TABLE 36-1. NEUROMUSCULAR MIMICS
TABLE 36-1. NEUROMUSCULAR MIMICSWe define “neuromuscular mimic” as any musculoskeletal condition that presents with pain and apparent weakness, and can mimic a neuromuscular etiology such as radiculopathy or entrapment neuropathy. “Limb pain” is a common reason for referral to the clinic and EMG laboratory and the identification of the underlying pain generator is often challenging. For example, in two series of patients referred for electrodiagnostic testing for suspected cervical or lumbosacral radiculopathy, the prevalence of musculoskeletal disorders was 42% and 32%, respectively.1,2 Thus, musculoskeletal disorders are common in patients suspected of having a radiculopathy. They can mimic radiculopathy or coexist with it in many individuals.1,2 Importantly, neuromuscular mimics can often be diagnosed quickly at the bedside and are eminently treatable. Their prompt recognition may avoid unnecessary and expensive diagnostic procedures and result in more efficient clinical practice. It is common for physicians from many specialties to be unfamiliar with recognizing these conditions.3
In this chapter, we will describe the most common mimics of radiculopathy and neuropathy in the upper and lower limbs (Table 36-1). We will not perform an exhaustive review of these pathologies. Rather, this chapter will serve as an entry point for physicians with minimal musculoskeletal training with the goal of providing them with time-efficient and resource-efficient tools to screen for these common conditions in their busy daily practice.
TABLE 36-1. NEUROMUSCULAR MIMICS
Upper Limb Mimics
Supraspinatus tendinopathy
Biceps tendinopathy
Lateral epicondylitis
De Quervain syndrome
Carpometacarpal (CMC) joint osteoarthritis
Lower Limb Mimics
Hip joint osteoarthritis
Greater trochanteric bursitis
Pes anserine bursitis
Plantar fasciitis
A few key “pearls” are worth remembering when performing a musculoskeletal examination. First, it is important to check the bilateral limbs for side-to-side comparison, starting from the noninvolved side first, whenever possible. If the test maneuver elicits pain, one needs to ask the patient whether the elicited pain is the same that he/she has been experiencing. This is important in order to avoid overcalling pathology as musculoskeletal examination maneuvers can trigger some discomfort even in healthy individuals, particularly if palpation and provocative tests are performed too vigorously. Finally, when assessing whether the maneuver reproduces the patient’s chief complaint, it is very helpful to look for the “wince sign,” with the patient blinking and grimacing as the pain is reproduced.
 TOP MIMICS IN THE UPPER LIMBS
TOP MIMICS IN THE UPPER LIMBSSupraspinatus tendinopathy is a common cause of shoulder pain and can mimic C5/6/7 radiculopathy.
The rotator cuff consists of four muscles that are responsible for securing the arm into the glenohumeral (shoulder) joint. These muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. The tendon most commonly injured within the rotator cuff is the supraspinatus.4 Risk factors include older age, repetitive overhead activity, whether work- or sport-related, anatomic variants, instability of the glenohumeral joint, and periscapular muscle weakness and imbalance.5–7 The latter are common in people with underlying neurologic diseases.
Patients complain of shoulder pain that is aggravated by arm movement, especially overhead. Painful daily activities may include putting on a shirt or brushing hair. The pain may be localized to the deltoid area, but may also radiate upward toward the neck or distally down the arm, thus mimicking cervical radiculopathy, most often in a C5–C7 distribution. Often, patients have difficulty sleeping on the side of the affected shoulder due to pain.
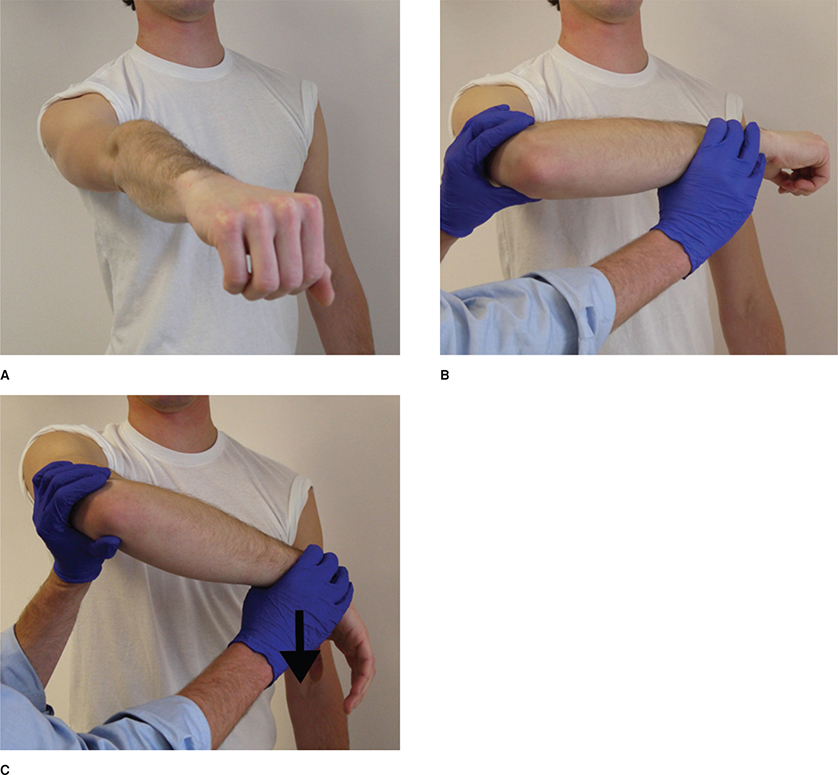
Shoulder examination includes inspection, range of motion (ROM), strength testing, palpation, and special tests.8 With long-standing rotator cuff tendinopathy, inspection may reveal atrophy of the supra- and infraspinatus muscles. ROM above 90 degrees of abduction, either actively or passively, is often painful. Active ROM may be limited by pain, but passive ROM is preserved. There may be tenderness to palpation over the affected muscles or focal subacromial tenderness at the posterolateral border of the acromion. Pain may also be elicited by one of the many special tests that are available to examine the shoulder.8,9 A simple and sensitive screening test for supraspinatus tendinopathy is the Hawkins test (Fig. 36-1). Reduced passive ROM and weakness with resisted abduction and/or external rotation suggest the presence of adhesive capsulitis and rotator cuff tear, respectively. Musculoskeletal ultrasound and magnetic resonance imaging (MRI) can be considered if further investigation and confirmation of the etiology are desired.10
Figure 36-1. Hawkins test. Correct positioning is important to perform the test. The patient forward flexes the arm to 90 degrees (A) and the examiner flexes the elbow to 90 degrees (B). The examiner then forcibly internally rotates the shoulder (C). The maneuver drives the greater tuberosity of the humerus farther under the coracoacromial ligament. Pain with this maneuver is considered positive for impingement of the supraspinatus tendon under the acromion.
Conservative treatment for supraspinatus tendinopathy includes rest, activity modification, ice, nonsteroidal anti-inflammatory drugs (NSAIDs), and physical therapy. Physical therapy is directed to preserving ROM while restoring proper muscle activation and strength balance among the muscles of the rotator cuff.11,12 A subacromial steroid injection may reduce pain and enable earlier participation in ROM exercises and rehabilitation.13 Referral to orthopedics, physiatry, or rheumatology for further diagnostic and therapeutic management is warranted if there is no response to several weeks of conservative management or if additional pathology is suspected.
Biceps tendinopathy is a common cause of anterior shoulder pain and can mimic C5/C6 cervical radiculopathy.
