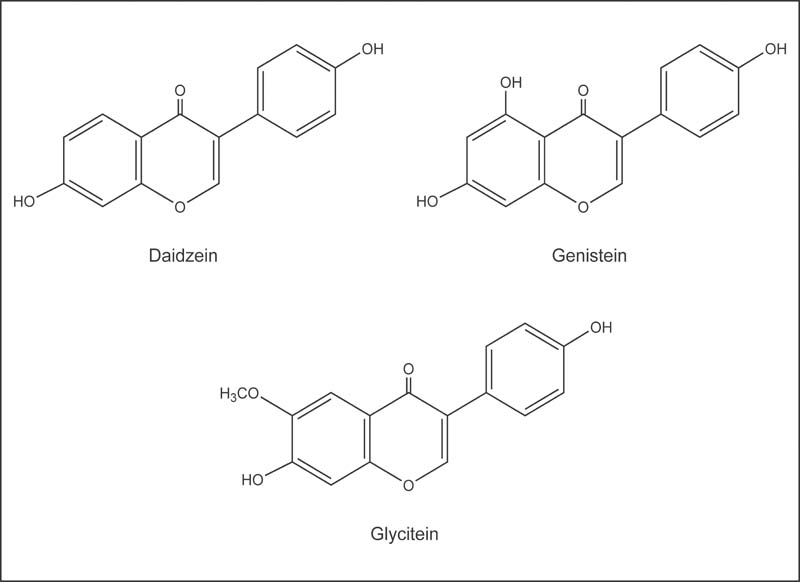
Fig. 12.1 Chemical structures of the soy isoflavones, daidzein, genistein, and glycitein, in their aglycone forms.
Isoflavones are polyphenolic compounds that are capable of exerting estrogen-like effects. For this reason, they are classified as phytoestrogens—plant-derived compounds with estrogenic activity.1 Legumes, particularly soybeans, are the richest sources of isoflavones in the human diet. In soybeans, isoflavones are present as glycosides (bound to a sugar molecule). Fermentation or digestion of soybeans or soy products results in release of the sugar molecule from the isoflavone glycoside, leaving an isoflavone aglycone. Soy isoflavone glycosides are called daidzin, genistin, and glycitin; the aglycones are called genistein, daidzein, and glycitein, respectively (Fig. 12.1). Unless otherwise indicated, quantities of isoflavones specified in this article refer to aglycones—not glycosides.
The biological effects of soy isoflavones are strongly influenced by their metabolism, which is dependent on the activity of bacteria that colonize the human intestine.2 For example, the soy isoflavone daidzein may be metabolized in the intestine to equol (Fig. 12.2), a metabolite that has greater estrogenic activity than daidzein, and to other metabolites that are less estrogenic. Studies that measure urinary equol excretion after soy consumption indicate that only approximately 33% of individuals from Western populations metabolize daidzein to equol.3 Thus, individual differences in the metabolism of isoflavones could have important implications for the biological activities of these phytoestrogens.
Fig. 12.1 Chemical structures of the soy isoflavones, daidzein, genistein, and glycitein, in their aglycone forms.
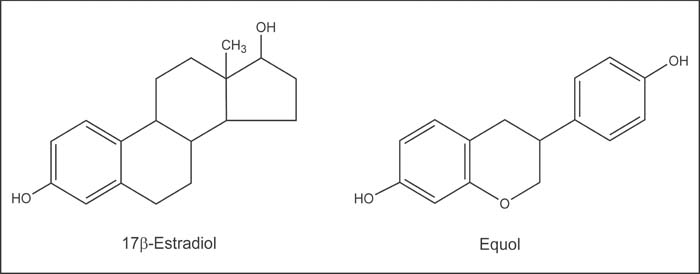
Fig. 12.2 Chemical structures of 17 β-estradiol, an endogenous estrogen, and equol, a bacterial metabolite of daidzein that has estrogenic activity.
Soy isoflavones are known to have weak estrogenic or hormone-like activity. Estrogens are signaling molecules that exert their effects by binding to estrogen receptors within cells. The estrogen–receptor complex interacts with DNA to change the expression of estrogen-responsive genes. Estrogen receptors are present in numerous tissues other than those associated with reproduction, including bone, liver, heart, and brain.4 Soy isoflavones and other phytoestrogens can bind to estrogen receptors, mimicking the effects of estrogen in some tissues and antagonizing (blocking) the effects of estrogen in others.5 Scientists are interested in the tissue-selective activities of phytoestrogens because antiestrogenic effects in reproductive tissue could help reduce the risk of hormone-associated cancers (breast, uterine, and prostate), while estrogenic effects in other tissues could help maintain bone density and improve blood lipid profiles (cholesterol levels). The extent to which soy isoflavones exert estrogenic and antiestrogenic effects in humans is currently the focus of considerable scientific research.
Soy isoflavones and their metabolites also have biological activities that are unrelated to their interactions with estrogen receptors.6 By inhibiting the synthesis and activity of certain enzymes involved in estrogen metabolism, soy isoflavones may alter the biological activity of endogenous estrogens and androgens.7–9 Soy isoflavones have also been found to inhibit tyrosine kinases,10 enzymes that play critical roles in the signaling pathways that stimulate cell proliferation. Additionally, isoflavones can act as antioxidants in vitro,11 but the extent to which they contribute to the antioxidant status of humans is not yet clear. Plasma F2-isoprostanes, biomarkers of lipid peroxidation in vivo, were significantly lower after 2 weeks of daily consumption of soy protein containing 56 mg of isoflavones than after consumption of soy protein providing only 2 mg of isoflavones.12 However, daily supplementation with 50–100 mg of isolated soy isoflavones did not significantly alter plasma or urinary F2-isoprostane levels.13,14
Although controlled clinical trials conducted prior to 1995 suggested that substituting 25–50 g/day of soy protein for animal protein lowered serum low-density lipoprotein (LDL) cholesterol by approximately 13%,15 more recent and better controlled trials indicate that the LDL-cholesterol-lowering effect of soy protein is much more modest. A review in 2000 of 22 randomized controlled trials concluded that substituting 50 g/day of soy protein for animal protein lowered LDL cholesterol by only approximately 3%.16 There is limited evidence that soy protein containing isoflavones is more effective than soy protein without isoflavones in lowering LDL cholesterol,17,18 but the consumption of soy isoflavones alone (as supplements or extracts) does not appear to have favorable effects on serum lipid profiles.16,19–21 For more information on soy protein and cholesterol, see Chapter 3.
The preservation of normal arterial function plays an important role in cardiovascular disease prevention. The ability of arteries to dilate in response to nitric oxide produced by the endothelial cells that line their inner surface (endothelium-mediated vasodilation) is compromised in people at high risk for cardiovascular disease.22 To date, results of randomized controlled trials on the effect of soy isoflavones on arterial function have been mixed. However, most placebo-controlled trials found no significant improvement in endothelium-mediated vasodilation when postmenopausal women were supplemented with up to 80 mg/day of soy isoflavones23–25 or up to 60 g/day of soy protein containing isoflavones.26–30 Arterial stiffness is another measure of arterial function. Measurements of arterial stiffness assess the distensibility of arteries, and a strong association between arterial stiffness and atherosclerosis has been observed.31 In placebo-controlled clinical trials, supplementing the diet of postmenopausal women with 80 mg/day of a soy isoflavone extract for 5 weeks significantly decreased arterial stiffness,32 as did supplementation of men and postmenopausal women at 40 g/day of soy protein, providing 118 mg/day of soy isoflavones for 3 months.29 Although most studies have not found supplementation with soy protein or isoflavones to improve endothelium-mediated vasodilation, preliminary research suggests that soy isoflavone supplementation may decrease arterial stiffness. However, a recent randomized, controlled, crossover trial in hypertensive individuals found that supplementation with soy protein containing 118 mg/day of isoflavones for 6 months did not improve measures of arterial function, including arterial stiffness.33 More research is needed to determine whether supplementation with soy isoflavones improves arterial function.
