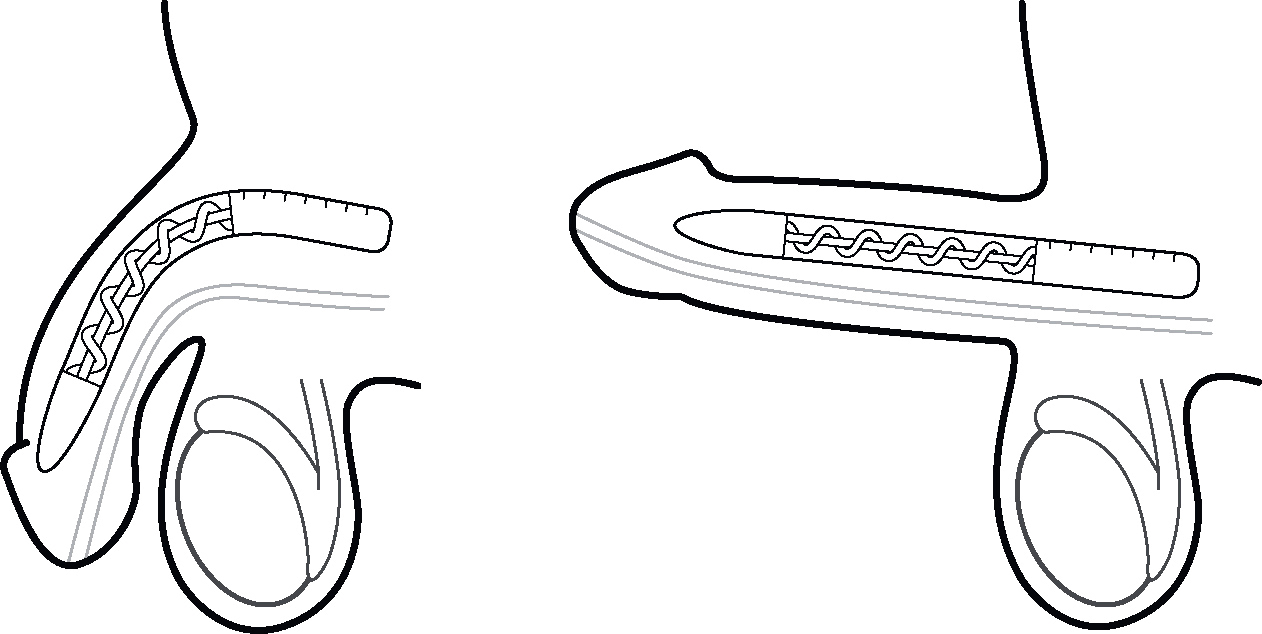
Figure 1 Semirigid penis implant
“Nothing is certain except death and taxes…and erections if you really want them.” So said a urology colleague to me years ago. Most guys want to take a pill to fix a problem. Shots and vacuum pumps are not necessarily first-line treatments, but they often work when pills fail. Even so, they don’t work for everyone. That’s where surgery comes in. Known as third-line therapy, it’s the end of the line when it comes to treatment options, but it’s also the beginning of sex again for men who need it and can, in fact, give them a great deal of satisfaction.
The most commonly performed surgery to restore erections is a penile implant. This is a replacement for the blood-filling chambers of the penis. Other less commonly performed surgeries or procedures are intended to repair, bypass, or stretch open the actual blood vessels entering those chambers. Because of the very small caliber of the blood vessels and because so often the problem is not just limited to those blood vessels but is within the chambers themselves, these other operations are less successful, not routinely practiced, and best reserved for the very specific types of problems for which they work best.
