When I first read this manual I didn’t believe it. Of course, it all sounded very sensible, but I just didn’t think I could do it. In fact, my first thought was that it was all going to be much too difficult for me and that it would be best if I didn’t even start, as I would only be disappointed and become demoralized. Luckily, I discussed this with my friend. She read the manual and pointed out that I wasn’t supposed to try to do everything all at once – the whole point was to proceed in small steps, building on the progress made – so it was worth making a start and seeing how I got on. I am so grateful to her for encouraging me to have a go. I am not saying it was easy. Far from it! It has been very difficult. But, it has changed my life for ever. And it was all about making small steps, practising them, and then doing a bit more. Like building a tower of bricks on the strong bricks below. The other day I threw the manual away. It was such a wonderful feeling because I know I don’t need it any more.
Many people who have problems controlling their eating manage to overcome their difficulties without seeking professional help. Some will have run into difficulties relatively recently and their disturbed eating will not therefore have become a habit. Others will have had problems for many years but never seriously got around to trying to do something about putting things right. For some the process of restoring their eating habits to normal is a relatively simple matter of starting to eat sensibly again. For many others the task is a very difficult one, yet somehow they do succeed. They manage to stop binge-eating. They stop making themselves sick. They stop taking laxatives. They eat ordinary meals at regular times. And, most important of all, food and eating cease to dominate their lives and they stop being so intensely concerned about their weight and their shape. In other words, they start to lead ‘normal’ lives again.
Sadly, many other people with very similar problems turn up in specialist clinics having been unable, after repeated efforts, to manage on their own. It is not necessarily that their problems have been around longer or that their eating habits are more severely disturbed. It is just that the things they tried to do to improve matters simply did not work. And often they made things considerably worse. Now, of course, many people with bulimia nervosa will need specialist help and it is important that they seek such help and receive it. But many others could, if they knew how to go about it, manage to restore their eating habits to normal without professional help. This self-help manual is intended to provide guidelines for people who want to try to manage on their own but are unsure where to begin.
The guidelines that follow are aimed at people who have what might be termed ‘classic bulimia nervosa’: that is to say, people who regularly lose control of their eating and binge, attempt to compensate for the episodes of overeating in extreme ways (e.g., by fasting, vomiting or taking laxatives), and who regard their body shape or weight as of great personal significance, to the extent that concerns about weight and shape dominate their lives.
Of course, there are many other people who do not quite fit this description but who share some of the same features. They may binge very occasionally. They may not binge but regularly make themselves sick after meals or after eating any food they believe to be potentially fattening. They may alternate between periods of relatively normal eating and days of strict fasting to lose weight. They may regularly take laxatives to compensate for eating what they regard as fattening food. The guidelines that follow are also likely to be of use to these people. Although some of what is discussed may not be relevant to them, the general principles apply to all people who are experiencing difficulty controlling their eating and want to restore their disturbed eating habits to normal and to put their concerns about their weight and shape into a manageable perspective.
There are six categories of people with bulimia nervosa for whom this manual is probably not appropriate.
1 For some people who are rigidly locked into a pattern of grossly disturbed eating habits, the idea of their being able to break out of the cycle on their own may not be realistic, and they may well need to consult a CBT therapist. It is important to add here that many people who do not belong to this category will think that they do. If you are prepared to try to change some aspects of your current eating habits, then it is certainly worth your while making an effort at using this manual.
2 Some people who are completely socially isolated may well need the support and encouragement of a therapist they can see regularly.
3 Some people who are so demoralized and disheartened that they cannot muster the energy to begin to try to change may well need to consult their GP about getting help with their mood before starting to use this manual.
4 For some people whose body weight is very low (and, in addition to bulimia nervosa, are suffering from anorexia nervosa), it is possible that the guidelines contained in this manual could actually do them harm rather than improve matters, and they should consult their GP.
5 For some people the eating disorder is only one relatively minor feature of much wider difficulties, such as problems with alcohol, self-harm (such as cutting themselves or repeatedly taking overdoses) and their relationships; they will need more help than that provided in this manual.
6 People with a medical condition in which eating can have a significant impact (such as diabetes), and women who are pregnant, need to place themselves in medical care.
If you belong to one or more of these six categories you will need specialist help and you should consult your doctor about being referred for treatment. For all of these groups specific treatments are available, and the prospects of being helped are good if such treatment is received.
In fact, this manual is likely to be of help to the great majority of those with bulimia nervosa and related problems. This statement can be made with confidence because the effectiveness of the manual has been studied. Some years ago we studied more than eighty people with bulimia nervosa who were referred by their doctor to whom we gave the manual. They used it for four to six months and were then re-evaluated. The great majority of them had improved substantially and regarded themselves as no longer in need of help. Some of these people have written accounts of their use of the manual, four of which have been included at the end of this book (Appendix 4). These preliminary findings have recently been confirmed by independent research (see pages 74–7).
