the foot and three times as many of the hand in a minute.5
Beyond the echoes of reflex theory such examples conjure up, the emphasis on a defective physical constitution was a variation of the theories of degeneration as a cause of crime, alcoholism, violence, and madness. The concept of degeneration was broadly embraced in the last third of the nineteenth century—nowhere more enthusiastically than among asylum doctors, for whom this ideology at once provided a new legitimation for the mental hospital, and an explanation for their failure to deliver on their earlier promises of cure. For Charcot, such notions provided indispensable support for his assertions about hysteria’s organicity.
Two factors were of particular importance in directing steadily more of Charcot’s attention to the problem of hysteria. First, he was given authority in 1870 over yet another ward in the Salpêtrière, a space for thirty patients where epileptics and hysterics were clustered together, and where, almost by osmosis, the hysterical patients seemed to have acquired a propensity for major fits. Though this was scarcely Charcot’s first encounter with either disorder, the combination fascinated him, and drew him away from the study of the scleroses and related disorders, and more and more towards an interest in what he first termed “hystero-epilepsy,” and would later dub “la grande hystérie” or “hystérie major.” Secondly, there was his late 1870s embrace of “hypnosis,” the term James Braid had invented in 1843 in an effort to detoxify the odors of quackery that had enveloped mesmerism. For Charcot, the use of hypnosis led directly to the apotheosis of his Tuesday spectacles, the ever more elaborate display of the pathologies of his hysterical patients that brought him such large and entranced audiences. Earlier in the 1870s, the audience for his lectures had been small and purely professional, some fellow physicians and a handful of interns. His hypnotic séances soon multiplied their numbers many times over, broadening their appeal and attracting a host of the laity.
Again, we seem to enter an Alice-in-Wonderland world. For surely the basis of the hypnotic trance is suggestion, the manipulation of psychological states? Not for Charcot, nor, it should be said, for Braid himself, at least when he initially coined the term. And not for Charcot’s British contemporaries, who, like him, claimed that only the biologically susceptible—that is, the hysterical—could be hypnotized. Part of Braid’s break with mesmerism, and of his attempt to reclaim the technique for medicine, had been his rejection of Mesmer’s doctrine of “animal magnetism,” and his insistence that what occurred in hypnosis was a change in cerebral circulation, the provoking of a changed state of the nervous system analogous to what one saw in sleep. It was, he insisted, “merely a simple, speedy, and certain method of throwing the nervous system into a new condition …”6 For Charcot, and his counterparts across the Channel, it was a bit more than that: it was a technique that could work only when practiced upon the defective—indeed, to be hypnotizable was to reveal oneself as a hysteric, to make manifest an underlying diseased state of the entire organism. Hypnotism and hysteria, in Michael Clark’s felicitous summary, were “closely related states of mental and moral [and I would add, physical] degeneracy.”7 The inherited weakness created a prodigious predisposition to the disease, which was then typically triggered by trauma—an accident, violence, perhaps even by the presence of another hysteric, when the hysterical manifestations might multiply and travel from patient to patient, in a veritable epidemic of mass hysteria.
At their core, Charcot’s dazzling displays of his hysterical patients were flamboyant, dramatic occasions. The Great Man was, as Ruth Harris notes, “ruthlessly insensitive to the pain and anguish of his patients, and so enamoured of his scientific mission that he dispensed with ethical proprieties when presenting them to the public.”8 Those who were at the center of a particular week’s lecture were brought on to the stage, to be examined, poked and prodded, hypnotized, all-but-anatomized by the professor himself, their foibles and physical contortions made the centerpiece of the week’s entertainment and instruction.
Sometimes, the drama had a rapid and satisfying conclusion. There was the case of Henriette A., for example, a laundress whose hysteria, like that of many of Charcot’s patients, seemed to have its origins in a traumatic incident; in this case she had suffered a glancing blow on the head from a falling bookshelf. The accident left her agitated but apparently unhurt, but a day later, she had suffered a fall, which was soon followed by a developing paralysis of her right arm. In Charcot’s hands, the upshot was an almost instantaneous cure, a piece of magic carried out in front of an enthusiastic crowd, and climaxing with Henriette prancing “round among the audience vigorously shaking them by the [right] hand, desirous of proving how real was the recovery they had just witnessed.”9
But this was a simple case. Others proved far more challenging, and incapable of real amendment. As he had earlier done with cases of multiple sclerosis, Charcot was determined to explore the natural history of hysteria, its characteristic forms and its development over time. All his efforts to localize hysteria in the morgue met with frustration, so he turned to the shifting kaleidoscope of symptoms with which his parade of patients provided him, and sought to produce order from the apparent chaos. A classificatory schema, a sequence of stages through which all patients passed, these were what he thought he detected, and what in reality he manufactured.