The tendon of the long head of the biceps, with its synovial lining, lies within the bicipital groove which is located in the anterior upper humerus and is bordered laterally by the greater tuberosity and medially by the lesser tuberosity. The bicipital groove is easily palpable in the anterior upper arm when the arm is externally rotated (Fig. 36-2). Tendinopathy occurs where the tendon passes through the bicipital groove and over the head of the humerus just like a rope through a pulley. The underlying pathology may involve inflammation of the tendon and tendon sheath (tendonitis, tenosynovitis) and/or chronic overuse injury and degeneration (tendinosis).14
Figure 36-2. Yergason test. The long head of the biceps tendon is palpated for tenderness in the bicipital groove, between the greater and lesser tuberosities of the humeral head. Localization of the bicipital groove is aided by internally and externally rotating the shoulder with the elbow flexed at 90 degrees while feeling for the tuberosities.
Affected individuals complain of a deep, throbbing ache in the anterior shoulder. Tenderness is usually localized to the bicipital groove, but may radiate to the deltoid region or downward to the anterolateral arm making it difficult to distinguish from upper cervical radicular pain. The pain often worsens at night, especially if sleeping on the affected side, and may increase with lifting, pulling, or repetitive overhead reaching. The risk of developing biceps tendinopathy increases with age and is higher in people who routinely perform activities that require repetitive overhead movements. Importantly, biceps tendinopathy often coexists with other pathologies of the shoulder, including rotator cuff tendinopathy and tears, as well as intra-articular injuries such as a labral tear.15,16
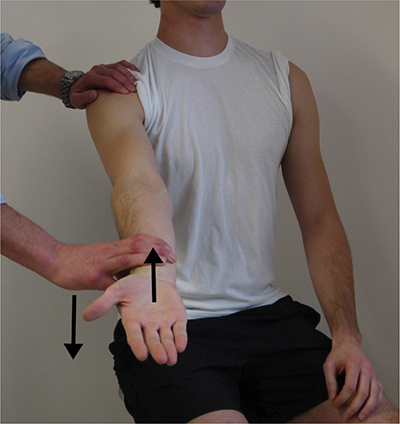
Clinical diagnosis includes assessing for Yergason test, which is tenderness identified by palpation of the long head of the biceps tendon in the bicipital groove while internally and externally rotating the humerus (Fig. 36-2).17 Another helpful test is the Speed test.18 For the Speed test, the patient is asked to flex the arm (lift upward) against resistance from the examiner with the elbow extended and the forearm fully supinated (Fig. 36-3). The test is considered positive when pain is localized to the bicipital groove, implying biceps tendonitis and/or tenosynovitis. Of note, the Speed test may be positive with other shoulder degenerative pathologies. Ultrasound19 and/or MRI20 are not needed for the diagnosis of biceps tendinopathy, but may be considered in patients who are suspected of having additional concurrent shoulder pathologies or are refractory to treatment.
Figure 36-3. Speed test. The patient is asked to flex the shoulder against resistance from the examiner while the elbow is extended and the forearm is supinated. The test is positive for biceps tendon pathology when pain is localized to the bicipital groove.
Conservative treatment is appropriate for most patients with biceps tendinopathy.21,22 Treatment includes rest and activity modification to allow the tendon to heal. Oral or topical NSAIDs and modalities, such as ice therapy, help reduce pain and inflammation. The superficial location of the biceps tendon as it runs through the bicipital groove makes it particularly amenable to ice massage. Patients can be instructed to ice the tender area by directly applying ice to the skin using gentle stroking motions (“ice massage”). The paper cup method is a comfortable, convenient, and inexpensive method of performing ice massage. Water is frozen in a paper cup and ice is exposed by tearing the top rim of paper (Fig. 36-4). Ice is then applied to the affected area multiple times a day until the area is numb, which usually occurs within 5 minutes.
Figure 36-4. Frozen paper cup for ice therapy. A paper cup is filled with water and placed in a freezer. When the water is frozen, the top of the cup can be peeled away to expose the ice. Ice massage is then performed by placing the cup over the injury in a circular pattern allowing the ice to melt away.
If symptoms do not improve with use of rest, activity modification, NSAIDs, and ice therapy, referral to a musculoskeletal medicine expert (from physiatry, sports medicine or orthopedic surgery) may be considered. Physical therapy is used to improve muscle strength and tendon stability. An ultrasound-guided injection of steroid in the biceps tendon sheath is an option for both diagnostic and therapeutic purposes.23,24 Ultrasound guidance is needed to avoid injecting the tendon with resulting risk of rupture. Surgical intervention is used only in selected patients and includes tenotomy and tenodesis.20,25
Lateral epicondylitis (colloquially known as “tennis elbow”) is a common tendinopathy that presents as lateral elbow pain. Pain may radiate distally along the forearm, mimicking C6 cervical radiculopathy or ulnar neuropathy.
The lateral epicondyle of the humerus is located lateral to the olecranon process and is the origin of the wrist and finger extensors. Overuse and poor mechanics can lead to an overload of the extensor tendons.26,27 The underlying pathology is not inflammatory, but rather degenerative and consists of tendon microtearing.28 Pathology most often involves the extensor carpi radialis brevis, approximately 1–2 cm distal to the attachment to the lateral epicondyle, but can affect the other extensors as well.
In most cases, the pain begins shortly after a period of overuse and slowly worsens over weeks and months. There is usually no specific injury associated with the start of symptoms. The point of maximal pain and tenderness is typically located just distal to the lateral epicondyle over the extensor tendon mass, however pain can extend into the distal forearm mimicking C6 radiculopathy. Pain is exacerbated by arm use, especially repetitive wrist extension and pronation/supination activities. There may be perceived weakness in grip strength. Lateral epicondylitis is most often associated with tennis and other racquet sports. Poor technique including improper backhand, string tension, and grip size are contributing factors.29 However, any activity that places excessive repetitive stress on the lateral forearm musculature can cause this condition.30,31
Clinical diagnosis includes assessing for tenderness by palpation over the lateral epicondyle and 1–2 cm distal to it over the common extensor tendon which usually represents the point of maximal tenderness in lateral epicondylitis. The provocative maneuver or “tennis elbow test” consists of resisted radial wrist extension with the forearm in pronation (Fig. 36-5). The examiner stabilizes the elbow with a thumb over the lateral epicondyle. The test is positive if pain is elicited when the patient makes a fist and extends the wrist against resistance by the examiner. The pain is usually worse with the elbow in extension than with the elbow in flexion. Imaging is generally not needed to diagnose this condition, but a plain x-ray of the elbow may be considered to rule out intra-articular pathology and/or loose body fragments. In addition, an x-ray may reveal calcification over the lateral epicondyle. Ultrasound and MRI may be considered if there is no response to conservative treatment.
Figure 36-5. Tennis elbow test. The examiner stabilizes the elbow while palpating along the lateral epicondyle. With the elbow pronated and a closed fist, the patient extends the wrist against the examiner’s resistance. The point of maximal tenderness is generally located one fingerbreadth distal to the lateral epicondyle over the extensor tendon mass. The pain is usually worse with the elbow in extension than with the elbow in flexion.
Despite the prevalence of lateral epicondylitis and the availability of different treatment options, only few high-quality clinical trials are available to support evidence-based management algorithms for this condition. Activity modification is an important first step in management and includes correcting training or technique errors such as grip size of the tennis racket when appropriate. Initial conservative management also includes pain control by using a short course of topical or oral NSAIDs32 and ice massage (as described above). Wrist extensor stretching (Fig. 36-6)33 and bracing34 are often helpful. Bracing consists of using a counterforce elbow strap. Elbow or “tennis straps” are placed on the forearm a few centimeters distal to the elbow joint, are easy to use and inexpensive. Counterforce bracing may reduce tendon and muscle strain at the origin of the forearm extensor muscles, thus relieving pain during activities. Physical therapy has been found to be effective in lateral epicondylitis.35,36 Therapy includes progressive isometric and eccentric strengthening and incorporates stretching and modalities as needed. Eccentric exercise occurs when muscles contract while lengthening. Application of this technique for lateral epicondylitis involves contracting the wrist extensors against the resistance of an exercise band.37,38 Steroid injections have also been used to treat “tennis elbow.”39 Their use, however, is controversial.40 Trials have found that corticosteroid injections improve short-term outcomes in lateral epicondylitis, but do not prevent recurrence and may actually lead to worse long-term outcomes.36,41,42
Figure 36-6. Wrist extensor stretch.