The incidence of breast cancer in Asia, where average isoflavone intakes from soy foods range from 25 mg/day to 50 mg/day,34 is lower than breast cancer rates in the Western countries where average isoflavone intakes in non-Asian women are less than 2 mg/day.35,36 However, many other hereditary and lifestyle factors could contribute to this difference. Epidemiological studies of dietary soy and breast cancer have reported conflicting results. A few studies suggest that a higher soy intake during adolescence may lower risk of developing breast cancer later in life.37,38 See Chapter 3 for more information about soy consumption and breast cancer risk. At present, there is little evidence that taking soy isoflavone supplements decreases the risk of breast cancer.
Because the development of endometrial (uterine) cancer is related to prolonged exposure to unopposed estrogens (estrogen not counterbalanced with the hormone progesterone), it has been suggested that high intakes of phytoestrogens with antiestrogenic activity could be protective against endometrial cancer.39 In support of this idea, three retrospective case–control studies found that women with endometrial cancer had lower intakes of soy isoflavones from foods compared with cancer-free control groups.39–41 However, giving soy protein supplements to postmenopausal women, providing 120 mg/day of isoflavones for 6 months did not prevent endometrial hyperplasia induced by the administration of exogenous estradiol.42 Although limited evidence from case–control studies suggests an inverse relationship between consumption of soy foods and endometrial cancer, there is no evidence from intervention trials that taking soy isoflavone supplements decreases the risk of endometrial cancer.
Mortality from prostate cancer is much higher in the United States than in Asian countries, such as Japan and China.43 However, epidemiological studies do not provide consistent evidence that high intakes of soy foods are associated with reduced prostate cancer risk. See Chapter 3 for more information about soy foods and prostate cancer risk. The results of cell culture and animal studies suggest a potential role for soy isoflavones in limiting the progression of prostate cancer.44 Although soy isoflavone supplementation for up to 1 year did not significantly decrease serum concentration of prostate-specific antigen (PSA) in men without confirmed prostate cancer,45–47 soy isoflavone supplementation appeared to slow the rising serum PSA concentration associated with prostate tumor growth in two small studies of patients with prostate cancer.48,49 One small, short-term (<1 month) study in patients with prostate cancer found that men randomized to receive a high-phytoestrogen diet experienced a statistically significant improvement in PSA concentrations compared with men randomized to receive a low-phytoestrogen diet.50 A trial of soy milk supplementation (141 mg/day isoflavones) in men with PSA-specific recurrent prostate cancer found that PSA levels increased by an average of 20% over a 12-month period compared with a 56% yearly increase prior to the study.51 A review published in 2006 found that isoflavone supplementation in prostate cancer patients favorably affected PSA concentrations in four out of eight trials.52 Additionally, a recent meta-analysis of eight studies found that consumption of isoflavones was associated with a reduction in risk of prostate cancer, but the association was not statistically significant.53 Although such preliminary findings are encouraging, the results of larger randomized controlled trials, which are currently ongoing, are needed to determine whether soy isoflavone supplementation can play a role in the prevention or treatment of prostate cancer.54
Although hip fracture rates are generally lower among Asian populations consuming soy foods than among Western populations, it is not yet clear whether increasing soy isoflavone consumption in Western populations helps to prevent osteoporosis.55 The results of short-term clinical trials (≤6 months) assessing the effects of increased soy intake on biochemical markers of bone formation and bone resorption are inconsistent. Some controlled trials in postmenopausal women have found that increasing intakes of soy foods, soy protein, or soy isoflavones improves markers of bone resorption and formation56–59 or attenuates bone loss,59,60 but other trials have found no significant benefit of increasing soy intake.61–64 Randomized controlled trials of longer duration are required to determine whether increased soy intake can actually prevent losses in bone mineral density (BMD) or osteoporotic fracture. Two controlled clinical trials found that BMD losses over 6 months were significantly lower in postmenopausal women given supplements of soy protein containing isoflavones than in those given supplements with equal amounts of milk protein,62,65 but two longer trials found that BMD loss did not significantly differ between postmenopausal women given supplements with soy protein containing isoflavones and those supplemented with milk protein.66,67 A 2-year clinical trial found that daily consumption of soy milk containing isoflavones significantly decreased BMD loss in the lumbar spine compared with daily consumption of soy milk without isoflavones,68 but three other studies found that BMD loss did not significantly differ between postmenopausal women taking soy protein supplements containing isoflavones and those taking soy protein supplements without or with negligible amounts of isoflavones.68–70 Loss of bone mineral content at the hip over 1 year was lower in Taiwanese women who took 80 mg/day of isolated soy isoflavones compared with placebo, but the difference was significant only in those women who were at least 4 years past menopause, had lower body weights, or had lower calcium intakes.71 Another study in Taiwanese women found that those taking 100 mg/day of isolated soy isoflavones for 1 year experienced less bone loss compared with the control group, but women taking 200 mg/day of supplemental isoflavones did not experience any benefit.72 Yet, a randomized controlled trial in European post-menopausal women found that supplementation with isoflavone-enriched foods (110 mg/day of isoflavones) for 1 year had no significant effect on BMD.73 A recent placebo-controlled trial in post-menopausal women, aged >60 years, found that neither supplemental soy protein (18 g/day) nor isoflavones (105 mg/day), alone or in combination, significantly affected BMD over a 1-year period.74 To date, results of studies are conflicting, but a recent meta-analysis of nine randomized controlled trials (trial duration: 1–12 months) concluded that soy isoflavones at doses up to 90 mg/day inhibit bone resorption and stimulate bone formation.75 Some authors have proposed that the effect of soy isoflavones on bone health may be dependent on whether or not the individual produces the isoflavone metabolite, equol (see the Bioavailability and Metabolism section above).76–79 This could possibly explain disparate results among clinical trials. Thus, while there is some evidence that isoflavone-rich diets have bone-sparing effects, it is not known whether increasing soy isoflavone intake appreciably decreases the risk of osteoporosis or osteoporotic fracture.