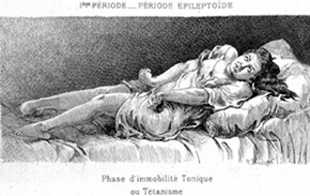
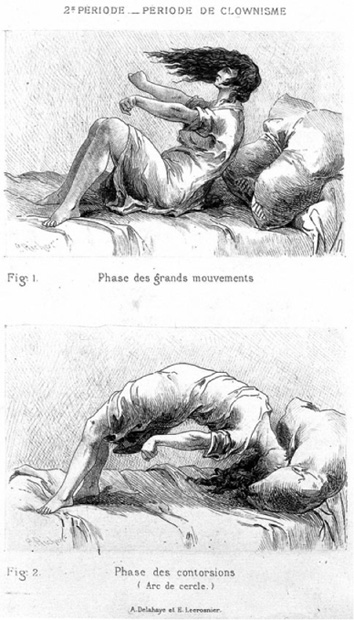
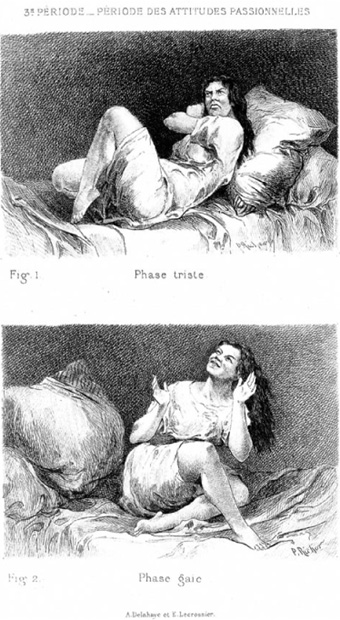
Hysteria, Charcot pronounced, had four distinct stages, “four periods [that] succeeded each other in the complete attack with mechanical regularity.” There was first an epileptoide period, where the patient suffered fits. In the next phase, the “period of contortions and grands mouvements,” as its name implies, the patient engaged in dramatic physical displays, often accompanied by cries and shrieks, and culminating in some cases in the adoption of an arc-en-cercle position, in which the patient bent backwards into a seemingly impossible contortion, with only the back of the head and the heels still touching the ground. Charcot also referred to these episodes as clownisme. Then, especially in female patients, there was a phase where the patient adopted attitudes passionelles, posing as if being crucified, or in the throes of erotic ecstasy.10
In the final or terminal phase of delirium, the patient might experience hallucinations or delusions, which gradually subsided. “What I want to emphasize,” Charcot insisted in 1882, “is that in the [hysterical] fit, nothing is left to chance, that to the contrary everything unfolds according to the rules, which are always the same and characterize what we see in outpatients as well as inpatients; they are valid for all countries, for all epochs, for all races, and are, in short, universal.”11 And, of course, it was that universality, that regularity, that lent weight to his contention that hysteria was an organic disease of the nervous system—except that the regularity and the universalism were manufactured, socially constructed by Charcot’s assistants and their pliable specimens, though the mise en scène took place behind Charcot’s back, and in all probability without his knowledge.