Overcoming difficulties with eating is seldom easy and is usually very hard indeed. It is therefore essential, if you are to make a serious effort at recovery, to make this task a very high priority in your life. Restoring your eating habits to normal must be your first priority; and other responsibilities will have to fall in line behind this priority. This may sound like awful advice. You may well feel that it is totally against your principles to act so ‘selfishly’. But it is really the responsible thing to do because it is only by overcoming your eating problems that you can properly take on your wider personal and social commitments. So, if you feel reluctant to give your own problems such a high priority at the expense of the needs of others, you can reassure yourself that it would really be in everyone else’s best interests if you did so.
While it is true that it is difficult to overcome bulimia nervosa, doing so is immensely worthwhile. To most people this conclusion is so obvious that it is hardly worth stating. But some people might need a certain amount of convincing. There are three main reasons why restoring eating habits to normal is worth the effort involved.
Psychological reasons There are a number of psycho logical consequences of bulimia nervosa and related disturbances in eating habits which make overcoming these problems worthwhile. Considerable shame and guilt frequently surround binge-eating and vomiting. This leads people to live a secret and lonely existence, sometimes for many years, and makes them feel inferior to others – even, at times, quite worthless. Also, severe depression commonly sets in after a binge, and this can last for some time. Some people undergo wild mood swings, usually in response to their degree of control over their eating, such that they change rapidly from feeling extremely happy to feeling utterly miserable. Often people feel very anxious in situations involving exposure to food, such as eating out, eating in front of others, or preparing food for other people. The constant preoccupation with weight, shape, food and eating often makes concentrating difficult. Indeed, it is common for people to feel that their lives are totally dominated by thoughts about food and eating and concerns about weight and shape. Reinstating ‘normal’ eating habits reverses many of these difficulties and is a major step towards resolving the others.
Social reasons Bulimia nervosa takes a great toll in terms of one’s social life. Personal relationships are badly affected. At worst, binge-eating and vomiting occur many times a day and there is simply no time to lead anything approximating a normal life. The truth is that much of social life involves eating with other people. Many people with bulimia nervosa solve this particular problem by always eating on their own. Also, it is common for people to feel fat and unattractive after a binge and not to want to be seen by anyone. So they avoid company and again choose to remain on their own. Unfortunately, under these circumstances they are much more likely to binge. Family relationships frequently become strained.
In addition, for a number of reasons work can be adversely affected. Food-related situations are particularly problematic. For example, there can be major difficulties in dealing with the cafeteria or coffee breaks. Also, as noted above, thoughts of food and eating and concerns about weight and shape can interfere with the ability to concentrate to such an extent that performance at work can suffer. People find it difficult to keep track of what they are doing; and they find it impossible to focus on a particular task, ending up, for example, reading something over and over again, quite unable to take anything in.
Even if one is apparently coping quite well, the feelings of depression and worthlessness which the binge-eating and vomiting cause can make one feel generally inadequate and unconfident at work and socially. Again, all these difficulties improve considerably when one’s eating habits return to normal.
Medical reasons There are a number of potential medical complications associated with bulimia nervosa and binge-eating. Some of these arise as a result of the binge-eating and others as a result of the methods to which people resort to compensate for overeating (vomiting, taking laxatives and so on). Some of these complications are common, such as abdominal pain, salivary gland swelling and sore throats. Rarely, there can be more serious complications, such as damage to the stomach wall or the oesophagus. Repeated vomiting and frequent laxative-taking can disturb the body’s fluid balance and lead to hypokalemia (low potassium), which can cause irregularities in heartbeat.
All of these potential physical hazards add force to the argument that it is worth making an effort to recover. It is important to emphasize that the majority of these physical complications are reversible. That is, when normal eating habits are re-established, the body readjusts and returns to a healthy state.
The disturbed eating habits of people who binge can complicate the course of pregnancy. If you are pregnant and binge-eating, or dieting, or vomiting, or taking laxatives, diuretics or other pills, you should discuss these matters frankly with your doctor.
These are some of the reasons why it is worthwhile committing yourself to overcoming your eating difficulties. No doubt there are other, perhaps more compelling, personal reasons for doing so. Whatever your particular reasons for wishing to change, it is important to emphasize at the outset that you will not be able to stop binge-eating and resume ‘normal’ eating unless you are very highly motivated to do so. By the same token, if you really want to change and are prepared to make a major commitment to doing so, there is every reason to expect that you will be successful.