Scientific research on the effect of soy isoflavones on cognitive function is limited. An observational study that examined the relationship between soy intake and cognitive function found that Hawaiian men who reported consuming tofu at least twice weekly during midlife were more likely to have poor cognitive test scores 20–25 years later than those who reported consuming tofu less than twice a week.80 In an Indonesian study of elderly men and women, consumption of tofu was associated with worse memory, while consumption of tempeh was associated with improved memory.81 In contrast, the results of several small clinical trials in postmenopausal women suggest that increasing soy isoflavone in-take may result in modest improvements in performance on some cognitive tests for up to 6 months. Postmenopausal women given soy extracts, providing 60 mg/day of soy isoflavones for 6–12 weeks, performed better on cognitive tests of picture recall (short-term memory), learning rule reversals (mental flexibility), and a planning task, compared with women given a placebo.82,83 In a longer trial, postmenopausal women given supplements that provided 110 mg/day of soy isoflavones for 6 months performed better on a test of verbal fluency than women given placebos.84 In a crossover trial lasting 6 months, women receiving 60 mg/day of soy isoflavones experienced significant improvements in cognitive performance and overall mood compared with when the women were given a placebo.85 However, in larger placebo-controlled trials of postmenopausal women, giving 80 mg/day of isoflavones for 6 months or 99 mg/day of isoflavones for 1 year did not affect performance on a battery of cognitive function tests, including tests for memory, attention, verbal fluency, motor control, and dementia.67,86 A recent review of eight trials, seven of which were conducted in postmenopausal women, found half reported that soy isoflavone treatment was associated with improvements in cognitive function.87
Hot flushes (flashes) are the primary reason that women seek medical attention for menopausal symptoms.88 Concern over potential adverse effects of hormone replacement therapy89,90 has led to increased interest in the use of phytoestrogen supplements by women experiencing menopausal symptoms.91 The effects of increasing soy isoflavone intake on the frequency of hot flushes have been examined in several randomized controlled trials.92–94 To date, at least four reviews of such trials have been published. A review published in 2002 found that only one out of eight randomized controlled trials of soy foods reported a significant reduction in the frequency of hot flushes, while three out of five controlled trials of soy isoflavone extracts reported a significant reduction in hot flush frequency.95 In general, any reductions observed were modest (10%–20%) compared with placebo. A 2004 systematic review that examined 10 randomized controlled trials found that only four trials reported beneficial effects of soy preparations in the treatment of menopausal symptoms like hot flushes.94 More recently, another systematic review and meta-analysis of 12 randomized controlled trials found that soy isoflavone supplementation was associated with a small reduction in the number of hot flushes; this analysis found that women with a higher number of daily flushes experienced the greatest benefit from isoflavone therapy.93 One review that analyzed various trials according to the specific isoflavones contained in the supplements found that use of supplements containing primarily genistein reduced symptoms of hot flushes.96 Interestingly, a recent study found that only women who produced the isoflavone metabolite, equol (see the Bioavailability and Metabolism section above), which was detected in the urine, experienced improvements in menopausal symptoms like hot flushes following soy isoflavone supplementation.97 Breast cancer survivors in particular may experience more frequent and severe hot flushes related to therapies aimed at preventing recurrence of breast cancer.98 However, none of the randomized controlled trials in breast cancer survivors found that soy isoflavone supplementation was significantly more effective than a placebo in decreasing the frequency or severity of hot flushes.99–102 To date, studies on the effect of soy isoflavone consumption on menopausal symptoms have reported mixed results.
Isoflavones are found in small amounts in several legumes, grains, and vegetables, but soybeans are by far the most concentrated source of isoflavones in the human diet.103,104 Recent surveys suggest that average dietary isoflavone intakes in Japan, China, and other Asian countries range from 25 mg/day to 50 mg/day.34 Dietary isoflavone intakes are considerably lower in Western countries, where studies have found average isoflavone intakes to be as low as 2 mg/day.35,36 Traditional Asian foods made from soybeans include tofu, tempeh, miso, and natto. Edamame refers to varieties of soybeans that are harvested and eaten in their green phase. Soy products that are gaining popularity in Western countries include soy-based meat substitutes, soy milk, soy cheese, and soy yogurt.
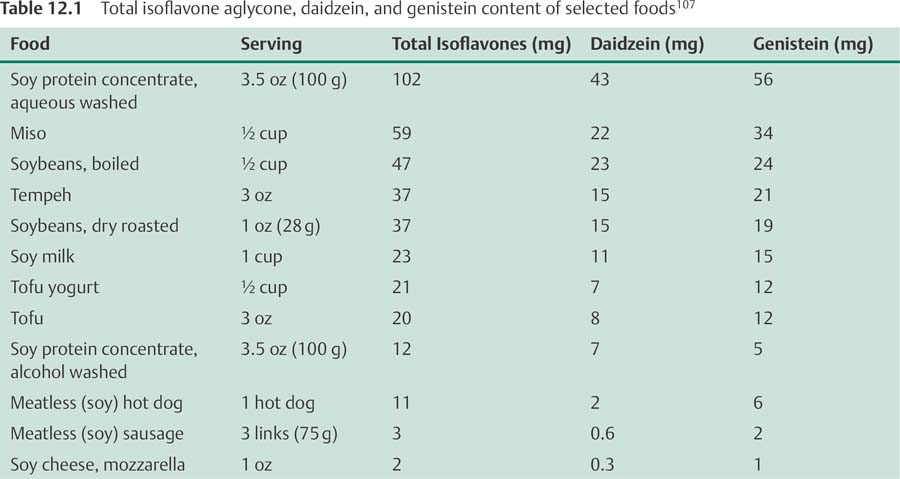
The isoflavone content of a soy protein isolate depends on the method used to isolate it. Soy protein isolates prepared by an ethanol wash process generally lose most of their associated isoflavones, while those prepared by aqueous wash processes tend to retain them.105 Some foods that are rich in soy isoflavones are listed in Table 12.1, along with their isoflavone content.106 Because the isoflavone content of soy foods can vary considerably between brands and between different lots of the same brand,105 these values should be viewed only as a guide. Given the potential health implications of diets rich in soy isoflavones, accurate and consistent labeling of the soy isoflavone content of soy foods is needed.
Soy isoflavone extracts and supplements are available as dietary supplements without a prescription in the United States. These products are not standardized, and the amounts of soy isoflavones they provide may vary considerably. Moreover, quality control may be an issue with some of these products.107 When isoflavone supplements available in the United States were tested for their isoflavone content by an independent laboratory, the isoflavone content in the product differed by more than 10% from the amount claimed on the label in approximately 50% of the products tested.108
Soy-based infant formulas are made from soy protein isolate and contain significant amounts of soy isoflavones. In 1997, the total isoflavone content of soy-based infant formulas that were commercially available in the United States ranged from 32 mg/L to 47 mg/L (approx. 34 fl oz).109
For many years, soy isoflavones have been consumed by humans as part of soy-based diets, without any evidence of adverse effects.104 The 75th percentile of dietary isoflavone intake has been reported to be as high as 65 mg/day in some Asian populations.110 Although diets rich in soy or soy-containing products appear safe and potentially beneficial, the long-term safety of very high supplemental doses of soy isoflavones is not yet known. One study in older men and women found that 100 mg/day of soy isoflavones for 6 months was well tolerated.111 Yet, long-term studies are needed to evaluate the safety of isoflavones.