10. The first phase of Charcot’s grand hystérie. The patient, having suffered a seizure, is locked into a tonic immobility, arms rigid, nightgown rucked up. (Wellcome Library, London)
11. Clownisme, Charcot’s second stage of a hysterical attack. The bottom plate shows the characteristic arc-en-cercle adopted by many of his patients. (Wellcome Library, London)
12. Attitudes passionelles, the third phase of grand hystérie. Engravings based on one of many photographic studies of the female patients who made up Charcot’s circus. (Wellcome Library, London)
Charcot was, however, fully conscious of the possibility of simulation, and aware that those who rejected his claims about the reality of hysteria saw the patients as malingerers and fakes. “Here is an element,” he acknowledged, “that we meet with at each step … of this neurosis, and which throws (there is no use in denying it) a certain amount of disfavor on the studies which are connected with it. But,” he went on, “is it really as difficult as some appear to believe, to discern the real symptomatology from the imaginary? By no means.”12 One could, as Charcot proceeded to do, devise experiments to demonstrate the distinction. Hysterics in the cataleptic phase, for example, might keep an arm extended for an extraordinary amount of time, and instruments could be used to trace the least oscillations of the outstretched limb, documenting a difference between the true hysteric and the person who was merely simulating the disorder. “A hundred other examples,” he triumphantly concluded, “might be invoked which would only show that the simulation, which is talked about so much when hysteria and allied affections are under consideration, is, in the actual state of our knowledge, only a bugbear, before which the fearful and novice alone are stopped.”13
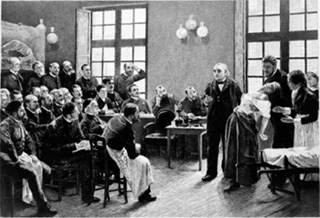
Charcot had his favorites, those who returned time and again to put on multiple, often increasingly elaborate, performances. None was more famous than Blanche Wittman, the queen of hysterics, a performer who luxuriated in her role. Perhaps the most famous single image of a hysterical patient is an 1887 painting by André Brouillet that captures Charcot presenting Blanche, his pet hysteric, to members of his neurological service. She swoons over the outstretched arm of his assistant, Joseph Babinski, her pelvis thrust forward, her breasts barely covered by her blouse and pointing suggestively toward the professor, her head twisted to the side and her face contorted in what looks like the throes of orgasm. (Freud kept a copy of this painting, which dates from 1887, in his study in Vienna, and again in London.)
Wittman was admitted to the Salpêtrière in 1878, and remained there for some sixteen years, performing on command. After her discharge, she became Marie Curie’s laboratory assistant, and eventually was poisoned by the radium she was working with. In consequence, both legs and her left arm had to be amputated. Then there was Augustine, admitted to the Salpêtrière in 1875 at 15a½,
13. Blanche Wittman (1863–1913), the “queen of hysterics,” in the archetypical portrait of Charcot demonstrating a case of hysteria before a rapt audience. (Wellcome Library, London)
tall, well-developed (neck a bit thick, ample breasts, underarms and pubis covered with hair), with a determined tone and bearing, temperamental, noisy. No longer behaving in the least like a child, she looks almost like a full-grown woman, and yet she has never menstruated. She was admitted for paralysis of sensation in her right arm, preceded by pains in her lower right abdomen.14
She had, we now know, been threatened with a razor and raped by her mother’s lover when only 13, and sexually attacked by other men in her neighborhood. Once in the hospital, she was stripped and displayed, physically and emotionally laid bare, photographed incessantly in diaphanous and revealing hospital gowns for the multi-volume Catalogue of images that constituted the Iconographie and the Nouvelle Iconographie of the Salpêtrière, Augustine would play a starring role in the circus for five years, till, one day in September 1880, she abruptly stole away, disguised (and this sealed her status as a Surrealist and then a feminist icon) as a man, never to be heard from again.
14. Augustine, before she stole away from the Salpêtrière. Frequently caught by the camera lens in erotic poses, here she poses half naked in a state of extase, or ecstasy.
But the supporting cast grew ever more numerous, and the audience steadily larger and more heterogeneous. Axel Munthe has provided us with a vivid reconstruction of the scene, one he himself observed and participated in. Out beyond the stage, “the huge amphitheatre was filled to the last place with a multicoloured audience drawn from tout Paris, authors, journalists, leading actors and actresses, fashionable demimondaines”—all gathered for the show. Now came the performers, the grey-coated, sombre Charcot, the master of ceremonies for the proceedings, and then the women who would do his bidding, apparently under the influence of the hypnotic trance:
Some of them smelt with delight a bottle of ammonia when told it was rose water, others would eat a piece of charcoal when presented to them as chocolate. Another would crawl on all fours on the floor, barking furiously when told she was a dog, flap her arms as if trying to fly when turned into a pigeon, lift her skirts with a shriek of terror when a glove was thrown at her feet with a suggestion of being a snake. Another would walk with a top hat in her arms rocking it to and fro and kissing it tenderly when told it was a baby.”15
The masculine dominance, the foolishness and frailty of the female, both were decisively on display.