It is worth considering, before going any further with this manual, whether now is the right time for you to be tackling this problem. If you are about to go on holiday in two weeks, or you are studying for exams, you will not be able to devote yourself properly to the principles outlined below. In such circumstances, it would be best if you postponed beginning the program until the time is right and you can make the necessary commitment. If you make a half-hearted start and then run into difficulties you may well become disheartened and give up on something that might work for you under the right circumstances. On the other hand, unless there is a serious reason for not starting with this program now, like the two examples given above, you should commit yourself to beginning at a definite time in the near future. There will always be sufficient trivial reasons for postponing beginning this program and you should be suspicious of weak excuses.
Before setting out the program you should follow in tackling your difficulties with eating, it is worth describing the kinds of factors operating to prevent people with bulimia nervosa from just getting better spontaneously. It may seem odd that bulimia nervosa continues when the behavior in which people engage is so contrary to how they want to behave and when it makes them so miserable. The reason for this is that people unwittingly adopt methods of coping which are counter-productive. For example, fasting after a binge may make you feel better temporarily, but it also significantly increases the chances that you will binge again. The three main factors which serve to perpetuate bulimia nervosa are shown in Figure 1.
Most young women at some time go on a diet to lose weight. However, it is a sad fact that, despite the effort and commitment and the money invested in diet literature and diet regimes, these attempts are rarely successful. Moreover, there is good evidence that dieting places people under physiological and psychological pressures to eat and, paradoxically, causes overeating. For the great majority of people with bulimia nervosa, binge-eating began after they had started dieting. And for all of them, it is dieting that keeps the binge-eating going. In order to overcome bulimia nervosa and be confident of being able to eat ‘normally’ you are going to have to give up the idea of dieting. Of course, this is a terrible prospect for someone who has dieted for years and who is terrified that to stop doing so would inevitably lead to her becoming fat. But, for anyone reading this guide in the hope that it might contain information which will help you deal with your eating problems, it is a simple truth that dieting has not worked: you are almost certainly heavier than you want to be and, despite wanting to lose weight, you periodically lose control and binge, which is guaranteed to prevent you from losing weight. It is also the case that for most people their current weight is, in fact, more than the weight they were when they started dieting. Indeed, an interesting question for anyone who is binge-eating and dieting to ask themselves is whether the average number of calories they absorb in a typical week is really less than it would be if they were not binge-eating and dieting but were, instead, eating ordinary regular meals. It is very difficult for anyone whose eating habits have become seriously disorganized and disturbed to answer this question. However, the truth is that, whatever efforts one goes to in order to compensate for overeating, a large number of calories is absorbed from a binge; and, in fact, it is usually the case that people who replace a pattern of dieting and binge-eating with regular meals do not gain weight. Some people actually lose weight. It is very rare that normal eating leads to significant weight gain.
Figure 1 The three main factors that perpetuate binge-eating.
Having read the previous section, you may well be thinking: ‘Well, if I am not allowed to diet, this program is not for me.’ This is an understandable response; but it must be repeated in the strongest terms that dieting has not worked for you and it is a major factor causing you to binge. You may well reply that, while it is true that dieting has failed in the sense that your eating habits are disorganized and out of control, it is, nevertheless, the case that if you were not dieting you would be even worse off since you would be eating far too much and would be gaining weight and in no time would be fat. This is a very strong conviction and a very compelling fear for many people with bulimia nervosa. However, it is a conviction which is almost certainly wrong and a fear which is almost certainly unfounded. It is worth repeating that for most people the replacement of a pattern of dieting and binge-eating with ‘normal’ meals does not have a significant effect on their weight. It will be very difficult for anyone who has these convictions and fears to accept this rebuttal on faith. The only way forward is to try the following experiment: for a four-week trial period commit yourself to sticking to all the principles spelled out in this manual and, after the four weeks, assess whether there has been an improvement in your eating habits and see what has happened to your weight. The answers to these questions will help you decide whether it is worth continuing with the program.
Vomiting encourages overeating. It is very common for people to say that when they first discovered vomiting as a method of dealing with overeating they felt elated. Suddenly they could eat what they wanted without it affecting their weight. However, they soon discovered that, far from liberating them, vomiting is a trap: vomiting leads to more eating which in turn leads to more vomiting. And a vicious cycle is established where vomiting comes, in part, to encourage binge-eating. Indeed, many people with bulimia nervosa find that, if they know that the circumstances are such that they are not going to be able to vomit (for example, if they are going on a long car journey with friends), this acts as a temporary brake on their eating. The implication for someone who wants to restore their eating habits to normal is that by stopping vomiting they will be encouraged to exert more control over their eating. It is, of course, not as simple as this and giving up vomiting as a method of escaping the consequences of overeating is far from easy. To some extent the same argument applies to the use of laxatives (see the section below headed ‘Some advice’).