The safety of high intakes of soy isoflavones and other phytoestrogens for breast cancer survivors is an area of considerable debate among scientists and clinicians.98,112 The effects of high in-takes of soy isoflavones on breast cancer recurrence and survival of breast cancer patients have not been well studied. The results of cell culture and animal studies are conflicting, but some have found that soy isoflavones can stimulate the growth of estrogen-receptor-positive (ER+) breast cancer cells.113,114 High intakes of the soy isoflavone, genistein, interfered with the ability of tamoxifen to inhibit the growth of ER+ breast cancer cells implanted in mice,115 but it is not known if a similar effect would be seen in humans. A recent prospective study in 5042 female breast cancer survivors in China, who were followed for a median of 3.9 years, found that consumption of isoflavone-rich soy foods was significantly associated with a 29% lower risk of death and a 32% lower risk of cancer recurrence.116 In this study, soy isoflavone consumption was associated with a nonsignificant, 21% reduction in risk of death and a significant, 23% reduction in risk of cancer recurrence.116 Very limited data from clinical trials suggest that increased consumption of soy isoflavones (38–45 mg/day) can have estrogenic effects in human breast tissue.117,118 However, a study in women with biopsy-confirmed breast cancer found that supplementation with 200 mg/day of soy isoflavones did not increase tumor growth over the next 2–6 weeks before surgery when compared with a control group that did not take soy isoflavones.119 Given the available data, some experts think that women with a history of breast cancer, particularly ER+ breast cancer, should not increase their consumption of phytoestrogens, including soy isoflavones.98 However, other experts argue that there is not enough evidence to discourage breast cancer survivors from consuming soy foods in moderation,112 and the recent study mentioned above116 indicates that moderate consumption of soy foods (11 g/day of soy protein) may even be beneficial to breast cancer survivors. Due to conflicting results, more research is needed to determine the safety of high soy isoflavone intake in breast cancer survivors.
Infant formula made from soy protein isolate has been commercially available since the mid-1960s.120 As much as 25% of the infant formula sold in the United States is soy-based formula.121 Since infants fed soy-based formulas are exposed to relatively high levels of isoflavones, which they can absorb and metabolize, concern has been raised regarding potential long-term effects on growth and development, as well as reproductive and immune function.109,122 The results of at least six clinical trials comparing infants who were fed soy-based formula with infants fed cow's-milk-based formula indicate that soy-based formula supports normal growth and development in the first year of life.123 A prospective study evaluating growth and development in children fed breast milk, cow's-milk-based formula, or soy-based formula is currently under way at the Arkansas Children's Nutrition Center. Five years into the study, adverse effects of soy formula have not been observed, and no differences in growth and development among the various groups have been noted.124 In addition, one retrospective study of 811 men and women aged 20–34 years found no differences in height, weight, time of puberty, general health, or pregnancy outcomes between those fed soy-based formula as infants and those fed cow's-milk-based formula, although women fed soy-based formula reported significantly greater use of asthma or allergy drugs than women fed cow's milk formula.125 The American Academy of Pediatrics recently published a report that reviews the indications and contraindications for the use of soy-based formulas.121 At present, there is no convincing evidence that infants fed soy-based formula are at greater risk for adverse effects than infants fed cow's milk-based formula. However, long-term studies on the growth and development of infants fed soy-based formula are currently ongoing.126,127
In cell culture and animal studies, soy isoflavones have been found to inhibit the activity of thyroid peroxidase, an enzyme required for thyroid hormone synthesis.128,129 However, high intakes of soy isoflavones do not appear to increase the risk of hypothyroidism, as long as dietary iodine consumption is adequate.130 Since the addition of iodine to soy-based formulas in the 1960s, there have been no further reports of hypothyroidism in infants fed on soy formula.131 Several clinical trials, mostly in premenopausal and postmenopausal women with sufficient iodine intakes, have not found that increased consumption of soy isoflavones results in clinically significant changes in circulating thyroid hormone levels.132–136
To date, studies have not examined the effect of an isoflavone-rich diet on fetal development or pregnancy outcomes in humans, and the safety of isoflavone supplements during pregnancy has not been established.
Because colonic bacteria play an important role in the metabolism of soy isoflavones, antibiotic therapy could decrease their biological activity.137 Some evidence from animal studies suggests that high intakes of soy isoflavones, particularly genistein, can interfere with the antitumor effects of tamoxifen (Nolvadex).115 Until more is known about potential interactions in humans, those taking tamoxifen or other selective estrogen receptor modulators to treat or prevent breast cancer should avoid soy protein supplements or isoflavone extracts (see the Safety for Breast Cancer Survivors section above). High in-takes of soy protein may interfere with the efficacy of the anticoagulant medication warfarin. There is one case report of an individual on warfarin who developed subtherapeutic international normalized ratio (INR; prothrombin time) values upon consuming approximately 16 oz of soy milk daily for 4 weeks.138 INR values returned to therapeutic levels 2 weeks after discontinuing soy milk. The amount of levothyroxine required for adequate thyroid hormone replacement has been found to increase in infants with congenital hypothyroidism fed soy formula.131,139 Taking levothyroxine at the same time as a soy protein supplement also increased the levothyroxine dose required for adequate thyroid hormone replacement in an adult with hypothyroidism.140
• Isoflavones are a class of phytoestrogens—plant-derived compounds with estrogenic activity. Soybeans and soy products are the richest sources of isoflavones in the human diet.
• The results of randomized controlled trials suggest that substituting 50 g/day of soy protein for animal protein results in only a modest 3% reduction of low-density lipoprotein cholesterol. Isolated soy isoflavone supplements do not appear to have favorable effects on serum lipid profiles.
• Consumption of soy isoflavones, at doses of <90 mg/day, may inhibit bone resorption and stimulate bone formation.
• Overall, the results of numerous observational studies do not support the idea that high soy isoflavone intakes in adults are protective against breast cancer. Limited research suggests that higher intakes of soy foods early in life may decrease the risk of breast cancer in adulthood.
• Although scientists are interested in the potential for soy isoflavones to prevent or inhibit the progression of prostate cancer, evidence from observational studies that soy isoflavones are protective against prostate cancer is limited and inconsistent.
• To date, studies on the effect of soy isoflavone consumption on menopausal symptoms have reported mixed results.
• Some health effects of soy isoflavones may be dependent on whether or not the isoflavone metabolite equol is produced.
• Although diets rich in soy or soy-containing products appear safe and potentially beneficial, the long-term safety of high doses of soy isoflavone supplements is not yet known.
• At present, there is no convincing evidence that infants fed soy-based formula are at greater risk for adverse effects than infants fed cow's-milk-based formula.