De Quervain syndrome is a common cause of wrist pain and can mimic carpal tunnel syndrome, C6 cervical radiculopathy, and superficial radial sensory neuropathy.
De Quervain syndrome is the most common tenosynovitis of the wrist. It results from inflammation of the fluid-filled sheath (synovium) that surrounds the tendons of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) in the first dorsal compartment of the wrist. These tendons run over the dorsal aspect of the radial styloid process.
The exact causes of De Quervain syndrome are unclear, but they probably include shear and repetitive microtrauma. Postures where the thumb is held in abduction and extension are considered predisposing factors43,44 although evidence regarding a possible relation with certain occupations is controversial. A systematic review of potential risk factors did not find evidence of an association with specific occupation-related activities.45 Women are affected more than men46 and the syndrome commonly occurs during and after pregnancy, due to hormonal changes and possibly lifting the newborn repetitively in a cradled position thus putting stress on the wrist and thumb. Because of the latter postulated risk factor, De Quervain syndrome is also known as “mother’s wrist.”
Patients with this condition present with insidious onset of pain over the dorsal radial aspect of the wrist which may be accompanied by swelling. The pain may radiate distally into the thumb or proximally along the radial aspect of the forearm. Symptoms are exacerbated by grasping or ulnar deviation of the wrist.
De Quervain syndrome can be easily diagnosed on physical examination. Patients usually have tenderness to palpation over the dorsal radial wrist. Finkelstein test is pathognomonic for the condition (Fig. 36-7). To perform the test, the patient is first asked to wrap the fingers around the thumb. To avoid having tight finger flexor tendons splint and immobilize the wrist, it is helpful to ask the patient to wrap the fingers around the thumb lightly, as if the thumb were an egg. The examiner then ulnarly deviates the wrist. A positive test occurs when the patient experiences sharp and intense pain over the radial styloid process, exactly where the tendon sheath takes its course. De Quervain tenosynovitis is a clinical diagnosis and imaging is not needed.
Figure 36-7. Finkelstein test. The patient is asked to make a fist over the thumb. The examiner ulnarly deviates the wrist. A positive test is indicated by exquisite pain in the region of the radial styloid.
Conservative treatment includes rest, ice, anti-inflammatory medications (oral or topical), steroid injections, and a thumb spica splint. The splint is worn during the day, but the patient should remove it several times a day to perform gentle ROM exercises to prevent the complications of prolonged immobilization. Iontophoresis can help with inflammation and pain control. Steroid injections are very effective in providing pain relief and have a favorable side effect profile.47 They work best when used in conjunction with a thumb spica splint.48 Ultrasound guidance for steroid injection is recommended to more precisely localize the site of injection.49 Surgery is rarely indicated and carries a small risk of injury to the superficial radial nerve.50
Carpometacarpal (CMC) joint osteoarthritis (OA) (colloquially known as “thumb arthritis”) is a common cause of hand pain and can mimic carpal tunnel syndrome.
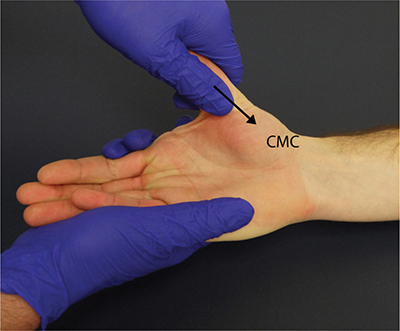
The CMC joint of the thumb connects the trapezium to the first metacarpal bone and plays an important role in the normal functioning of the thumb (Fig. 36-8). Degenerative changes in this joint result in “thumb arthritis” which can cause severe hand pain, swelling, decreased ROM, and reduced grip strength.51 Pain and swelling occur at the base of the thumb. The discomfort is exacerbated by activities that involve using the thumb to apply force or grasping an object. Thumb arthritis can make it difficult to perform simple household tasks, such as opening jars, pulling a zipper, and turning doorknobs.52 Patients may complain of reduced grip strength.52
Figure 36-8. Thumb osteoarthritis. The location of the first CMC joint at the base of the thumb is demonstrated in the figure. The grind test is performed by gripping the metacarpal bone of the thumb, loading it with axial forces to push it against the carpal bone (trapezium), and rotating it in circular motion.
The condition is more common in postmenopausal women.53 Risk factors include genetic predisposition,54 history of prior trauma to the joint, occupations involving repetitive thumb use,55 history of rheumatoid arthritis or articular hypermobility,56 and the presence of OA in other joints.57,58
Thumb OA can be easily diagnosed by using the grind test (Fig. 36-8).59 The examiner holds the wrist in one hand and grasps the first metacarpal bone in the other hand. Axial pressure toward the wrist is applied while rotating the metacarpal bone in a wide circular arc, resulting in compression of the CMC joint. The test is considered positive if the patient reports pain at the base of the thumb. In a positive test, the examiner will also note a grinding or catch sensation while rotating the metacarpal bone in the circular arc. In addition, the CMC joint may appear enlarged from osteoarthritic hypertrophy. Radiographic evaluation has higher sensitivity than the grind test, but the presence of radiographic OA only has a modest association with clinical symptoms such as hand pain and disability.60
Treatment for thumb arthritis includes both nonsurgical and surgical options. Activity modification can be tried first to reduce the activities that most exacerbate pain. As an example, one can use pens with a bigger grip, change door knobs to latches, and use jar openers. Splints can be effective in early stages and can be used at night and/or during the day depending on the patient’s job and needs. Different splints are available to support the thumb, place the joint in a resting position, and decrease pain.61–63 No one splint is superior to the other. Customized braces may provide a better fit and have been associated with improved outcomes, but are more expensive.62 Oral acetaminophen and NSAIDs can be used to manage pain. If a combination of splinting and oral medications is not effective, an intra-articular steroid injection can reduce inflammation and provide pain relief for a few months.64,65 In severe cases, surgical treatment may be needed and includes different procedures that are tailored to the extent of arthritic involvement.66 Surgery may include metacarpal osteotomy, trapeziectomy, arthrodesis (joint fusion), and arthroplasty67 (joint replacement). Recovery after surgery includes 6 weeks of bracing and about 3 months of hand therapy to work on ROM and flexibility of the thumb.68 Most patients regain their strength and return to normal activities at the 6-month time point.
TOP MIMICS IN THE LOWER LIMBSHip OA is a common69 cause of hip, groin, and thigh pain and can mimic L2/3/4 radiculopathy.
The characteristic symptoms of hip OA include anterior hip and groin pain that is exacerbated by weight bearing/physical activity and improves with rest. These characteristics help differentiate hip OA from greater trochanteric bursitis which presents with lateral hip pain aggravated by direct pressure. The pain of hip OA can radiate down the thigh and may also involve the groin area, knee region, and buttock area. Patients may complain of difficulty walking and leg “stiffness.” The pain can either be stabbing and sharp or it can be a dull ache. While the causes of hip OA are not completely known, risk factors include increasing age, genetic predisposition, prior hip injury or developmental deformities, heavy manual labor, participation in weight-bearing sports, and being overweight.70–73
The key clinical finding suggestive of hip OA on examination is the ability to reproduce the patient’s pain when ranging the femur into full internal rotation (Fig. 36-9).74 Furthermore, with hip OA, internal rotation is generally limited more than external rotation. The reason underlying these findings is that sharp forceful internal rotation of the femur compresses the joint space, approximating the bony acetabulum and femoral head, which is uncomfortable when the articular cartilage is degenerated. External rotation is generally better tolerated. Patients may also develop an antalgic gait because they tend to spend a shorter time weight bearing on the affected side due to pain. Diagnosis can be confirmed by weight-bearing anteroposterior (AP) pelvis x-ray to assess the articular width of the hip joints. Joint space narrowing, sclerosis of the joint space margins, and periarticular osteophyte formation are consistent with OA.75 An ultrasound-guided intra-articular anesthetic and/or steroid injection can be a valuable diagnostic tool when there are questions about the location of the pain generator.76,77
Figure 36-9. Hip internal and external rotation. Hip external rotation (A) is not typically associated with pain in hip osteoarthritis, whereas hip internal rotation (B) does reproduce the patient’s pain. Hip range of motion can be tested in a sitting position, as demonstrated here, or with the patient lying down on the examination table.