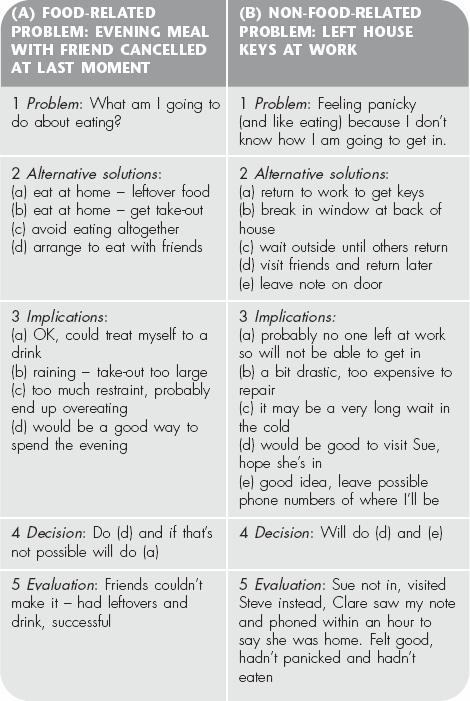
Depression often causes people with bulimia nervosa to binge. And binges make people depressed. Thus, another vicious cycle is set up. Now, if you are making an effort not to binge, you will be attempting to break out of this cycle. However, many things other than overeating can make you feel depressed and thereby indirectly lead you to binge. The implication here is that it is important for you to examine which aspects of your life are unsatisfactory and cause you to feel depressed, and to attempt to find solutions to these difficulties (see the advice about problem solving in Step 4 below).
There are a number of other factors which serve to perpetuate binge-eating. One important factor is a very low body weight. This is not usually a problem in bulimia nervosa because most people with the disorder are within the ‘normal’ weight range. But for some people whose body weight is very low, the body is, in effect, in a state of starvation and this, in itself, seems to cause binge-eating. For people in this situation binge-eating cannot be overcome completely unless they allow their body weight to rise to a healthy level (see below under ‘Some advice’).
There are other factors, too, which can make it more likely that a binge will take place (such as drinking alcohol), and it is important that these are identified and steps taken to eliminate their effect (see Step 3, ‘Learning to intervene’).
The guidelines spelled out below are essentially practical. They arise from an acceptance of the problems with eating at face value: that is, that there are people who are distressed by being unable to control their eating and who need help in restoring their eating habits to normal. The manual is intended to provide these people with the tools they need to recover. The guidelines are not, therefore, intended to help you uncover any deep reasons which might have caused your eating to become disordered in the first place. The reason for this is simply that the process of uncovering hidden causes is not necessary for restoring eating habits to ‘normal’. That is to say, it is perfectly possible for someone with bulimia nervosa to overcome her problems with eating simply by focusing on changing her eating habits and her attitudes towards weight and shape. Given that this is possible, it seems sensible to specify how someone might achieve this end on her own.
Of course, some people may feel that the problems they have, including their eating disorder, arise directly from aspects of their early experience of which they want a deeper understanding, and they may well feel that a course of psychotherapy would be helpful to them in this regard. Similarly, some people may feel that a course of counselling would help them to deal with the day-to-day stresses of their lives. Following the guidelines set out in this manual is not at odds with either of these options. Psychotherapy and counselling do not stand in opposition to your dealing with your eating problems yourself; and you may feel that they would actually help you manage better with the manual. However, it must be emphasized that while they may or may not be helpful to you, it is usually perfectly reasonable to expect that you will be able to restore order to your eating habits without such additional help.
Finally, it is important to consider the recent research on CBT for eating disorders which has indicated that a more complex form of treatment than that outlined in this book may be helpful for certain people. These people are those who have an eating disorder and at least two of the following four factors (present in at least moderate clinical severity):
1 Low self-esteem
2 Interpersonal difficulties
3 Perfectionism and
4 Mood intolerance (i.e. inappropriate ways of dealing with anger, anxiety or depression, such as self-injury, taking alcohol or certain drugs, or bingeing).
The research findings suggest that such people need a form of CBT that focuses not only on their eating disorder, but also on these wider problems. It is not that the eating-focused CBT, of the sort specified in this manual, does not help such people; it is just that it does not help them as much as a CBT approach which also deals with their wider problems. It is important that you give some thought to this issue when you consider how to proceed with this manual. For example, if you feel that you do have a serious problem with low self-esteem or with interpersonal difficulties, there are other books in this series which you should consider consulting (for example, Overcoming Low Self-Esteem by Melanie Fennell and Overcoming Relationship Problems by Michael Crowe). If you feel that you are a perfectionist and that this is creating significant difficulties for you, a manual for overcoming perfectionism is available in this series (Overcoming Perfectionism by Roz Shafran, Tracey Wade and Sarah Egan), and it is likely to be of help to you.