1. Lampe JW. Isoflavonoid and lignan phytoestrogens as dietary biomarkers. J Nutr 2003;133(Suppl 3):956S–964S
2. Rowland I, Faughnan M, Hoey L, Wähälä K, Williamson G, Cassidy A. Bioavailability of phyto-oestrogens. Br J Nutr 2003;89(Suppl 1):S45–S58
3. Setchell KD, Brown NM, Lydeking-Olsen E. The clinical importance of the metabolite equol-a clue to the effectiveness of soy and its isoflavones. J Nutr 2002;132(12):3577–3584
4. National Cancer Institute. Understanding Cancer Series: Estrogen Receptors/SERMs. National Cancer Institute. Available at: http://www.cancer.gov/cancertopics/understandingcancer/estrogenreceptors. Accessed May 3, 2012
5. Wang LQ. Mammalian phytoestrogens: enterodiol and enterolactone. J Chromatogr B Analyt Technol Biomed Life Sci 2002;777(1–2):289–309
6. Barnes S, Boersma B, Patel R, et al. Isoflavonoids and chronic disease: mechanisms of action. Biofactors 2000;12(1–4):209–215
7. Kao YC, Zhou C, Sherman M, Laughton CA, Chen S. Molecular basis of the inhibition of human aromatase (estrogen synthetase) by flavone and isoflavone phytoestrogens: A site-directed mutagenesis study. Environ Health Perspect 1998;106(2):85–92
8. Whitehead SA, Cross JE, Burden C, Lacey M. Acute and chronic effects of genistein, tyrphostin and lavendustin A on steroid synthesis in luteinized human granulosa cells. Hum Reprod 2002;17(3):589–594
9. Holzbeierlein JM, McIntosh J, Thrasher JB. The role of soy phytoestrogens in prostate cancer. Curr Opin Urol 2005;15(1):17–22
10. Akiyama T, Ishida J, Nakagawa S, et al. Genistein, a specific inhibitor of tyrosine-specific protein kinases. J Biol Chem 1987;262(12):5592–5595
11. Ruiz-Larrea MB, Mohan AR, Paganga G, Miller NJ, Bolwell GP, Rice-Evans CA. Antioxidant activity of phytoestrogenic isoflavones. Free Radic Res 1997; 26(1):63–70
12. Wiseman H, O'Reilly JD, Adlercreutz H, et al. Isoflavone phytoestrogens consumed in soy decrease F(2)-isoprostane concentrations and increase resistance of low-density lipoprotein to oxidation in humans. Am J Clin Nutr 2000;72(2):395–400
13. Hodgson JM, Puddey IB, Croft KD, Mori TA, Rivera J, Beilin LJ. Isoflavonoids do not inhibit in vivo lipid peroxidation in subjects with high-normal blood pressure. Atherosclerosis 1999;145(1):167–172
14. Djuric Z, Chen G, Doerge DR, Heilbrun LK, Kucuk O. Effect of soy isoflavone supplementation on markers of oxidative stress in men and women. Cancer Lett 2001;172(1):1–6
15. Anderson JW, Johnstone BM, Cook-Newell ME. Meta-analysis of the effects of soy protein intake on serum lipids. N Engl J Med 1995;333(5):276–282
16. Sacks FM, Lichtenstein A, Van Horn L, Harris W, KrisEtherton P, Winston M; American Heart Association Nutrition Committee. Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation 2006;113(7):1034–1044
17. Zhan S, Ho SC. Meta-analysis of the effects of soy protein containing isoflavones on the lipid profile. Am J Clin Nutr 2005;81(2):397–408
18. Zhuo XG, Melby MK, Watanabe S. Soy isoflavone in-take lowers serum LDL cholesterol: a meta-analysis of 8 randomized controlled trials in humans. J Nutr 2004;134(9):2395–2400
19. Lichtenstein AH, Jalbert SM, Adlercreutz H, et al. Lipo-protein response to diets high in soy or animal protein with and without isoflavones in moderately hypercholesterolemic subjects. Arterioscler Thromb Vasc Biol 2002;22(11):1852–1858
20. Weggemans RM, Trautwein EA. Relation between soy-associated isoflavones and LDL and HDL cholesterol concentrations in humans: a meta-analysis. Eur J Clin Nutr 2003;57(8):940–946
21. Dewell A, Hollenbeck PL, Hollenbeck CB. Clinical review: a critical evaluation of the role of soy protein and isoflavone supplementation in the control of plasma cholesterol concentrations. J Clin Endocrinol Metab 2006;91(3):772–780
22. Landmesser U, Hornig B, Drexler H. Endothelial function: a critical determinant in atherosclerosis? Circulation 2004; 109(21, Suppl 1): II27–II33
23. Squadrito F, Altavilla D, Crisafulli A, et al. Effect of genistein on endothelial function in postmenopausal women: a randomized, double-blind, controlled study. Am J Med 2003;114(6):470–476
24. Simons LA, von Konigsmark M, Simons J, Celermajer DS. Phytoestrogens do not influence lipoprotein levels or endothelial function in healthy, postmenopausal women. Am J Cardiol 2000;85(11):1297–1301
25. Katz DL, Evans MA, Njike VY, et al. Raloxifene, soy phytoestrogens and endothelial function in post-menopausal women. Climacteric 2007;10(6):500–507
26. Kreijkamp-Kaspers S, Kok L, Bots ML, Grobbee DE, Lampe JW, van der Schouw YT. Randomized controlled trial of the effects of soy protein containing isoflavones on vascular function in postmenopausal women. Am J Clin Nutr 2005;81(1):189–195
27. Steinberg FM, Guthrie NL, Villablanca AC, Kumar K, Murray MJ. Soy protein with isoflavones has favorable effects on endothelial function that are independent of lipid and antioxidant effects in healthy postmenopausal women. Am J Clin Nutr 2003;78(1):123–130
28. Blum A, Lang N, Vigder F, et al. Effects of soy protein on endothelium-dependent vasodilatation and lipid profile in postmenopausal women with mild hyper-cholesterolemia. Clin Invest Med 2003;26(1):20–26
29. Teede HJ, Dalais FS, Kotsopoulos D, Liang YL, Davis S, McGrath BP. Dietary soy has both beneficial and potentially adverse cardiovascular effects: a placebo-controlled study in men and postmenopausal women. J Clin Endocrinol Metab 2001;86(7):3053–3060
30. Evans M, Njike VY, Hoxley M, Pearson M, Katz DL. Effect of soy isoflavone protein and soy lecithin on endothelial function in healthy postmenopausal women. Menopause 2007;14(1):141–149
31. van Popele NM, Grobbee DE, Bots ML, et al. Association between arterial stiffness and atherosclerosis: the Rotterdam Study. Stroke 2001;32(2):454–460
32. Nestel PJ, Yamashita T, Sasahara T, et al. Soy isoflavones improve systemic arterial compliance but not plasma lipids in menopausal and perimenopausal women. Arterioscler Thromb Vasc Biol 1997; 17(12):3392–3398
33. Teede HJ, Giannopoulos D, Dalais FS, Hodgson J, McGrath BP. Randomised, controlled, cross-over trial of soy protein with isoflavones on blood pressure and arterial function in hypertensive subjects. J Am Coll Nutr 2006;25(6):533–540
34. Messina M, Nagata C, Wu AH. Estimated Asian adult soy protein and isoflavone intakes. Nutr Cancer 2006;55(1):1–12
35. van Erp-Baart MA, Brants HA, Kiely M, et al. Isoflavone intake in four different European countries: the VENUS approach. Br J Nutr 2003;89(Suppl 1):S25–S30