The Iconographies, the collections of photographs of the performers who made up the circus, circulated widely and disseminated the Charcotian vision of hysteria to an audience who could only virtually witness the Parisian scene. They did much to fix the image of hysteria in the public mind, and perhaps to spread suggestively what purported to be neutral, naturalistic recordings of a neuropathic disorder. The photograph (at least before the age of digital manipulation) carried the illusion of providing the truth, a direct and unmediated portrait or even a mirror of nature, the instantaneous representation of what passed before the lens of the camera. But the limitations of lighting, and the technical requirements of picture-taking with wet collodion plates, or even the later silver gelatino-bromide coating, made for long exposures, sometimes as long as twenty minutes per plate. Perhaps appropriately, given that Charcot’s posthumous critics (whom, as we shall see, included even—in fact, especially—his collaborators and protégés) viewed his clinical demonstrations as fraudulent, the “objective” photographs that recorded the pathologies were themselves necessarily staged, posed, and manufactured constructions whose status as “facts” is as slippery as the live demonstrations they purport to record.
Charcot was not alone in exploiting his patients, in treating them as so many specimens rather than as suffering human beings. The disdain and the callousness were a feature of the whole clinico-pathological tradition, something that American medical students visiting Paris for instruction viewed with dismay as early as the 1830s. As feminist historians focused their attentions on hysteria as a female complaint, and perhaps the product, as some of them speculated, of an inchoate, inarticulate protest against the roles in which Victorian women were imprisoned, Charcot’s serial exploitations of these poor creatures, his willingness to expose them repeatedly to the prurient gaze of his audience at whatever cost to their emotional well-being, drew fierce criticism and reproof. But those same moral failings were visible to Charcot’s contemporaries, and were the subject of bitter commentary, even from literary figures such as Tolstoy and de Maupassant. A Madame Renooz, in the pages of the Revue scientifique des femmes, protested about his “sort of vivisection of women under the pretext of studying a disease for which he knows neither the cause nor the treatment.”16 And across the Channel, another critic condemned the
disgusting experiments practiced on lunatics and hysterical patients in the Salpêtrière. The nurses drag these unfortunate women, notwithstanding their cries and resistance, before men who make them fall into catalepsy. They play on these organisms … on which the experiment strains the nervous system and aggravates the morbid conditions, as if it were an instrument … One of my friends told me that she … had seen a doctor of great reputation make one unhappy patient pass, without transition, from a celestial beatitude to a condition of infamous sensualment. And this before a company of literary men and men of the world.17
And yet Charcot, as the feminist historian Elaine Showalter acknowledges, cannot be easily typecast as a crude misogynist, for he adopted liberal positions by the standards of his time on women’s rights, and his students and externs included women training for the medical profession. Moreover, one of Charcot’s more striking departures from the conventional wisdom of his time had been his insistence that hysteria was not just a female disease. Earlier proponents of a neuropathic etiology for hysteria, such as Willis and Sydenham, had made this point in the late seventeenth century, but reflex theory had created a new way of re-emphasizing the connections between women’s reproductive organs, their brains, and their propensity to be hysterical. Thomas Laycock, writing in 1840, had drawn upon such ideas to reassert that “hysteria is peculiar to females” because it is “the nervous system of the woman which is implicated in these affections.”18 And some decades later, Beard’s invention of neurasthenia, while not precluding men from being diagnosed with hysteria, had created an alternative diagnostic label many physicians used disproportionately for men.
Charcot, on the other hand, controversially insisted on emphasizing that hysteria afflicted males as well as females. His colleague Pierre Briquet of the Hôpital de la Charité in Paris had made similar claims in 1859, arguing against those who had used reflex theory to relink hysteria to women’s reproductive organs, and Charcot acknowledged his debt to Briquet many times in lectures and in print. Charcot had opened a ward for hysterical males at the Salpêtrière, in 1882, the first accommodation for men that the vast hospital had ever made, and male patients had also attended his out-patient clinics from 1878 onwards. Beginning in the 1880s, perhaps a quarter of his published discussions of hysteria focused on men, and his contradiction of the traditional view that hysteria was a female disorder drew widespread attention.