Finally, if mood intolerance is a significant problem for you then finding ways of dealing with this issue is likely to be an important part of your recovery. It is an issue that is touched on in several places in this manual, but it may be an area where you find you need further help. If, having completed the course of self-treatment specified in this manual, you feel this is an area where you do need to make more progress, then do consult your GP and ask to be referred to your local clinical psychology or CBT service.
This self-help program is not intended to be a comprehensive record of everything one could imagine doing that might be helpful in restoring eating habits to normal. It would be a formidable task to produce such a record because it would need to include so many variations applicable to such a wide range of people. It would also be confusing to find one’s way around and probably would not be very helpful to many people. Instead, the manual provided here consists of the core elements of a self-help program. Much of the specific detail will need to be filled in by you and will depend on your particular circumstances and what sort of person you are. The manual is intended to be what might be termed a basic treatment: that is, it consists of the minimum requirements necessary for restoring eating habits to ‘normal’. This minimal treatment is set out on the assumption that it will be sufficiently helpful to many people with bulimia nervosa to enable them to deal with their eating problems without specialist help. It is, however, important to state again that for some people it may not be sufficient and it is important that they consult their doctor about finding additional help.
The treatment program described below is highly structured. It assumes that you want to overcome your eating difficulties and that you want advice on how to go about doing so. This advice is given. It is, of course, entirely up to you which pieces of advice you choose to accept and which you do not. However, all the components of the program are known to be helpful to patients with bulimia nervosa receiving treatment in specialist clinics, and the more of the advice you choose not to follow the less likely it is that the program will be helpful to you in restoring control to your eating. Conversely, the extent to which this manual is going to be useful to you depends on how strictly you can adhere to its guidelines. In some sense, if this manual is going to help you, it is necessary for you to trust it all more or less as an act of faith. However, given that you have read this far and it is therefore likely that you do not know how to proceed with helping yourself, it is an act of faith probably worth making, at least on a trial basis.
The self-help program spelled out below places considerable demands on you. As you read on you may well feel overwhelmed by how much you are going to have to do to overcome your problems with eating. Do not be too daunted. First, the program builds up slowly, in steps, and you can set the pace. Second, although the program specifies definite steps you must take in order to recover, it is not intended that you should follow these steps for ever. Indeed, the goal of this treatment is that you should be able to reach a position where food is no longer a threat to you, where you can eat normally, with enjoyment, and without anxieties about your weight and shape. To arrive at such a goal, however, it is necessary to proceed via a route that does involve thinking a great deal about food and eating and about your weight and shape. In other words, in order to free yourself of your anxieties, for a period of time it will be necessary for you to pay particular attention to your eating and your concerns about weight and shape. How long it will take to recover varies greatly from individual to individual. Most people with bulimia nervosa who can make use of this manual work through it in about six months. Some manage to do so in a shorter period and some need longer. It would be a mistake to concern yourself at this stage with how long it will take you. However, if you find that you have made a real effort to use the manual and have not been able to make any progress at all in, say, around six weeks, then it would be sensible to stop trying to use it alone and consult your doctor about getting further help. If, on the other hand, you have made even just a little progress, over some months, then as long as you continue to progress it is worth persevering.
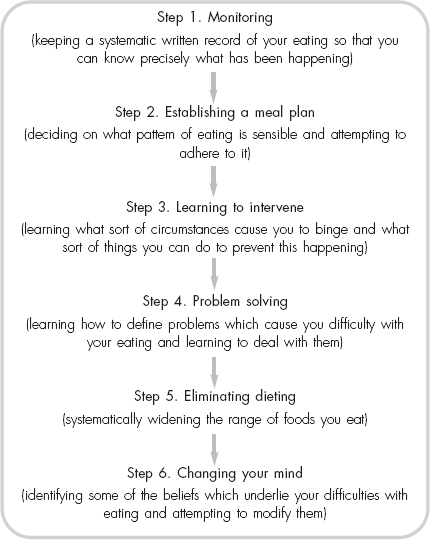
There are six steps to the self-help program. These are listed in Figure 2 (page 101), and these six steps follow each other in the order given: having established regular monitoring of your eating (Step 1), you move on to setting up a meal plan (Step 2) while continuing with the monitoring; and, having set up a meal plan, you move on to learning to intervene in times of difficulty (Step 3), in the context of your meal plan (while continuing to monitor your eating); and so on. At the end of each step there is a ‘Review Box’. This consists of a set of questions which you should ask yourself, concerning the progress you have made. Only when you are able to answer ‘yes’ to all the questions should you proceed to the next step in the manual.