Treatment of hip OA starts with education about joint protection, weight loss (if appropriate), use of modalities for pain reduction, physical therapy78,79 to preserve strength and ROM, and use of mobility aids as needed.80,81 A cane held on the nonaffected side helps to off load the affected hip resulting in improved pain and gait mechanics. Pharmacologic treatment includes acetaminophen, NSAIDs, and ultrasound-guided intra-articular steroid injections.82 Surgical intervention (either hip resurfacing or replacement) followed by rehabilitation may ultimately be needed to ensure optimal pain control and function in advanced cases.81
Greater trochanteric bursitis causes lateral hip/thigh pain and can mimic L3/L4/L5 radiculopathy.83
Greater trochanteric bursitis presents as tenderness to palpation over the greater trochanter, in the lateral hip and thigh.84,85 Some prefer the term “greater trochanteric pain syndrome,” which may be more accurate because the etiology of this condition is not fully understood. The pain generator may be related to an inflammation of the trochanteric bursa located on the outer side of the femur. However, contributing pain generators may include the gluteus medius and gluteus minimus muscles, their attachments into the greater trochanter of the femur and the femoral shaft, and overlying tissue such as the iliotibial (IT) band.86–89 All of these structures are associated with the greater trochanter and may be affected by abnormal lower limb biomechanics and disturbances in gait, which are common occurrences in people with underlying neurologic diseases.83,90–92 Gait abnormalities affect the biomechanics around the greater trochanter and lead to altered pressure on the bursae and friction in the tendons and other soft tissue structures, which ultimately result in local pain and tenderness.90
Patients typically complain of lateral hip pain that may radiate into the buttock and outer thigh into the knee. Patients may rub their thigh when describing the pain. The pain is characteristically exacerbated by direct pressure to the point that patients may describe intolerance to sleeping on the affected side. Pain can also be aggravated by walking, especially climbing stairs and can be disabling with a negative impact on quality of life.93
The diagnosis is based on history and clinical findings of exquisite pain on direct palpation of the region of the greater trochanter.94 Palpation can be performed in the lateral decubitus position with the affected side placed upward. The trochanteric process is the most prominent portion of the femur. Side-to-side comparison can be easily accomplished by palpating the outer thighs and hips with the patient in a seated position facing the examiner (Fig. 36-10). The examiner palpates along the lateral femurs from distal to proximal until reaching the greater trochanters (Fig. 36-10). Note that palpation of the lateral thigh can elicit some discomfort in people with tight IT bands. However, when trochanteric bursitis is present, direct palpation will elicit prominent sharp pain that reproduces the patient’s pain.
Figure 36-10. Greater trochanter palpation. To localize the greater trochanter, the examiner palpates the lateral thigh starting distally (arrows) and moving proximally until the greater trochanter of the femur is identified (as indicated by the examiner in the picture). Palpating the greater trochanter will elicit pain in patients with greater trochanteric bursitis. Performing the maneuver in sitting, as demonstrated here, allows a quick side-to-side comparison. Note that palpation of the lateral thigh can elicit some discomfort in people with tight iliotibial bands. However, when greater trochanteric bursitis is present, there will be additional, sharp pain localized to the greater trochanter. The maneuver can also be performed with the patient lying down on the examination table and the affected leg placed upward. Lying down on the side of the affected leg produces exquisite pain in patients with greater trochanteric bursitis.
Pain relief with local anesthetic and/or steroid injection corroborates the diagnosis and provides excellent pain relief.95,96 Plain radiographs of the hip can be performed to exclude structural abnormalities, while ultrasound and MRI can be considered in refractory cases.87
NSAIDs and ice therapy help relieve pain and reduce the inflammation. Ice therapy to the lateral hip every 4–6 hours can be accomplished by ice massage with a paper cup (Fig. 36-4) or by using flexible frozen gels or a bag of frozen peas against the hip to cover a larger area. Typical, uncomplicated greater trochanteric pain syndrome responds very well to local injections of an anesthetic and/or steroid.91,95,96 The pain may actually worsen for 1 or 2 days immediately following the procedure before improving. Injection aftercare is critical to the success of the injection. The patient should rest, avoid direct pressure and repetitive bending, and use NSAIDs and ice as needed for pain relief. In order to help prevent recurrence, predisposing factors should be addressed as much as possible. Physical therapy can be helpful to stretch the back and IT band and strengthening the hip muscles can relieve tension in the hip and reduce friction. Daily stretches should be incorporated into an individualized home exercise program (HEP) for best results. Stretches are most effective and best tolerated after the steroid injection of the bursae has been performed.
Bursitis is a common cause of lower extremity pain. Pes anserine bursitis presents as medial knee and leg pain and can mimic L4 lumbar radiculopathy.
The pes anserinus (“goose’s foot”) is the insertion of the conjoined tendons of three muscles (semitendinosus, sartorius, and gracilis) onto the anteromedial surface of the proximal tibia. It lies superficial to the superficial fibers of the medial collateral ligament (MCL) of the knee. Inflammation of the anserine bursa that lies just under the tendons near their insertion is termed pes anserine bursitis.97
Pes anserine bursitis should be suspected when pain occurs in the medial knee region over the upper tibia.98 Pain is exacerbated by repetitive knee flexion such as when ascending stairs and climbing. Sports that involve side-to-side cutting activity (e.g., tennis and soccer) as well as underlying knee medial compartment OA and obesity may predispose to bursitis. Muscle imbalances involving the hip adductors, hip flexors, and hamstrings may cause an abnormal pull at the insertion point of the three tendons resulting in pes anserine bursitis.99,100
The diagnosis of pes anserine bursitis is made clinically by direct palpation of the bursa, which elicits localized tenderness (Fig. 36-11). The entire tibial plateau needs to be palpated to differentiate between the localized tenderness of anserine bursitis and medial joint line tenderness from an intra-articular injury. In addition, there may be more extensive tenderness along the medial femoral epicondyle to the medial tibia which is present with MCL injury. Imaging is usually not indicated unless there is suspicion for stress fracture or intra-articular pathology such as meniscal injury or knee OA.
Figure 36-11. Pes anserine bursa. The figure depicts the location of the anserine bursa in the medial leg.
In the acute phase, treatment includes rest, ice massage (as described above), and a short course of topical or oral NSAIDs to reduce the pain and swelling in the bursa. Activity modification to “rest” the bursa include avoiding direct pressure (which can be accomplished at night by using a pillow between the knees) as well as activities such as squatting, repetitive knee bending, and crossing the legs.101 A corticosteroid injection into the bursa can be used both as a diagnostic and therapeutic tool and often provides quick relief.102 A rehabilitation program is needed to treat any underlying cause of anterior to posterior and medial to lateral muscle imbalance. Therapy focuses on maximizing flexibility, strength, and endurance of the muscles whose tendons form the pes anserinus as well as addressing any muscle imbalances of the entire kinetic chain. Core control should be maximized to allow for proper hamstring and hip adductor and flexion function. Running shoes and inserts need to be appropriate for each individual biomechanics characteristics. Surgery (bursectomy) is rarely needed.
Plantar fasciitis is a common cause of plantar foot pain. It can occur on both sides and mimic the pain associated with distal sensory polyneuropathy. It can also present unilaterally mimicking S1 radiculopathy.