36. de Kleijn MJ, van der Schouw YT, Wilson PW, et al. Intake of dietary phytoestrogens is low in postmenopausal women in the United States: the Framingham study(1–4). J Nutr 2001;131(6):1826–1832
37. Shu XO, Jin F, Dai Q, et al. Soyfood intake during adolescence and subsequent risk of breast cancer among Chinese women. Cancer Epidemiol Biomarkers Prev 2001;10(5):483–488
38. Wu AH, Wan P, Hankin J, Tseng CC, Yu MC, Pike MC. Adolescent and adult soy intake and risk of breast cancer in Asian-Americans. Carcinogenesis 2002; 23(9):1491–1496
39. Horn-Ross PL, John EM, Canchola AJ, Stewart SL, Lee MM. Phytoestrogen intake and endometrial cancer risk. J Natl Cancer Inst 2003;95(15):1158–1164
40. Goodman MT, Wilkens LR, Hankin JH, Lyu LC, Wu AH, Kolonel LN. Association of soy and fiber consumption with the risk of endometrial cancer. Am J Epidemiol 1997;146(4):294–306
41. Xu WH, Zheng W, Xiang YB, et al. Soya food intake and risk of endometrial cancer among Chinese women in Shanghai: population based case-control study. BMJ 2004;328(7451):1285
42. Murray MJ, Meyer WR, Lessey BA, Oi RH, DeWire RE, Fritz MA. Soy protein isolate with isoflavones does not prevent estradiol-induced endometrial hyperplasia in postmenopausal women: a pilot trial. Meno-pause 2003;10(5):456–464
43. Messina MJ. Emerging evidence on the role of soy in reducing prostate cancer risk. Nutr Rev 2003;61(4): 117–131
44. Steiner C, Arnould S, Scalbert A, Manach C. Isoflavones and the prevention of breast and prostate cancer: new perspectives opened by nutrigenomicc. Br J Nutr 2008;99 (E Suppl 1):ES78–ES108
45. Adams KF, Chen C, Newton KM, Potter JD, Lampe JW. Soy isoflavones do not modulate prostate-specific antigen concentrations in older men in a randomized controlled trial. Cancer Epidemiol Biomarkers Prev 2004;13(4):644–648
46. Jenkins DJ, Kendall CW, D'Costa MA, et al. Soy consumption and phytoestrogens: effect on serum prostate specific antigen when blood lipids and oxidized low-density lipoprotein are reduced in hyperlipidemic men. J Urol 2003;169(2):507–511
47. Urban D, Irwin W, Kirk M, et al. The effect of isolated soy protein on plasma biomarkers in elderly men with elevated serum prostate specific antigen. J Urol 2001;165(1):294–300
48. Fischer L, Mahoney C, Jeffcoat AR, et al. Clinical characteristics and pharmacokinetics of purified soy isoflavones: multiple-dose administration to men with prostate neoplasia. Nutr Cancer 2004;48(2):160–170
49. Hussain M, Banerjee M, Sarkar FH, et al. Soy isoflavones in the treatment of prostate cancer. Nutr Cancer 2003;47(2):111–117
50. Dalais FS, Meliala A, Wattanapenpaiboon N, et al. Effects of a diet rich in phytoestrogens on prostate-specific antigen and sex hormones in men diagnosed with prostate cancer. Urology 2004;64(3):510–515
51. Pendleton JM, Tan WW, Anai S, et al. Phase II trial of isoflavone in prostate-specific antigen recurrent prostate cancer after previous local therapy. BMC Cancer 2008;8:132
52. Messina M, Kucuk O, Lampe JW. An overview of the health effects of isoflavones with an emphasis on prostate cancer risk and prostate-specific antigen levels. J AOAC Int 2006;89(4):1121–1134
53. Yan L, Spitznagel EL. Soy consumption and prostate cancer risk in men: a revisit of a meta-analysis. Am J Clin Nutr 2009;89(4):1155–1163
54. Goetzl MA, Van Veldhuizen PJ, Thrasher JB. Effects of soy phytoestrogens on the prostate. Prostate Cancer Prostatic Dis 2007;10(3):216–223
55. Setchell KD, Lydeking-Olsen E. Dietary phytoestrogens and their effect on bone: evidence from in vitro and in vivo, human observational, and dietary intervention studies. Am J Clin Nutr 2003; 78(3, Suppl):593S–609S
56. Chiechi LM, Secreto G, D'Amore M, et al. Efficacy of a soy rich diet in preventing postmenopausal osteoporosis: the Menfis randomized trial. Maturitas 2002;42(4):295–300
57. Scheiber MD, Liu JH, Subbiah MT, Rebar RW, Setchell KD. Dietary inclusion of whole soy foods results in significant reductions in clinical risk factors for osteoporosis and cardiovascular disease in normal post-menopausal women. Menopause 2001;8(5):384–392
58. Arjmandi BH, Khalil DA, Smith BJ, et al. Soy protein has a greater effect on bone in postmenopausal women not on hormone replacement therapy, as evidenced by reducing bone resorption and urinary calcium excretion. J Clin Endocrinol Metab 2003;88(3): 1048–1054
59. Harkness LS, Fiedler K, Sehgal AR, Oravec D, Lerner E. Decreased bone resorption with soy isoflavone supplementation in postmenopausal women. J Womens Health (Larchmt) 2004;13(9):1000–1007
60. Ye YB, Tang XY, Verbruggen MA, Su YX. Soy isoflavones attenuate bone loss in early postmenopausal Chinese women: a single-blind randomized, placebo-controlled trial. Eur J Nutr 2006;45(6):327–334
61. Wangen KE, Duncan AM, Merz-Demlow BE, et al. Effects of soy isoflavones on markers of bone turnover in premenopausal and postmenopausal women. J Clin Endocrinol Metab 2000;85(9):3043–3048
62. Alekel DL, Germain AS, Peterson CT, Hanson KB, Stewart JW, Toda T. Isoflavone-rich soy protein isolate attenuates bone loss in the lumbar spine of perimenopausal women. Am J Clin Nutr 2000;72(3):844–852
63. Dalais FS, Ebeling PR, Kotsopoulos D, McGrath BP, Teede HJ. The effects of soy protein containing isoflavones on lipids and indices of bone resorption in postmenopausal women. Clin Endocrinol (Oxf) 2003;58(6):704–709
64. Cheong JM, Martin BR, Jackson GS, et al. Soy isoflavones do not affect bone resorption in postmenopausal women: a dose-response study using a novel approach with 41Ca. J Clin Endocrinol Metab 2007;92(2):577–582
65. Potter SM, Baum JA, Teng H, Stillman RJ, Shay NF, Erdman JW Jr. Soy protein and isoflavones: their effects on blood lipids and bone density in postmenopausal women. Am J Clin Nutr 1998; 68(6, Suppl):1375S–1379S
66. Arjmandi BH, Lucas EA, Khalil DA, et al. One year soy protein supplementation has positive effects on bone formation markers but not bone density in post-menopausal women. Nutr J 2005;4(1):8
67. Kreijkamp-Kaspers S, Kok L, Grobbee DE, et al. Effect of soy protein containing isoflavones on cognitive function, bone mineral density, and plasma lipids in postmenopausal women: a randomized controlled trial. JAMA 2004;292(1):65–74
68. Lydeking-Olsen E, Beck-Jensen JE, Setchell KD, Holm-Jensen T. Soymilk or progesterone for prevention of bone loss—a 2 year randomized, placebo-controlled trial. Eur J Nutr 2004;43(4):246–257