The earliest recorded penile implant surgery was performed by a German surgeon, Dr. Bogaras, to repair a severe battle injury in the 1930s. He used rib cartilage because he took notice that many animals, including monkeys and dogs, have bones in their penises. In 1944, Dr. Frumkin used a rib surrounded by some abdominal skin as an implant in a patient with erectile dysfunction.1 A variety of implanted artificial materials were experimented with over the years. Today we use crafted metal coated with silicone. These implants are referred to as “semi-rigid” because they are designed to have a flexible but firm section that can be bent up or down, depending on how you roll. Up is for “sport suspension” (sex) and down is for “comfort suspension” (tucked out of the way). These are safe, reliable, and simple implants that work very well.2
In 1973, down in Texas (where everything is bigger), Dr. Brantley Scott of Baylor University introduced the world to a multi-component system that can mimic the hardness of an erection and the softness of a flaccid penis. This is a more natural experience for the man as opposed to the semirigid implant, which is always firm, one way or the other. Known as an “inflatable” penile prosthesis (implant), it has become the standard of care for most men needing surgery. Refinements and technological advances over the years have led to a device that is reliable, safe, and straightforward to place, making it accessible to men far and wide (and deep). The implant has three specialized components. The first component is the cylinders that are implanted into the penis. Penises come in varying lengths, and so do these cylinders. They are designed to be the approximate shape and size of the chambers in the penis that fill up with blood. These, however, don’t fill up with blood; instead, they fill up with sterile water. That water is stored in a small reservoir or container that is tucked away under the lower abdominal muscles, near the bladder. The water gets pumped into and out of these cylinders by a small mechanism that is placed in the scrotum between the two testicles like a third ball. All the components are connected to each other by thin tubing. These ingenious implants not only provide excellent erections, but they also provide a more natural “resting” state of the penis when it’s not working hard.
A penile prosthesis (implant) is a wonderful treatment for men who need it, but it’s not for everyone. Because the penile implant cylinders are placed inside the penis’s natural chambers, the tiny, spongy blood vessels inside those chambers that normally would fill with blood are permanently damaged, so if the implant were to be removed, that tissue would never work again. Therefore, the implant surgery is a permanent step. There is no going back and trying pills or shots or even the vacuum. This is why the surgery is considered third-line treatment. Before having penile implant surgery, most men will be encouraged to try the first-line options of pills up to maximal doses and the second-line options of penis self-injection or vacuum constriction device (the penis pump). For most men who choose surgery, none of these options works. For some, the side effects are prohibitive, and for a few, the nature of the second-line treatments is distressing and simply unacceptable.
Figure 1 Semirigid penis implant

Figure 2 Inflatable penile implant
Unlike a breast augmentation, a penile prosthesis is not for cosmetic purposes, but rather to restore a function. Breast implants do not restore the function of the breast, which is to produce milk. Penis implants do restore the function of the penis, which along with urinating is to become erect so as to allow sexual activity and, if desired, insemination and reproduction. A penis implant allows all of that to happen. A penis implant does not, however, make the penis any bigger. Let me repeat that: A penis implant does not make the penis bigger. You may be wondering why not, since breast augmentation certainly makes breasts bigger. The reason is that the tissues inside the penis will stretch and enlarge only to a point, and then no further. The tissues surrounding the breast glands are fat and skin. These can stretch out a lot and more and more over time. Women can receive larger implants and then a period of time later “upgrade” if they so choose. The part of the penile implant that gets the penis hard and straight is inserted within the chambers of the penis that fill with blood. The chambers, known as the corpus cavernosa, are made of a very flexible but very strong tissue known as tunica albuginia. It’s stretchy, but only to a point, and cannot be overstretched like the skin of the breast. In fact, a penile implant must fit inside this chamber, and therefore the erection is just a little smaller than the natural one. Furthermore, the implant goes in the shaft of the penis only. The head of the penis cannot be implanted, so it does not get bigger when the implant is pumped up.
Getting a penile implant is a big step, and it’s important to go into the operation with realistic expectations. The best way to estimate the size of the penis after an implant is to hold the head of the penis and stretch it straight out as far as you can away from you. Now look down. That’s how long it will be, give or take a few millimeters. The stretched penis is a good approximation of the erect penis size. If you have a gut, it will hide part or all of your penis as you look down at it. If you lose your gut, your penis will look bigger. As you age, gravity pulls your looser parts—skin and fat—ever downward, so even without a gut your penis may be partially hidden behind some skin and fat that used to be above it—sort of like a mudslide, but I call it a “man slide.” This makes your penis look shorter as well. Again, keep in mind the operation is not cosmetic but is to restore function.
Many men who have implants suffer from some actual shrinkage of the penis due to the poor bloodflow over time. These men can feel like they are getting shortchanged since only now are they getting the treatment that works, and it may seem like too little too late. Fortunately, there is a way to restore some or most of the lost length—“penis prehab.” As described in a previous chapter, the vacuum constriction device, aka penis pump, is a cylinder that goes over the penis and forces an erection by creating a vacuum around the penis. This can be done for several minutes a day for several weeks to increase the bloodflow into the penis and stretch and expand it back closer to its old shape before the day of surgery. Improvement in lengthening averages more than 3.5 centimeters over a 2-month period. The other benefits of this stretching prehab are that it often makes the tissues of the penis easier to work with during surgery and may make recovery less painful as well.3
Before performing a surgical implant, the urologist will make sure there are no looming problems with your bladder, prostate, or urethra. If you have problems with your urinary tract that result in infections or the need for surgery, that can lead to complications with the implant. The urologist may take a look at the urinary passageway with a special fiber-optic scope to make sure all is well. No specific testing of the penis itself is required prior to penile implant surgery, but in many cases a duplex/Doppler ultrasound of the penis may be performed to validate that there is a problem with bloodflow. The ultrasound measures the flow of blood into the penis after it is injected with alprostadil or trimix. The Doppler sensor can detect how well the blood is rushing in and how well it is being trapped.