The plantar fascia is a band of thick connective tissue that originates on the calcaneus (or heel bone) and fans out on the sole of the foot to connect it to the base of the toes and support the arch of the foot. It is also related to the Achilles tendon, with connecting fibers between the two from the distal aspect of the Achilles tendon to the origin of the plantar fascia at the calcaneal tubercle.103 Poor foot biomechanics can cause increased tension on the fascia and pain. This can occur in patients with pes planus, pes cavus, increased subtalar pronation, limited ankle dorsiflexion, decreased intrinsic foot muscle strength, and tight heel cords, all conditions that place stress on the plantar fascia.104,105 Therefore plantar fasciitis can coexist with many underlying neuromuscular conditions that are associated with foot deformity and weakness. Obesity, pregnancy, and prolonged standing are additional risk factors.104,106
Patients typically describe the worst pain as occurring with weight bearing after getting out of bed in the morning or after a period of inactivity. Pain can be gnawing, stabbing, or burning. History of pain when taking the first steps in the morning helps differentiate this condition from the pain experienced by patients with sensory polyneuropathy whose foot pain is characteristically worse at night when off their feet. In some patients, the pain may radiate to the dorsolateral foot due to the patient offloading the pressure on the heel and walking on the outside of the foot creating an overuse condition to the lateral foot and ankle.
The history and clinical examination are the mainstay of diagnosis. On physical examination there is tenderness to palpation on the medial plantar aspect of the heel bone (Fig. 36-12). This area corresponds to the site of the plantar fascia insertion on the calcaneus. Palpation of the medial slip of the plantar fascia may also reveal tightness and discomfort (Fig. 36-13), but the area of maximal tenderness corresponds to the medial tubercle of the calcaneus (Fig. 36-12). Discomfort in the proximal plantar fascia can also be elicited by passive ankle and toe dorsiflexion. Diagnostic imaging is rarely needed for the initial diagnosis. Ultrasound and MRI are reserved for cases that do not respond to treatment or to exclude other heel pathology.107,108 Plain x-rays of the foot can reveal a calcaneal heel spur in many individuals.108 The heel spur, however, is not pathognomonic of plantar fasciitis and is not the cause of pain in this condition. Rather, the heel spur is thought to represent a byproduct of the chronic pulling of the fascia off the calcaneus and exists in many patients without symptoms of plantar fasciitis.
Figure 36-12. Medial calcaneus palpation. This maneuver reveals the area of maximal tenderness in plantar fasciitis at the site of the plantar fascia insertion on the heel bone (shaded area).
Figure 36-13. Plantar fascia palpation. Palpating the plantar fascia in the arch of the foot can elicit pain in people with plantar fasciitis.
Plantar fasciitis is a self-limiting condition that usually improves within 1 year regardless of treatment. Conservative treatment usually starts with patient-directed therapies. If these are not effective within a few weeks to a few months, management is advanced to include physician-prescribed interventions.
Initial patient-directed modalities include rest, activity modification, ice massage, oral analgesics (acetaminophen or NSAIDs), and stretching.109,110 Ice massage is performed by having the patient roll the arch of the foot over a frozen soda can or plastic bottle until numb. Treatment can be repeated multiple times a day. Stretching is performed both in bed before getting up in the morning and several times during the day. Before getting up, the patient is asked to stretch the Achilles tendon by dorsiflexing the foot and holding on to it for at least 30 seconds. This exercise is repeated 10 times and can be modified by including a large towel if limited flexibility prevents the patient from reaching the foot. While seated, the patient is also asked to stretch the plantar fascia by dorsiflexing the toes, holding the metatarsophalangeals and stretching the fascia in the arch region. During the day, the patient may stretch by leaning against a wall and performing wall leans, alternating between knee bent and knee extended while the heel is on the ground. Again each stretch is held for a minimum of 30 seconds and repeated several times. Intrinsic foot and calf strengthening exercises can help as well.
If pain persists, physician-prescribed treatments should be considered. These include shoe inserts, night splinting, physical therapy, and corticosteroid injections. Shoe inserts are commonly recommended for people with plantar fasciitis to aid in limiting overpronation of the foot and to unload the tensile forces on the plantar fascia. These include heel cups, prefabricated longitudinal arch supports, and custom-made full-length shoe insoles.111–113 Night splints can be used to prevent foot plantar flexion during sleep by keeping the foot and ankle in a neutral 90-degree position. Night splints have been shown to improve plantar fasciitis pain,113 but poor compliance because of sleep disturbance and foot discomfort has limited their long-term use. Multiple physical therapy modalities may be used, often in combination. Deep myofascial massage and iontophoresis can be performed by a physical therapist. In iontophoresis, electrical pulses are used to cause absorption of topical medications into the soft tissues beneath the skin. A small study found iontophoresis of acetic acid or dexamethasone to be helpful in plantar fasciitis.114 Corticosteroid injections have been found to be effective in the treatment of plantar fasciitis and may be part of the initial approach in patients who desire an expedited return to normal activity.115,116 Possible risks associated with corticosteroid injection include fat pad atrophy and plantar fascia rupture. In recent years, platelet-rich plasma injections have been proposed as an alternative treatment for plantar fasciitis and are currently being tested in clinical trials to determine their efficacy.117,118 Patients with recalcitrant plantar fasciitis can consider extracorporeal shock wave therapy (ESWT) or, as a last resort, plantar fasciotomy. ESWT is thought to promote neovascularization and induce tissue repair. The technique is commonly used as it is noninvasive and has a good side effect profile although clinical trials have resulted in conflicting evidence.119–122
SUMMARYMusculoskeletal disorders are a common cause of limb pain and are likely to be encountered in daily practice, whether in the neuromuscular clinic or in the EMG laboratory. Musculoskeletal problems can “mimic” radiculopathy or entrapment neuropathy, thus posing a diagnostic challenge. In addition, musculoskeletal pain can complicate chronic neuromuscular diseases such as motor neuron disease and muscular dystrophy. Importantly, many common musculoskeletal problems can be diagnosed quickly at the bedside and are eminently treatable. Therefore, their prompt recognition has the potential to improve clinical flow and patient outcomes.
ACKNOWLEDGMENTSWe would like to thank Farah Hameed, MD (Columbia University Medical Center, Department of Rehabilitation and Regenerative Medicine) for helpful comments and suggestions, and Andrew Sandefer (EMG Laboratory, VA Boston Healthcare) for technical assistance during the drafting of this chapter.
1. Cannon DE, Dillingham TR, Miao H, Andary MT, Pezzin LE. Musculoskeletal disorders in referrals for suspected cervical radiculopathy. Arch Phys Med Rehabil. 2007;88:1256–1259.
2. Cannon DE, Dillingham TR, Miao H, Andary MT, Pezzin LE. Musculoskeletal disorders in referrals for suspected lumbosacral radiculopathy. Am J Phys Med Rehabil. 2007;86:957–961.
3. Stockard AR1, Allen TW. Competence levels in musculoskeletal medicine: comparison of osteopathic and allopathic medical graduates. J Am Osteopath Assoc. 2006;106(6):350–355.
4. Fu FH, Harner CD, Klein AH. Shoulder impingement syndrome. A critical review. Clin Orthop Relat Res. 1991;269:162–173.
5. Yi Y, Shim JS, Kim K, et al. Prevalence of the rotator cuff tear increases with weakness in hemiplegic shoulder. Ann Rehabil Med. 2013;37:471–478.
6. Gumina S, Carbone S, Campagna V, Candela V, Sacchetti FM, Giannicola G. The impact of aging on rotator cuff tear size. Musculoskelet Surg. 2013;97(suppl 1):69–72.
7. Bodin J, Ha C, Petit Le Manac’h A, et al. Risk factors for incidence of rotator cuff syndrome in a large working population. Scand J Work Environ Health. 2012;38:436–446.