Although the claim that masculine hysterics existed was certainly not new, generally such cases had been ignored or marginalized. Often, when they were recognized as such, hysterical males had been dismissed as effeminate, sedentary, and studious. Many of Charcot’s male patients, by contrast, were drawn from the laboring classes and were muscular, virile men—in his words “vigoreux, solide, non énervé par la culture.”19 They included train drivers, plumbers, bakers, blacksmiths, and the like. Earlier generations, Charcot insisted, had simply misdiagnosed such cases, whereas modern medical science (in whose vanguard, of course, he stood) had finally grasped their true nature. As with his female hysterics, Charcot emphasized the neuropathic origins of these men’s disorders, and, in parallel fashion, it was the men’s hemianesthesias and their paralyses, their contractures and their seizures, rather than their psychological disturbances, that were the primary focus of his attentions. Just as American neurologists had dismissed the efforts of gynecologists to trespass on neurological territory, so these emphases in Charcot’s theorizing not so coincidentally cut the ground out from under French gynecologists who were tempted to endorse ovariotomies as a cure for hysteria.
Charcot’s emphasis on the prevalence of hysteria among men of the artisanal and working classes reflected a more general way in which his writings on hysteria departed from most prior orthodoxy. Where standard discussions had tended to stress the connection between nervous disorders and affluence, and this claim was as clear in Cheyne’s remarks on the English malady as in Beard’s commentary on American nervousness, Charcot’s female patients at the Salpêtrière were almost all drawn from the lower orders. For both sexes, therefore, he was led to acknowledge that previous discussions of hysteria’s social location had gone badly astray. “We must not forget,” he commented with some asperity,
that the psychological constitution [of the working class] is fundamentally the same as ours, and that, perhaps even more than other people, they are subjected to the destructive effects of painful moral emotions, of anxieties related to the material difficulties of life, to the depressing influence of the exaggerated effect of physical forces … In addition, we should remember that neuropathic heredity is scarcely the exclusive privilege of the wealthy in life. It extends its reach to the working class as to everywhere else.
Hysteria, not surprisingly, may thus “be observed on a grand scale among the workers and artisans, by those the least favored by fate and who scarcely know anything other than hard manual labor.”20
Among patients with an inherited hysterical diathesis, it took only a precipitating event to bring about a full-blown hysterical attack. Alcohol was one such precipitant, especially among the lower orders. But so were industrial accidents and other traumatic incidents, railway accidents being one of the most common of these, both for Charcot, and for those trying to trace the etiology of the disorder elsewhere in Europe and North America. Here, Charcot verged on accepting the notion that ideas and emotions could be sufficient to precipitate a breakdown, though it was a model of how hysteria might materialize that he could never fully bring himself to accept. Understanding hysteria in terms of the “conversion” of the psychological into the physical was a move that would be left to others.
One of the hallmarks of the French academic system, and in many ways one of its great weaknesses, was its hierarchical and hyper-centralized character. (In this respect it mimicked the larger society that had spawned and supported it.) Those who stood at the head of the system could lord it over all beneath them, and no one more so than Charcot. Like many a poor boy made good, he liked nothing better than to mingle with the rich and the powerful.
His marriage to a wealthy widow, combined with the robust clinical income secured by his growing reputation, allowed him to purchase both a villa in the affluent suburb of Neuilly-sur-Seine and an elegant mansion, 217 Boulevard Saint-Germain, and to furnish both with tapestries, paintings, rare books, antiques, even stained-glass windows. His bookshelves, for example, were modeled on those found in Florence in the library of the Medicis in the Convent of San Lorenzo, and his collection of classical and Renaissance art provided him with an array of paintings depicting the visions and ecstasies of saints, portraits he delighted in reinterpreting as instances of undiagnosed hysteria. Charcot’s intellectual fortunes were in important ways linked to the fiercely anti-clerical politics of the Third Republic. His chair of nervous diseases, for example, had been pushed through the National Assembly by his prominent political friend Léon Gambetta. How better to return the favor, to tweak the forces of religious reaction, and to discredit the most sacred characters of Christian martyrdom, than by declaring them to be a collection of specimens of mental pathology, mere deluded hysterics?