This manual contains a lot of information. If you read right through it, put it aside, and then attempt to follow all the advice at once, you will not succeed. It is essential that you follow the steps in the order they come and only go on to the next step when you are ready to do so. It is a good idea to read through the entire manual first to get an overall idea of the sort of information it contains. For some people who have serious difficulties in concentrating, the prospect of reading through the entire manual will be too daunting. What they should do is spend just ten minutes skimming through the manual, perhaps just reading the headings and subheadings; this will be sufficient for them to get a rough idea of what the manual contains. Having read through the manual (or skimmed through it), you will be ready to begin Step 1. However, you will not be able to remember in sufficient detail from one reading what is contained in Step 1, so you will have to re-read it. In fact, you will need to refer to the manual again and again and it would therefore be sensible for you to carry it around with you. It might help you to mark the sections that are especially relevant to where you are in the program. In addition, if you attempt to follow some particular piece of advice given in the manual and it does not work out as planned, you should go back to the relevant section, re-read it, and try to determine why things went wrong and what you should do next time to improve your chances of succeeding.
Figure 2 An outline of the self-help program presented in this manual
Some people whose eating is not very seriously disturbed will be able to make use of this manual entirely on their own. However, for many people with bulimia nervosa this is an unrealistic expectation. The problem is that, however hard you try to stick to the guidelines set out in the treatment program, there will inevitably be times when things do not go well. At these times it is difficult not to become depressed, to blame yourself and to feel like giving up. Having someone to talk to, at these times, to go over what has happened and what you might be able to do about it, can be invaluable. Such a person could be a close friend or relative. However, it is usually better for such a helper to be someone with whom you do not have a close relationship in your ordinary life; someone who is less intimately involved with you and who can therefore be objective. Your doctor or the healthcare provider (in the UK your GP or the practice nurse) is probably a better person to choose than a friend. It is particularly good if you can see your helper regularly. Ideally this should be every week at first, but it soon can be less frequent than this.
At the end of this manual there is a brief section for helpers (Appendix 3). You should show this to the person you ask to help you.
It is common for people, having read right through the manual, to feel charged up with enthusiasm to tackle their difficulties with eating. It is also common for people to feel, the first time that something goes wrong, that they have totally failed and will never succeed. It is important to stress that if overcoming your problems with eating were easy, you would have done so long ago. It is going to be a struggle and there will be times when you will not manage to achieve as much as you want to. However, if you are attempting to follow the guidelines set out in this manual, you are making an effort at taking control of your eating; and any success at all is an improvement on which further improvements can be built. Do not imagine that you can follow all the manual’s principles tomorrow and that you will therefore never binge again. Replacing disorganized eating habits with a ‘normal’ pattern of eating is usually a slow and painful process in which there are a great many attempts which do not work out as one might wish. However, if you do try to follow the principles set out here and make rational decisions about how to proceed, you will almost certainly make progress. And if you are making progress, however slowly, it is worth persevering. Many people find that at some point, perhaps some months after starting out, suddenly things become much easier and the prospect of a life of ‘normal’ eating becomes a possibility they can genuinely imagine. So if you are just creeping forward, it is well worth carrying on and waiting for the breakthrough.
Before describing the six steps in the self-help program, it is important that you are armed with certain information which will be of help to you. In particular, it would be useful to reconsider what is an appropriate weight for you; it would be helpful to establish a regular system of weighing yourself; and it is worth considering how effective vomiting and purgative use actually are at getting rid of unwanted calories.
It is very difficult for anyone to pronounce on what is the ‘correct’ weight for you. Some people argue that your weight should not be allowed to fall more than 15 per cent below the average for your age, height and sex. The basis for this argument is that below such a weight the physiological and psychological effects of starvation will make it virtually impossible for you to eat normally. Others argue that the ‘correct’ weight is the weight you were before your problems with eating began. Both of these definitions can be helpful in many cases, but neither is entirely satisfactory. Some people whose relatives are all overweight, and whose natural weight is higher than the average, would experience starvation symptoms well before they weighed 15 per cent less than the average. And for many people with bulimia nervosa who have a long history of disturbed eating habits of one sort or another, it is impossible to identify a point at which their eating was sufficiently ‘normal’ to identify a natural body weight.
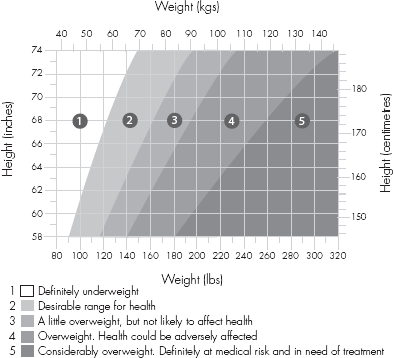
The range of body weights is shown in Figure 3. You might find it helpful to consider what would be a healthy weight for a person of your height. It may also be worth your considering where the weight you would ideally like to be is in relation to the norms shown in the figure. Many people with bulimia nervosa want to be at a very low weight, and if they are going to recover from their eating disorder and manage to eat normally they are going to have to give up this desire to weigh so little and replace it with a more realistic target weight range.