8. Jain NB, Wilcox RB 3rd, Katz JN, Higgins LD. Clinical examination of the rotator cuff. PM R. 2013;5:45–56.
9. Hegedus EJ, Goode AP, Cook CE, et al. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med. 2012;46:964–978.
10. Teefey SA, Rubin DA, Middleton WD, Hildebolt CF, Leibold RA, Yamaguchi K. Detection and quantification of rotator cuff tears. Comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic findings in seventy-one consecutive cases. J Bone Joint Surg Am. 2004;86-A:708–716.
11. Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev. 2003;(2): CD004258.
12. Gebremariam L, Hay EM, van der Sande R, Rinkel WD, Koes BW, Huisstede BM. Subacromial impingement syndrome–effectiveness of physiotherapy and manual therapy. Br J Sports Med. 2014;48(16):1202–1208.
13. Dogu B, Yucel SD, Sag SY, Bankaoglu M, Kuran B. Blind or ultrasound-guided corticosteroid injections and short-term response in subacromial impingement syndrome: A randomized, double-blind, prospective study. Am J Phys Med Rehabil. 2012;91:658–665.
14. Mazzocca AD, McCarthy MB, Ledgard FA, et al. Histomorphologic changes of the long head of the biceps tendon in common shoulder pathologies. Arthroscopy. 2013;29:972–981.
15. Beall DP, Williamson EE, Ly JQ, et al. Association of biceps tendon tears with rotator cuff abnormalities: Degree of correlation with tears of the anterior and superior portions of the rotator cuff. AJR Am J Roentgenol. 2003;180:633–639.
16. Murthi AM, Vosburgh CL, Neviaser TJ. The incidence of pathologic changes of the long head of the biceps tendon. J Shoulder Elbow Surg. 2000;9:382–385.
17. Gazzillo GP, Finnoff JT, Hall MM, Sayeed YA, Smith J. Accuracy of palpating the long head of the biceps tendon: An ultrasonographic study. PM R. 2011;3:1035–1040.
18. Bennett WF. Specificity of the Speed’s test: Arthroscopic technique for evaluating the biceps tendon at the level of the bicipital groove. Arthroscopy. 1998;14:789–796.
19. Chen HS, Lin SH, Hsu YH, Chen SC, Kang JH. A comparison of physical examinations with musculoskeletal ultrasound in the diagnosis of biceps long head tendinitis. Ultrasound Med Biol. 2011;37:1392–1398.
20. Schaeffeler C, Waldt S, Holzapfel K, et al. Lesions of the biceps pulley: Diagnostic accuracy of MR arthrography of the shoulder and evaluation of previously described and new diagnostic signs. Radiology. 2012;264:504–513.
21. Longo UG, Loppini M, Marineo G, Khan WS, Maffulli N, Denaro V. Tendinopathy of the tendon of the long head of the biceps. Sports Med Arthrosc. 2011;19:321–332.
22. Snyder GM, Mair SD, Lattermann C. Tendinopathy of the long head of the biceps. Med Sport Sci. 2012;57:76–89.
23. Zhang J, Ebraheim N, Lause GE. Ultrasound-guided injection for the biceps brachii tendinitis: Results and experience. Ultrasound Med Biol. 2011;37:729–733.
24. Hashiuchi T, Sakurai G, Morimoto M, Komei T, Takakura Y, Tanaka Y. Accuracy of the biceps tendon sheath injection: Ultrasound-guided or unguided injection? A randomized controlled trial. J Shoulder Elbow Surg. 2011;20:1069–1073.
25. Galasso O, Gasparini G, De Benedetto M, Familiari F, Castricini R. Tenotomy versus tenodesis in the treatment of the long head of biceps brachii tendon lesions. BMC Musculoskelet Disord. 2012;13:205.
26. Chourasia AO, Buhr KA, Rabago DP, et al. Relationships between biomechanics, tendon pathology, and function in individuals with lateral epicondylosis. J Orthop Sports Phys Ther. 2013;43:368–378.
27. Lucado AM, Kolber MJ, Cheng MS, Echternach JL Sr. Upper extremity strength characteristics in female recreational tennis players with and without lateral epicondylalgia. J Orthop Sports Phys Ther. 2012;42:1025–1031.
28. Regan W, Wold LE, Coonrad R, Morrey BF. Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med. 1992;20:746–749.
29. Abrams GD, Renstrom PA, Safran MR. Epidemiology of musculoskeletal injury in the tennis player. Br J Sports Med. 2012;46:492–498.
30. Titchener AG, Fakis A, Tambe AA, Smith C, Hubbard RB, Clark DI. Risk factors in lateral epicondylitis (tennis elbow): A case-control study. J Hand Surg Eur. 2013;38:159–164.
31. Shiri R, Viikari-Juntura E, Varonen H, Heliovaara M. Prevalence and determinants of lateral and medial epicondylitis: A population study. Am J Epidemiol. 2006;164:1065–1074.
32. Pattanittum P, Turner T, Green S, Buchbinder R. Non-steroidal anti-inflammatory drugs (NSAIDs) for treating lateral elbow pain in adults. Cochrane Database Syst Rev. 2013;5:CD003686.
33. Sölveborn SA. Radial epicondylalgia (‘tennis elbow’): Treatment with stretching or forearm band. A prospective study with long-term follow-up including range-of-motion measurements. Scand J Med Sci Sports. 1997;7:229–237.
34. Sadeghi-Demneh E, Jafarian F. The immediate effects of orthoses on pain in people with lateral epicondylalgia. Pain Res Treat. 2013;2013:353597.
35. Nilsson P, Baigi A, Swärd L, Möller M, Månsson J. Lateral epicondylalgia: A structured programme better than corticosteroids and NSAID. Scand J Occup Ther. 2012;19(5):404–410.
36. Olaussen M, Holmedal O, Lindbaek M, Brage S, Solvang H. Treating lateral epicondylitis with corticosteroid injections or non-electrotherapeutical physiotherapy: A systematic review. BMJ Open. 2013;3:e003564.
37. Svernlov B, Adolfsson L. Non-operative treatment regime including eccentric training for lateral humeral epicondylalgia. Scand J Med Sci Sports. 2001;11:328–334.
38. Martinez-Silvestrini JA, Newcomer KL, Gay RE, Schaefer MP, Kortebein P, Arendt KW. Chronic lateral epicondylitis: Comparative effectiveness of a home exercise program including stretching alone versus stretching supplemented with eccentric or concentric strengthening. J Hand Ther. 2005;18(4):411–419, quiz 420.
39. Titchener AG, Booker SJ, Bhamber NS, Tambe AA, Clark DI. Corticosteroid and platelet-rich plasma injection therapy in tennis elbow (lateral epicondylalgia): A survey of current UK specialist practice and a call for clinical guidelines. Br J Sports Med. 2013.
40. Krogh TP, Bartels EM, Ellingsen T, et al. Comparative effectiveness of injection therapies in lateral epicondylitis: A systematic review and network meta-analysis of randomized controlled trials. Am J Sports Med. 2013;41:1435–1446.
41. Coombes BK, Bisset L, Brooks P, Khan A, Vicenzino B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: A randomized controlled trial. JAMA. 2013;309:461–469.
42. Krogh TP, Fredberg U, Stengaard-Pedersen K, Christensen R, Jensen P, Ellingsen T. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: A randomized, double-blind, placebo-controlled trial. Am J Sports Med. 2013; 41:625–635.
43. Armstrong TJ, Fine LJ, Goldstein SA, Lifshitz YR, Silverstein BA. Ergonomics considerations in hand and wrist tendinitis. J Hand Surg Am. 1987;12:830–837.
44. Luopajarvi T, Kuorinka I, Virolainen M, Holmberg M. Prevalence of tenosynovitis and other injuries of the upper extremities in repetitive work. Scand J Work Environ Health. 1979; 5(suppl 3):48–55.
45. Stahl S, Vida D, Meisner C, et al. Systematic review and meta-analysis on the work-related cause of de Quervain tenosynovitis: A critical appraisal of its recognition as an occupational disease. Plast Reconstr Surg. 2013;132(6):1479–1491.