In the splendid setting of his city mansion, Charcot held regular soirées on Tuesdays after his public lectures, glittering affairs that brought together writers and poets, journalists and architects, statesmen and scientists, the occasional cardinal and the elite of the medical profession. Such figures were powerful allies, adding to the immense authority Charcot had already derived from his chair at the Paris medical faculty and from his increasingly global prominence. By the 1880s it was plausibly asserted that all appointments to the medical faculty required his imprimatur, an influence that he was not in the least shy about exercising.
What made this concentration of power the more dangerous was that Charcot was notoriously thin-skinned—allergic, not just to criticism, but even to minor forms of dissent among his underlings. To court the professor’s displeasure was to invite severe damage to one’s prospects, even professional ruin. Those who feared or had felt his wrath might take their revenge through the traditional subterranean tactics of the weak: damaging the careers of his protégés, for instance, when they could do so without fear of detection (as when Charles Bouchard, a rival neurologist, placed the young Joseph Babinski at the bottom of the aggrégation list, ensuring that the most talented French neurologist of his generation could never achieve the rank of professor); but seldom or never daring to confront him directly. In the words of Léon Daudet, the son of one of Charcot’s closest friends, the great professor “could not stand contradiction, however small. If someone dared to contradict his theories, he became ferocious and mean and did all he could to wreck the career of the imprudent man unless he retracted and apologized.”21 On a broader canvas, he was envious of others’ successes, and, according to the Goncourt brothers, showed “a ferocious resentment against those who declined invitations to his receptions.”22
The salutary correctives that close associates, or even independent rivals, might have on the great man’s wilder fancies were thus notable for their absence. Charcot found himself surrounded by yes-men and mediocrities, and those too frightened to speak out. Not only did this heighten the danger that his views might become entrenched in increasingly dubious and indefensible positions, but, as the sycophantic scurried to secure his favor, it actually encouraged them to stage performances for his benefit—fraudulent events that lent apparent intellectual support to increasingly suspect claims. In the final years before his death, even Charcot had begun to question whether there was not indeed a strong psychological component to hysteria, though for the most part he remained convinced of its organic roots. (In any event, it was an article of faith with Charcot that the realm of the psychological would ultimately prove reducible to cerebral physiology.) With his demise, however, the whole Charcotian edifice came rapidly crashing down.
In tribute to the great man, there was a project to publish his complete works, but it was soon abandoned and never revived, with only nine of a projected twenty-six volumes ever appearing in print. His long-cowed pupils now dared to voice their dissent, and men like Babinski and Déjerine (who succeeded to Charcot’s chair in 1911) were soon distancing themselves from the legacy of their maître, and denying the reality of the dramas they had once had so large a hand in staging. Babinski made his intellectual break with his patron clear by moving, in 1901, to do away with the label of “hysteria” altogether, and to replace it with a term of his own coinage, “pithiatism.” Déjerine waited only a little longer. “It now seems certain,” he said, almost two decades after his patron was safely in the grave, “that the crises delineated by this description [la grande hystérie] are nothing other than coaching [dressage] and imitation.”23 Axel Munthe was more biting yet:
these stage performances of the Salpêtrière before the public of Tout Paris were nothing but an absurd farce, a hopeless muddle of truth and cheating. Some of these subjects were no doubt real somnambulists faithfully carrying out in a waking state the various suggestions made to them during sleep—posthypnotic suggestions. Many of them were mere frauds, knowing quite well what they were expected to do, delighted to perform their various tricks in public, cheating both doctors and audience with the amazing cunning of the hystériques. They were always ready to piquer une attaque of Charcot’s grande hystérie, arc-en-ciel and all, or to exhibit his famous three stages of hypnotism: lethargy, catalepsy, somnambulism, all invented by the Master…24
All that for decades had seemed so solid melted into air. The very term “hysteria” vanished with astonishing rapidity from the French scene, and the epicenter of the hysterical imperium moved hundreds of miles to the east and south, to the hothouse, sexualized atmosphere of fin-de-siècle Vienna. As early as 1900, Charcot’s star had firmly set.