69. Gallagher JC, Satpathy R, Rafferty K, Haynatzka V. The effect of soy protein isolate on bone metabolism. Menopause 2004;11(3):290–298
70. Newton KM, LaCroix AZ, Levy L, et al. Soy protein and bone mineral density in older men and women: a randomized trial. Maturitas 2006;55(3):270–277
71. Chen YM, Ho SC, Lam SS, Ho SS, Woo JL. Beneficial effect of soy isoflavones on bone mineral content was modified by years since menopause, body weight, and calcium intake: a double-blind, randomized, controlled trial. Menopause 2004;11(3):246–254
72. Huang HY, Yang HP, Yang HT, Yang TC, Shieh MJ, Huang SY. One-year soy isoflavone supplementation prevents early postmenopausal bone loss but without a dose-dependent effect. J Nutr Biochem 2006;17(8):509–517
73. Brink E, Coxam V, Robins S, Wahala K, Cassidy A, Branca F; PHYTOS Investigators. Long-term consumption of isoflavone-enriched foods does not affect bone mineral density, bone metabolism, or hormonal status in early postmenopausal women: a randomized, double-blind, placebo controlled study. Am J Clin Nutr 2008;87(3):761–770
74. Kenny AM, Mangano KM, Abourizk RH, et al. Soy proteins and isoflavones affect bone mineral density in older women: a randomized controlled trial. Am J Clin Nutr 2009;90(1):234–242
75. Ma DF, Qin LQ, Wang PY, Katoh R. Soy isoflavone in-take inhibits bone resorption and stimulates bone formation in menopausal women: meta-analysis of randomized controlled trials. Eur J Clin Nutr 2008; 62(2):155–161
76. Wu J, Oka J, Ezaki J, et al. Possible role of equol status in the effects of isoflavone on bone and fat mass in postmenopausal Japanese women: a double-blind, randomized, controlled trial. Menopause 2007; 14(5):866–874
77. Vatanparast H, Chilibeck PD. Does the effect of soy phytoestrogens on bone in postmenopausal women depend on the equol-producing phenotype? Nutr Rev 2007;65(6 Pt 1):294–299
78. Ishimi Y. Soybean isoflavones in bone health. Forum Nutr 2009;61:104–116
79. Frankenfeld CL, McTiernan A, Thomas WK, et al. Post-menopausal bone mineral density in relation to soy isoflavone-metabolizing phenotypes. Maturitas 2006;53(3):315–324
80. White LR, Petrovitch H, Ross GW, et al. Brain aging and midlife tofu consumption. J Am Coll Nutr 2000;19(2):242–255
81. Hogervorst E, Sadjimim T, Yesufu A, Kreager P, Rahardjo TB. High tofu intake is associated with worse memory in elderly Indonesian men and women. Dement Geriatr Cogn Disord 2008;26(1):50–57
82. Duffy R, Wiseman H, File SE. Improved cognitive function in postmenopausal women after 12 weeks of consumption of a soya extract containing isoflavones. Pharmacol Biochem Behav 2003;75(3):721–729
83. File SE, Hartley DE, Elsabagh S, Duffy R, Wiseman H. Cognitive improvement after 6 weeks of soy supplements in postmenopausal women is limited to frontal lobe function. Menopause 2005;12(2):193–201
84. Kritz-Silverstein D, Von Mühlen D, Barrett-Connor E, Bressel MA. Isoflavones and cognitive function in older women: the SOy and Postmenopausal Health In Aging (SOPHIA) Study. Menopause 2003;10(3):196–202
85. Casini ML, Marelli G, Papaleo E, Ferrari A, D'Ambrosio F, Unfer V. Psychological assessment of the effects of treatment with phytoestrogens on postmenopausal women: a randomized, double-blind, crossover, placebo-controlled study. Fertil Steril 2006;85(4):972–978
86. Ho SC, Chan AS, Ho YP, et al. Effects of soy isoflavone supplementation on cognitive function in Chinese postmenopausal women: a double-blind, randomized, controlled trial. Menopause 2007;14(3 Pt 1): 489–499
87. Zhao L, Brinton RD. WHI and WHIMS follow-up and human studies of soy isoflavones on cognition. Expert Rev Neurother 2007;7(11):1549–1564
88. Tice JA, Ettinger B, Ensrud K, Wallace R, Blackwell T, Cummings SR. Phytoestrogen supplements for the treatment of hot flashes: the Isoflavone Clover Extract (ICE) Study: a randomized controlled trial. JAMA 2003;290(2):207–214
89. Nelson HD, Humphrey LL, Nygren P, Teutsch SM, Allan JD. Postmenopausal hormone replacement therapy: scientific review. JAMA 2002;288(7):872–881
90. Farquhar C, Marjoribanks J, Lethaby A, Suckling JA, Lamberts Q. Long term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev 2009; (2):CD004143
91. Nelson HD, Vesco KK, Haney E, et al. Nonhormonal therapies for menopausal hot flashes: systematic review and meta-analysis. JAMA 2006;295(17):2057–2071
92. Kronenberg F, Fugh-Berman A. Complementary and alternative medicine for menopausal symptoms: a review of randomized, controlled trials. Ann Intern Med 2002;137(10):805–813
93. Howes LG, Howes JB, Knight DC. Isoflavone therapy for menopausal flushes: a systematic review and meta-analysis. Maturitas 2006;55(3):203–211
94. Huntley AL, Ernst E. Soy for the treatment of perimenopausal symptoms—a systematic review. Maturitas 2004;47(1):1–9
95. Krebs EE, Ensrud KE, MacDonald R, Wilt TJ. Phytoestrogens for treatment of menopausal symptoms: a systematic review. Obstet Gynecol 2004;104(4):824–836
96. Williamson-Hughes PS, Flickinger BD, Messina MJ, Empie MW. Isoflavone supplements containing predominantly genistein reduce hot flash symptoms: a critical review of published studies. Menopause 2006;13(5):831–839
97. Jou HJ, Wu SC, Chang FW, Ling PY, Chu KS, Wu WH. Effect of intestinal production of equol on menopausal symptoms in women treated with soy isoflavones. Int J Gynaecol Obstet 2008;102(1):44–49
98. Duffy C, Cyr M. Phytoestrogens: potential benefits and implications for breast cancer survivors. J Womens Health (Larchmt) 2003;12(7):617–631
99. MacGregor CA, Canney PA, Patterson G, McDonald R, Paul J. A randomised double-blind controlled trial of oral soy supplements versus placebo for treatment of menopausal symptoms in patients with early breast cancer. Eur J Cancer 2005;41(5):708–714
100. Nikander E, Kilkkinen A, Metsä-Heikkilä M, et al. A randomized placebo-controlled crossover trial with phytoestrogens in treatment of menopause in breast cancer patients. Obstet Gynecol 2003;101(6):1213–1220
101. Van Patten CL, Olivotto IA, Chambers GK, et al. Effect of soy phytoestrogens on hot flashes in postmenopausal women with breast cancer: a randomized, controlled clinical trial. J Clin Oncol 2002;20(6): 1449–1455
102. Quella SK, Loprinzi CL, Barton DL, et al. Evaluation of soy phytoestrogens for the treatment of hot flashes in breast cancer survivors: A North Central Cancer Treatment Group Trial. J Clin Oncol 2000;18(5):1068–1074
103. Fletcher RJ. Food sources of phyto-oestrogens and their precursors in Europe. Br J Nutr 2003;89(Suppl 1):S39–S43