46. Hartwell SW Jr, Larsen RD, Posch JL. Tenosynovitis in Women in Industry. Cleve Clin Q. 1964;31:115–118.
47. Ashraf MO, Devadoss VG. Systematic review and meta-analysis on steroid injection therapy for de Quervain’s tenosynovitis in adults. Eur J Orthop Surg Traumatol. 2014;24(2):149–157.
48. Mardani-Kivi M, Karimi Mobarakeh M, Bahrami F, Hashemi-Motlagh K, Saheb-Ekhtiari K, Akhoondzadeh N. Corticosteroid injection with or without thumb spica cast for de quervain tenosynovitis. J Hand Surg Am. 2014;39:37–41.
49. McDermott JD, Ilyas AM, Nazarian LN, Leinberry CF. Ultrasound-guided injections for de Quervain’s tenosynovitis. Clin Orthop Relat Res. 2012;470:1925–1931.
50. Kang HJ, Koh IH, Jang JW, Choi YR. Endoscopic versus open release in patients with de Quervain’s tenosynovitis: A randomised trial. Bone Joint J. 2013;95-B:947–951.
51. Gehrmann SV, Tang J, Li ZM, Goitz RJ, Windolf J, Kaufmann RA. Motion deficit of the thumb in CMC joint arthritis. J Hand Surg Am. 2010;35:1449–1453.
52. Zhang Y, Niu J, Kelly-Hayes M, Chaisson CE, Aliabadi P, Felson DT. Prevalence of symptomatic hand osteoarthritis and its impact on functional status among the elderly: The Framingham Study. Am J Epidemiol. 2002;156:1021–1027.
53. Wilder FV, Barrett JP, Farina EJ. Joint-specific prevalence of osteoarthritis of the hand. Osteoarthritis Cartilage. 2006;14:953–957.
54. Jonsson H, Manolescu I, Stefansson SE, et al. The inheritance of hand osteoarthritis in Iceland. Arthritis Rheum. 2003;48:391–395.
55. Fontana L, Neel S, Claise JM, Ughetto S, Catilina P. Osteoarthritis of the thumb carpometacarpal joint in women and occupational risk factors: A case-control study. J Hand Surg Am. 2007;32:459–465.
56. Jonsson H, Valtysdottir ST, Kjartansson O, Brekkan A. Hypermobility associated with osteoarthritis of the thumb base: A clinical and radiological subset of hand osteoarthritis. Ann Rheum Dis. 1996;55:540–543.
57. Kessler S, Stove J, Puhl W, Sturmer T. First carpometacarpal and interphalangeal osteoarthritis of the hand in patients with advanced hip or knee OA. Are there differences in the aetiology? Clin Rheumatol. 2003;22:409–413.
58. Chaisson CE, Zhang Y, McAlindon TE, et al. Radiographic hand osteoarthritis: Incidence, patterns, and influence of pre-existing disease in a population based sample. J Rheumatol. 1997;24:1337–1343.
59. Merritt MM, Roddey TS, Costello C, Olson S. Diagnostic value of clinical grind test for carpometacarpal osteoarthritis of the thumb. J Hand Ther. 2010;23:261–267; quiz 268.
60. Dahaghin S, Bierma-Zeinstra SM, Ginai AZ, Pols HA, Hazes JM, Koes BW. Prevalence and pattern of radiographic hand osteoarthritis and association with pain and disability (the Rotterdam study). Ann Rheum Dis. 2005;64:682–687.
61. Sillem H, Backman CL, Miller WC, Li LC. Comparison of two carpometacarpal stabilizing splints for individuals with thumb osteoarthritis. J Hand Ther. 2011;24(3):216–225; quiz 126; discussion 227–230.
62. Bani MA, Arazpour M, Kashani RV, Mousavi ME, Hutchins SW. Comparison of custom-made and prefabricated neoprene splinting in patients with the first carpometacarpal joint osteoarthritis. Disabil Rehabil Assist Technol. 2013;8:232–237.
63. Egan MY, Brousseau L. Splinting for osteoarthritis of the carpometacarpal joint: A review of the evidence. Am J Occup Ther. 2007;61:70–78.
64. Maarse W, Watts AC, Bain GI. Medium-term outcome following intra-articular corticosteroid injection in first CMC joint arthritis using fluoroscopy. Hand Surg. 2009;14:99–104.
65. Joshi R. Intraarticular corticosteroid injection for first carpometacarpal osteoarthritis. J Rheumatol. 2005;32:1305–1306.
66. Hentz VR. Surgical treatment of trapeziometacarpal joint arthritis: A historical perspective. Clin Orthop Relat Res. 2014;472(4):1184–1189.
67. Badia A, Sambandam SN. Total joint arthroplasty in the treatment of advanced stages of thumb carpometacarpal joint osteoarthritis. J Hand Surg Am. 2006;31:1605–1614.
68. Ataker Y, Gudemez E, Ece SC, Canbulat N, Gulgonen A. Rehabilitation protocol after suspension arthroplasty of thumb carpometacarpal joint osteoarthritis. J Hand Ther. 2012; 25(4):374–382; quiz 383.
69. Nho SJ, Kymes SM, Callaghan JJ, Felson DT. The burden of hip osteoarthritis in the United States: Epidemiologic and economic considerations. J Am Acad Orthop Surg. 2013;21 (suppl 1):S1–S6.
70. Evangelou E, Kerkhof HJ, Styrkarsdottir U, et al. A meta-analysis of genome-wide association studies identifies novel variants associated with osteoarthritis of the hip. Ann Rheum Dis. 2014;73(12):2130–2136.
71. Richmond SA, Fukuchi RK, Ezzat A, Schneider K, Schneider G, Emery CA. Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. J Orthop Sports Phys Ther. 2013;43:515–B19.
72. Prieto-Alhambra D, Judge A, Javaid MK, Cooper C, Diez-Perez A, Arden NK. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis. 2014;73(9):1659–1664.
73. Franklin J, Ingvarsson T, Englund M, Lohmander S. Association between occupation and knee and hip replacement due to osteoarthritis: A case-control study. Arthritis Res Ther. 2010;12:R102.
74. Chong T, Don DW, Kao MC, Wong D, Mitra R. The value of physical examination in the diagnosis of hip osteoarthritis. J Back Musculoskelet Rehabil. 2013;26:397–400.
75. Xu L, Hayashi D, Guermazi A, et al. The diagnostic performance of radiography for detection of osteoarthritis-associated features compared with MRI in hip joints with chronic pain. Skeletal Radiol. 2013;42:1421–1428.
76. Yoong P, Guirguis R, Darrah R, Wijeratna M, Porteous MJ. Evaluation of ultrasound-guided diagnostic local anaesthetic hip joint injection for osteoarthritis. Skeletal Radiol. 2012;41:981–985.
77. Deshmukh AJ, Thakur RR, Goyal A, Klein DA, Ranawat AS, Rodriguez JA. Accuracy of diagnostic injection in differentiating source of atypical hip pain. J Arthroplasty. 2010;25:129–133.
78. Svege I, Nordsletten L, Fernandes L, Risberg MA. Exercise therapy may postpone total hip replacement surgery in patients with hip osteoarthritis: A long-term follow-up of a randomised trial. Ann Rheum Dis. 2015;74(1):164–169.
79. Jensen C, Roos EM, Kjaersgaard-Andersen P, Overgaard S. The effect of education and supervised exercise vs. education alone on the time to total hip replacement in patients with severe hip osteoarthritis. A randomized clinical trial protocol. BMC Musculoskelet Disord. 2013;14:21.
80. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008;16:137–162.
81. Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology. 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64:465–474.
82. Lambert RG, Hutchings EJ, Grace MG, Jhangri GS, Conner-Spady B, Maksymowych WP. Steroid injection for osteoarthritis of the hip: A randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2007;56:2278–2287.