Natural weight – the weight at which your body would settle if you were eating perfectly normally – varies considerably from one individual to another. This weight is determined by two things: first, genetic factors (i.e. factors which you have inherited from your parents), which have a strong influence on your natural weight; and second, the balance between how much you eat and the energy you expend. Now, it is most unlikely that you will have an accurate idea of what this weight would be if you were eating normally; and it is very likely that, if you were to make a guess, you would substantially overestimate the true figure. The truth is that the only way to discover what your natural weight is, is to reinstate normal eating habits and then see over a period of several months what happens to your weight. It is also important to remember that weight does not ordinarily sit at one fixed point. Rather, it is quite ‘normal’ for body weight to fluctuate within the space of a week by a few pounds in both directions. So if you do have in your mind an acceptable weight this should be a range of acceptability (with a two- or three-pound margin in either direction) rather than one fixed number. You must also remember that weight changes occur naturally over the menstrual cycle. Premenstrual water retention, bloatedness and ‘weight gain’ are very common and a result of normal hormonal changes.
Figure 3 Range of weights
Source: Adapted fromObesity and Related Diseases by John Garrow (1988), by kind permission of Churchill Livingstone.
As noted above, it is usual for the weight of people who follow the principles set out in this self-help guide not to change significantly. Some people do lose weight. However, most people never achieve the weight they would ideally like to be. This is because their ideal weight is usually unrealistically low and simply not achievable without starving themselves to a point where they would be at serious medical or psychological risk. It has to be added here that the vast majority of women with no particular eating problem also want to weigh much less than they do; and they also almost always fail to achieve this low weight. However, the important point here for people with bulimia nervosa is that there is often a trade-off to be made between weight and eating habits: thus, you may well find that, having stuck to this self-help program, you will be able to eat normally, but that your weight is, say, a few pounds more than you would like it to be. But, if you diet and lose those few pounds, then you will not be able to maintain control of your eating and binge-eating will return. Ultimately the choice here will be entirely yours. The question is: ‘Is weighing a few pounds more than you are entirely happy with a worthwhile price to pay for normal eating habits and the kind of life that this permits?’ Or, to put it the other way round: ‘Is weighing a few pounds less a worthwhile goal given that the cost is perpetually disturbed eating habits and the effect they have on the rest of your life?’
If you follow this treatment program it is likely that you will eventually be faced with the questions posed above. It is not worth considering your answer in any detail at this point because you do not know the exact nature of the choice; and you won’t know it until you are eating normally and your weight has settled. Some people are very lucky and their weight settles at exactly the point they always wished it to be. Others are less fortunate. For the great majority the outcome is the same as it is for everybody else: their weight is a little above what they would prefer it to be. The sensible thing to do at this stage, when you are just beginning to try to restore some order to your eating habits, is to postpone any decision about your weight and about what weight would be acceptable to you until you have regained control of your eating and seen precisely what effect this has actually had on your weight.
There are two common ways in which people with bulimia nervosa deal with weighing themselves. Some get on and off the scales frequently, to check what effect binge-eating, vomiting and so on has had on their weight. Many others avoid weighing themselves altogether because the effect of doing so is too distressing. Many alternate between the two extremes, depending on the degree of control over their eating and whether their weight is high or low. Neither solution is satisfactory. Frequent weighing merely serves to increase the level of concern and preoccupation with weight by highlighting small and insignificant fluctuations; and completely avoiding weighing also increases anxiety about what the weight might really be. Certainly, establishing a meal plan and attempting to follow it, as you will do if you follow the manual, does have direct implications for your weight, and if you are to make rational decisions about your behavior you ought to be aware of exactly what these implications are. The appropriate solution is to weigh yourself once a week. This should be at the same time each week (Friday morning is a good time for many people) and, given that on some occasions this may be an upsetting experience for you (and when you are upset you are likely to feel like eating), it is wise to choose a time of the day when it is going to be difficult for you to eat (such as just before you have to leave the house for work). You should record your weight so you can track its progress. Weighing should be obligatory. You should not weigh yourself at any time other than your set weekly time.
For some people this is going to be a very difficult task. If you have avoided weighing yourself for some time you will find it difficult to begin. Unfortunately there is no easy way to start: you will simply have to steel yourself. But you can be reassured that once you have started it can become a relatively simple routine. On the other hand, if you are weighing yourself frequently, say, many times a day, it will be very difficult to restrict weighing to once a week. In such circumstances you should put yourself on a program to cut down the frequency of weighing. For example, for the first week you should restrict weighing to once a day. For the second week you should weigh every second day. And so on. By the end of four weeks you should be on the once a week weighing schedule.