An important consideration is whether to have a semirigid implant or an inflatable penile prosthesis. The semirigid device is simpler, but it is less “natural.” The girth of the penis will be slightly smaller than with the inflated prosthesis, but the rigidity will be excellent. The biggest drawback is that it cannot be deflated, but it can be positioned downward, out of the way. The advantage to its simplicity is that it is easier to use because no pumping of water is required. The pumping mechanism in an inflatable penile prosthesis can be challenging to manipulate for men with limited hand function due to paralysis, severe arthritis, or other conditions that limit their strength or dexterity. For these men, and particularly for men with partial or total paralysis, a semirigid implant can be a better choice. For the vast majority of men, the inflatable three-piece prosthesis will be the right choice.
Penile implants are performed under general or spinal anesthesia. Most urologists will make an incision just below the base of the penis, right across the scrotum, or just above the penis at the pubic bone. Through that incision they can get access to the chambers of the penis, the scrotum, and behind the abdominal wall. The urologist will make small incisions in the chambers of the penis to allow the implanted cylinders to be placed within them. Before placing the implants, the surgeon will measure how long the cavernosal chambers are with a metal measuring sound. Remember, the chambers project back under the pelvic bones just as far as they project forward. These measurements are used to select the size of the implant cylinder that will be put in because one size does not fit all. A semirigid implant can then be placed and the openings sewn up—game over. For an inflatable penile prosthesis, there are two more steps—placing the reservoir for the water under the abdominal wall and placing the pump mechanism in the scrotum. The erection is tested before all the connections are finalized and everything is stitched closed. Sometimes the surgeon may place a small drain tube that will come out through the skin in the low groin and be attached to a suction bulb. This alleviates any oozing of blood from accumulating, and it will typically be removed a day later. The surgeon usually places a Foley catheter in the urethra to keep the bladder drained for a day too. A gauze wrap is placed around the penis, and a jockstrap with ice is applied.
During surgery, there can be challenges or complications. Real life is not like a textbook, and no two penises are exactly the same. An experienced surgeon can handle most any situation, but it’s good to know the possibilities going into surgery. The placement of the cylinders in the penis requires that a space be made within the natural chambers of the penis. This space is normally filled with spongy blood vessel tissue. The surgeon must smash that tissue out of the way with the metal sound that he passes to measure it, and in most cases, with additional sounds he uses to further flatten out that spongy tissue. During this process the surgeon may hit fibrotic tissue that makes it more difficult to pass the metal sound. This fibrosis may be from previous penis injection therapy or it may be from a condition known as Peyronie’s disease, which I will discuss further in Chapter 17. In order to open up the space, he may need to make additional cuts in the lining of the chamber to help get through fibrotic tissue. Sometimes the metal sound or dilator will poke through the wall of the penis chamber. If this happens, it’s not a big problem unless it pokes through the urethra. If that happens, there is a significant risk of infection or further urethral injury, so the implant cylinder cannot be placed on that side and the operation has to be postponed for about 3 months while things heal. Another risk during surgery is injury to the bladder, intestine, or blood vessels during the placement of the water reservoir into the abdomen. This risk is greater if there has been previous surgery in the pelvis.
Depending on the urologist’s discretion, you may go home the same day or the next morning, as long as recovery looks to be uncomplicated. A drain or catheter placed at the time of surgery will need to be removed, typically the next day. You will be instructed to use ice on and off your genitals for the first several days to a week, and typically you can bathe or shower after a couple of days. You will have a prescription for pain medication, but the ice will help a great deal. You will also have a prescription for antibiotics, and it is important that you take those to decrease your risk of infection. You cannot have sex right away. First of all, you will be too sore, and more importantly, your body has to heal and the suture lines that hold the components in place have to strengthen. Furthermore, you run the risk of an infection if your skin incision is not completely healed. Your urologist will let you know when you can have sex, but it’s usually 4 to 6 weeks after surgery, with 6 weeks being the most common.