104. Munro IC, Harwood M, Hlywka JJ, et al. Soy isoflavones: a safety review. Nutr Rev 2003;61(1):1–33
105. Setchell KD, Cole SJ. Variations in isoflavone levels in soy foods and soy protein isolates and issues related to isoflavone databases and food labeling. J Agric Food Chem 2003;51(14):4146–4155
106. United States Department of Agriculture Nutrient Data Laboratory. USDA-Iowa State University Isoflavones Database, 6/2002. Available at: http://www.nal.usda.gov/fnic/foodcomp/Data/isoflav/isoflav.html. Accessed May 3, 2012
107. Chua R, Anderson K, Chen J, Hu M. Quality, labeling accuracy, and cost comparison of purified soy isoflavonoid products. J Altern Complement Med 2004;10(6):1053–1060
108. Setchell KD, Brown NM, Desai P, et al. Bioavailability of pure isoflavones in healthy humans and analysis of commercial soy isoflavone supplements. J Nutr 2001; 131(4, Suppl):1362S–1375S
109. Setchell KD, Zimmer-Nechemias L, Cai J, Heubi JE. Isoflavone content of infant formulas and the metabolic fate of these phytoestrogens in early life. Am J Clin Nutr 1998; 68(6, Suppl):1453S–1461S
110. Chen Z, Zheng W, Custer LJ, et al. Usual dietary consumption of soy foods and its correlation with the excretion rate of isoflavonoids in overnight urine samples among Chinese women in Shanghai. Nutr Cancer 1999;33(1):82–87
111. Gleason CE, Carlsson CM, Barnet JH, et al. A preliminary study of the safety, feasibility and cognitive efficacy of soy isoflavone supplements in older men and women. Age Ageing 2009;38(1):86–93
112. Messina MJ, Loprinzi CL. Soy for breast cancer survivors: a critical review of the literature. J Nutr 2001; 131(11, Suppl):3095S–3108S
113. Allred CD, Allred KF, Ju YH, Virant SM, Helferich WG. Soy diets containing varying amounts of genistein stimulate growth of estrogen-dependent (MCF-7) tumors in a dose-dependent manner. Cancer Res 2001;61(13):5045–5050
114. Ju YH, Allred CD, Allred KF, Karko KL, Doerge DR, Helferich WG. Physiological concentrations of dietary genistein dose-dependently stimulate growth of estrogen-dependent human breast cancer (MCF-7) tumors implanted in athymic nude mice. J Nutr 2001;131(11):2957–2962
115. Ju YH, Doerge DR, Allred KF, Allred CD, Helferich WG. Dietary genistein negates the inhibitory effect of tamoxifen on growth of estrogen-dependent human breast cancer (MCF-7) cells implanted in athymic mice. Cancer Res 2002;62(9):2474–2477
116. Shu XO, Zheng Y, Cai H, et al. Soy food intake and breast cancer survival. JAMA 2009;302(22):2437–2443
117. Petrakis NL, Barnes S, King EB, et al. Stimulatory influence of soy protein isolate on breast secretion in pre- and postmenopausal women. Cancer Epidemiol Biomarkers Prev 1996;5(10):785–794
118. Hargreaves DF, Potten CS, Harding C, et al. Two-week dietary soy supplementation has an estrogenic effect on normal premenopausal breast. J Clin Endocrinol Metab 1999;84(11):4017–4024
119. Sartippour MR, Rao JY, Apple S, et al. A pilot clinical study of short-term isoflavone supplements in breast cancer patients. Nutr Cancer 2004;49(1):59–65
120. American Academy of Pediatrics. Committee on Nutrition. Soy protein-based formulas: recommendations for use in infant feeding. Pediatrics 1998;101(1 Pt 1):148–153
121. Bhatia J, Greer F; American Academy of Pediatrics Committee on Nutrition. Use of soy protein-based formulas in infant feeding. Pediatrics 2008;121(5): 1062–1068
122. Setchell KD, Zimmer-Nechemias L, Cai J, Heubi JE. Isoflavone content of infant formulas and the metabolic fate of these phytoestrogens in early life. Am J Clin Nutr 1998; 68(6, Suppl):1453S–1461S
123. Mendez MA, Anthony MS, Arab L. Soy-based formulae and infant growth and development: a review. J Nutr 2002;132(8):2127–2130
124. Badger TM, Gilchrist JM, Pivik RT, et al. The health implications of soy infant formula. Am J Clin Nutr 2009;89(5):1668S–1672S
125. Strom BL, Schinnar R, Ziegler EE, et al. Exposure to soy-based formula in infancy and endocrinological and reproductive outcomes in young adulthood. JAMA 2001;286(7):807–814
126. US Department of Agriculture, Agricultural Research Service. Study Examines Long-Term Health Effects of Soy Infant Formula. 2004. Available at: http://www.ars.usda.gov/is/AR/archive/jan04/soy0104.htm. Accessed May 3, 2012
127. Turck D. Soy protein for infant feeding: what do we know? Curr Opin Clin Nutr Metab Care 2007; 10(3):360–365
128. Divi RL, Chang HC, Doerge DR. Anti-thyroid isoflavones from soybean: isolation, characterization, and mechanisms of action. Biochem Pharmacol 1997; 54(10):1087–1096
129. Doerge DR, Sheehan DM. Goitrogenic and estrogenic activity of soy isoflavones. Environ Health Perspect 2002;110(Suppl 3):349–353
130. Messina M, Redmond G. Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: a review of the relevant literature. Thyroid 2006;16(3):249–258
131. Chorazy PA, Himelhoch S, Hopwood NJ, Greger NG, Postellon DC. Persistent hypothyroidism in an infant receiving a soy formula: case report and review of the literature. Pediatrics 1995;96(1 Pt 1):148–150
132. Bruce B, Messina M, Spiller GA. Isoflavone supplements do not affect thyroid function in iodine-replete postmenopausal women. J Med Food 2003; 6(4):309–316
133. Persky VW, Turyk ME, Wang L, et al. Effect of soy protein on endogenous hormones in postmenopausal women. Am J Clin Nutr 2002;75(1):145–153
134. Duncan AM, Merz BE, Xu X, Nagel TC, Phipps WR, Kurzer MS. Soy isoflavones exert modest hormonal effects in premenopausal women. J Clin Endocrinol Metab 1999;84(1):192–197
135. Duncan AM, Underhill KE, Xu X, Lavalleur J, Phipps WR, Kurzer MS. Modest hormonal effects of soy isoflavones in postmenopausal women. J Clin Endocrinol Metab 1999;84(10):3479–3484
136. Dillingham BL, McVeigh BL, Lampe JW, Duncan AM. Soy protein isolates of varied isoflavone content do not influence serum thyroid hormones in healthy young men. Thyroid 2007;17(2):131–137
137. Natural Medicines Comprehensive Database. Soy. 2004. Available at: http://www.naturaldatabase.com/monograph.asp?mono_id=975&brand_id=. Accessed May 3, 2012
138. Cambria-Kiely JA. Effect of soy milk on warfarin efficacy. Ann Pharmacother 2002;36(12):1893–1896
139. Jabbar MA, Larrea J, Shaw RA. Abnormal thyroid function tests in infants with congenital hypothyroidism: the influence of soy-based formula. J Am Coll Nutr 1997;16(3):280–282
140. Bell DS, Ovalle F. Use of soy protein supplement and resultant need for increased dose of levothyroxine. Endocr Pract 2001;7(3):193–194