83. Swezey RL. Pseudo-radiculopathy in subacute trochanteric bursitis of the subgluteus maximus bursa. Arch Phys Med Rehabil. 1976;57:387–390.
84. Schapira D, Nahir M, Scharf Y. Trochanteric bursitis: A common clinical problem. Arch Phys Med Rehabil. 1986;67:815–817.
85. Shbeeb MI, Matteson EL. Trochanteric bursitis (greater trochanter pain syndrome). Mayo Clin Proc. 1996;71:565–569.
86. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001;44:2138–2145.
87. Blankenbaker DG, Ullrick SR, Davis KW, De Smet AA, Haaland B, Fine JP. Correlation of MRI findings with clinical findings of trochanteric pain syndrome. Skeletal Radiol. 2008;37:903–909.
88. Fearon AM, Scarvell JM, Cook JL, Smith PN. Does ultrasound correlate with surgical or histologic findings in greater trochanteric pain syndrome? A pilot study. Clin Orthop Relat Res. 2010;468:1838–1844.
89. Long SS, Surrey DE, Nazarian LN. Sonography of greater trochanteric pain syndrome and the rarity of primary bursitis. AJR Am J Roentgenol. 2013;201:1083–1086.
90. Segal NA, Felson DT, Torner JC, et al; Multicenter Osteoarthritis Study Group. Greater trochanteric pain syndrome: Epidemiology and associated factors. Arch Phys Med Rehabil. 2007;88:988–992.
91. Sayegh F, Potoupnis M, Kapetanos G. Greater trochanter bursitis pain syndrome in females with chronic low back pain and sciatica. Acta Orthop Belg. 2004;70:423–428.
92. Sloan RL. Greater trochanteric pain syndrome, another cause of hip or thigh pain in multiple sclerosis. Pract Neurol. 2009;9:163–165.
93. Fearon AM, Cook JL, Scarvell JM, Neeman T, Cormick W, Smith PN. Greater trochanteric pain syndrome negatively affects work, physical activity and quality of life: A case control study. J Arthroplasty. 2014;29(2):383–386.
94. Karpinski MR, Piggott H. Greater trochanteric pain syndrome. A report of 15 cases. J Bone Joint Surg Br. 1985;67:762–763.
95. McEvoy JR, Lee KS, Blankenbaker DG, del Rio AM, Keene JS. Ultrasound-guided corticosteroid injections for treatment of greater trochanteric pain syndrome: Greater trochanter bursa versus subgluteus medius bursa. AJR Am J Roentgenol. 2013; 201:W313–W317.
96. Brinks A, van Rijn RM, Willemsen SP, et al. Corticosteroid injections for greater trochanteric pain syndrome: A randomized controlled trial in primary care. Ann Fam Med. 2011;9:226–234.
97. Forbes JR, Helms CA, Janzen DL. Acute pes anserine bursitis: MR imaging. Radiology. 1995;194:525–527.
98. Rennie WJ, Saifuddin A. Pes anserine bursitis: Incidence in symptomatic knees and clinical presentation. Skeletal Radiol. 2005;34:395–398.
99. Alvarez-Nemegyei J. Risk factors for pes anserinus tendinitis/bursitis syndrome: A case control study. J Clin Rheumatol. 2007;13:63–65.
100. Devan MR, Pescatello LS, Faghri P, Anderson J. A prospective study of overuse knee injuries among female athletes with muscle imbalances and structural abnormalities. J Athl Train. 2004;39:263–267.
101. Butcher JD, Salzman KL, Lillegard WA. Lower extremity bursitis. Am Fam Physician. 1996;53:2317–2324.
102. Cardone DA, Tallia AF. Diagnostic and therapeutic injection of the hip and knee. Am Fam Physician. 2003;67:2147–2152.
103. Stecco C, Corradin M, Macchi V, et al. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013;223:665–676.
104. Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for Plantar fasciitis: A matched case-control study. J Bone Joint Surg Am. 2003;85-A:872–877.
105. Bolivar YA, Munuera PV, Padillo JP. Relationship between tightness of the posterior muscles of the lower limb and plantar fasciitis. Foot Ankle Int. 2013;34:42–48.
106. Werner RA, Gell N, Hartigan A, Wiggerman N, Keyserling WM. Risk factors for plantar fasciitis among assembly plant workers. PM R. 2010;2:110–116; quiz 1 p following 167.
107. Karabay N, Toros T, Hurel C. Ultrasonographic evaluation in plantar fasciitis. J Foot Ankle Surg. 2007;46:442–446.
108. McMillan AM, Landorf KB, Barrett JT, Menz HB, Bird AR. Diagnostic imaging for chronic plantar heel pain: A systematic review and meta-analysis. J Foot Ankle Res. 2009;2:32.
109. Donley BG, Moore T, Sferra J, Gozdanovic J, Smith R. The efficacy of oral nonsteroidal anti-inflammatory medication (NSAID) in the treatment of plantar fasciitis: A randomized, prospective, placebo-controlled study. Foot Ankle Int. 2007;28:20–23.
110. Digiovanni BF, Nawoczenski DA, Malay DP, et al. Plantar fascia-specific stretching exercise improves outcomes in patients with chronic plantar fasciitis. A prospective clinical trial with two-year follow-up. J Bone Joint Surg Am. 2006;88:1775–1781.
111. Lee SY, McKeon P, Hertel J. Does the use of orthoses improve self-reported pain and function measures in patients with plantar fasciitis? A meta-analysis. Phys Ther Sport. 2009;10:12–18.
112. Hawke F, Burns J, Radford JA, du Toit V. Custom-made foot orthoses for the treatment of foot pain. Cochrane Database Syst Rev. 2008;3:CD006801.
113. Roos E, Engstrom M, Soderberg B. Foot orthoses for the treatment of plantar fasciitis. Foot Ankle Int. 2006;27:606–611.
114. Osborne HR, Allison GT. Treatment of plantar fasciitis by LowDye taping and iontophoresis: Short term results of a double blinded, randomised, placebo controlled clinical trial of dexamethasone and acetic acid. Br J Sports Med. 2006;40:545–549; discussion 549.
115. McMillan AM, Landorf KB, Gilheany MF, Bird AR, Morrow AD, Menz HB. Ultrasound guided corticosteroid injection for plantar fasciitis: Randomised controlled trial. BMJ. 2012;344: e3260.
116. Schulhofer SD. Short-term benefits of ultrasound-guided corticosteroid injection in plantar fasciitis. Clin J Sport Med. 2013;23:83–84.
117. Kim E, Lee JH. Autologous platelet-rich plasma versus dextrose prolotherapy for the treatment of chronic recalcitrant plantar fasciitis. PM R. 2014;6(2):152–158.
118. Peerbooms JC, van Laar W, Faber F, Schuller HM, van der Hoeven H, Gosens T. Use of platelet rich plasma to treat plantar fasciitis: Design of a multi centre randomized controlled trial. BMC Musculoskelet Disord. 2010;11:69.
119. Buchbinder R, Ptasznik R, Gordon J, Buchanan J, Prabaharan V, Forbes A. Ultrasound-guided extracorporeal shock wave therapy for plantar fasciitis: A randomized controlled trial. JAMA. 2002;288:1364–1372.
120. Kudo P, Dainty K, Clarfield M, Coughlin L, Lavoie P, Lebrun C. Randomized, placebo-controlled, double-blind clinical trial evaluating the treatment of plantar fasciitis with an extracoporeal shockwave therapy (ESWT) device: A North American confirmatory study. J Orthop Res. 2006;24:115–123.
121. Dizon JN, Gonzalez-Suarez C, Zamora MT, Gambito ED. Effectiveness of extracorporeal shock wave therapy in chronic plantar fasciitis: A meta-analysis. Am J Phys Med Rehabil. 2013;92:606–620.
122. Speed C. A systematic review of shockwave therapies in soft tissue conditions: Focusing on the evidence. Br J Sports Med. 2014;48(21):1538–1542.