You will typically have a visit with the doctor soon after surgery to make sure you are recovering appropriately, and then again around the time you are allowed to start using your new and improved penis. During that visit you will be taught how to work the pump in your scrotum. A newly implanted pump is a lot like a new baseball glove. It is stiff and hard to bend. It will take a fair amount of pressure to squeeze the pump the first several times, but then it will soften up and become much easier. Learning the location of the pump and feeling for the proper place to squeeze can be awkward as well, but like anything else, practice makes perfect. It will be a good idea for you to pump up the implant at least once a day for the first 3 months because the body will form a capsule around the cylinders during those early months, and if the implant is mostly empty, the capsule will be smaller and may restrict the cylinders from expanding. Also, your penis may hurt more than you expected. It can be very sore the first several days after the implant, but it will get better and better with each passing day, and once you are back in the saddle you will soon forget all about it. The first few times you have sex it may be sore as well, but some ibuprofen or acetaminophen can help with that, and things will quickly improve.
Over time, the mechanical components of the inflatable penile prosthesis can fail. The rate is amazingly low, less than 2 percent per year.4 The implant may fail to pump up. This can be due to an airlock or a kink in the tubing, a malfunction in the valve, or a leak in the system. If the system leaks, there is no harm done because it’s just sterile water that gets reabsorbed by the body. Another issue can be that the cylinders do not fully deflate or reinflate on their own as if the penis once again has a mind of its own. This can be due to an issue with the one-way valves in the system or to how the reservoir ends up positioned, and if it is not actually bothering you, you may be able to just leave it alone. Over time, the cylinders may erode through the tunica albuginea lining that they were placed inside. If that happens in the midshaft, it may cause an out-pouching of the cylinder under the skin, making the erection appear bent and irregular. If it happens at the tip of the penis, the cylinder may tent up the skin overlying the penis or, even worse, poke all the way through the skin or through the urethra. If it pokes through the urethra, you may notice spots of blood in your underwear or urine, or even spraying of the urine. These complications are more likely if the prosthesis is never deflated or if you have poor sensation and don’t sense the warning signs of too much pressure on the penis. Another rare complication is movement of the reservoir out of its proper place and down towards the scrotum, like a hernia. If it’s not bothering you, it can be left alone.5
Any malfunctions or complications require surgery to fix, and this often means removal and replacement of some or all of the components. A repeat surgery often has a quicker recovery, with less soreness than the initial surgery. Surveys show that the vast majority of patients who have had repeat surgeries did so without hesitation because they are so gratified with how the implant has restored their sexual function.6
The most dangerous risk is infection. Infection can start at the time of surgery and take a few weeks to show itself, or it can happen years later. The risk of infection is only about 2 percent,7 and the signs of infection can be very subtle. There may be some increased pain and tenderness in the penis or scrotum, possibly some redness and warmth, or the skin may thicken and get “stuck” on one of the underlying parts. Often there is no fever or abnormal blood test. In other instances an infection can be very dramatic, with pus draining from the scrotum or urethra and possibly fever and chills. Because the penis implant has no blood vessels within its parts, antibiotics cannot saturate it. Furthermore, the body naturally forms a tough capsule around the implanted parts that is a boundary across which no blood vessel can cross. To add insult to injury, when bacteria infect an implant, they form a defensive film barrier along the surface of the implant called a “biofilm” that protects them even further. So if bacteria are able to reach the implant and set up an infection, there is no way to eliminate the infection with antibiotics and the implant must be removed. In the case of a mild infection, the symptoms may seem to improve with antibiotics but once treatment is over, they will come back. If the infection is a milder one, a new implant can be put in right away after the infected one is removed, and the tissue is thoroughly rinsed out with antibiotic rinse. If the infection is severe, there is a much higher risk that a replacement at that time will get infected too, so in that case it must be removed and a new one put in later, after healing is complete. When an implant has to be removed and cannot be replaced, the penis can contract and scar down as it’s healing and become permanently shorter and narrower. In addition, the replacement implant often is narrower and shorter. In such a case there may be some benefit to using a vacuum pump daily to keep the penis long and strong while it is healing up.8
Penile implant surgery is the last line of defense for many men who suffer from erectile dysfunction. In spite of the seriousness of surgery and the possibility of risks, it is a treatment that provides many men and their partners tremendous satisfaction and a return to a healthy, happy love life.