It is common for people with bulimia nervosa to make frequent checks on their body shape, just as they might make frequent checks on their weight. So they might use a tape measure to judge the ‘fatness’ of particular parts of their body, such as their thighs or their waist. They might make regular inspections of themselves in the mirror. And they might pinch certain parts of themselves (like their stomach) to gauge how ‘fat’ they are. Checking your body shape in this way is not a good idea and you should try to stop doing it. Making these sorts of checks simply serves to increase your concerns about your shape. You feel happy when the check produces a desirable result and distressed when the results are unsatisfactory. And the problem is that these responses then come to govern your subsequent actions. Thus, it is common for people who have examined themselves in the mirror and decided that they are fat to immediately go and binge. It is important, therefore, that you stop making such checks of your body shape. If necessary, you can phase out these checks gradually, as described above for people who weigh themselves very often. However, the sooner they are stopped the better.
Some people judge their body shape by how tight their clothes feel. This too serves to maintain the preoccupation with shape and size. It is, incidentally, quite an unreliable method because some clothes shrink when they are washed; and the result is that one feels fatter when one is wearing clean clothes! If you habitually judge your shape by the feel of your clothes, then it would be well worth your while taking all your clothes which are tight (jeans and skirts are especially important) and either altering them so that they fit more loosely or getting rid of them. Some people keep in the wardrobe clothes they used to wear some time ago when they were much thinner. Their intention is to start wearing them again when they have successfully reduced their weight. This is a most unhelpful practice. It encourages dieting which, in turn, encourages binge-eating. And the small clothes are a depressing reminder that you are not as thin as you would like to be. It would be best if you got rid of these clothes.
Clearly an important aspect of restoring your eating habits to normal is for you to stop vomiting. For most people this will follow naturally once they have established a pattern of regular eating and have stopped the binges. Some people, however, will need to make a special effort. It is important to remember that vomiting encourages overeating. So, in a sense, the more you vomit the more you will overeat. A basic principle you should try to follow is that you should always try not to eat anything that you know you will feel unable to keep down (see Step 2, ‘Instituting a meal plan’).
A fact that comes as something of a surprise to most people with bulimia nervosa is that vomiting does not really work. Its purpose is to get rid of the food eaten, usually in a binge, so that the calories ingested will not be absorbed. The reason this purpose is not achieved by vomiting is that binges usually involve the consumption of a large number of calories and vomiting does not retrieve all of them. In fact, a significant proportion of the calories consumed in a binge will be absorbed by the stomach and small intestine. What this means is that usually the number of calories absorbed from binges, even after vomiting, is greater than the number that would have been absorbed in a binge-free day during which normal meals and snacks had been eaten.
Some people who find it difficult to make themselves sick take laxatives as an alternative method of compensating for binge-eating. Others who do vomit after binges take laxatives as a further ‘guarantee’ that calories are not absorbed. Laxatives are wholly ineffective as a method of losing weight or compensating for overeating. They have a minimal effect on the absorption of calories, and the small influence they do have on body weight is achieved by changing the body’s fluid balance (essentially, through water lost in diarrhoea). This is a temporary effect because one inevitably gets thirsty and drinks, and the restoration of the lost fluids reverses the apparent weight loss. Even if you have felt that some physical cost to taking purgatives would be worth it for the benefit to your weight, given that there is no such benefit there really is no point at all in continuing taking laxatives.
There are many problems associated with the use of laxatives. One is that the body develops tolerance to them, and people find that in order to experience the laxative effect, they have to increase the dose steadily. One consequence of this is that when they try to stop taking the laxatives, or try to cut down the number they take, they become constipated. Another problem is that the body retains water in an attempt to compensate for the laxative effect, leading to puffiness and swelling. If you are taking only small amounts of laxatives occasionally there should be no difficulty in your stopping this immediately. If you take them regularly it may be helpful for you to phase them out gradually. Certainly, if you take a large quantity, a phasing-out process is advisable to avoid the ‘withdrawal’ effects described above. You may also benefit from taking one of the commercially available fibre supplements (in the normal prescribed dose) to counteract any constipation. If you are regularly taking large quantities of laxatives and cannot manage to phase them out, even with the help of a fibre supplement, you should consult your doctor for help.
Some people say that even though they know that laxatives are no help to them in controlling their weight or in compensating for overeating, they serve another purpose which makes them want to continue taking them. One such purpose is to make them ‘feel empty’, which is a comfort, particularly after a binge. Another reason people give for taking laxatives is that their effect is exceedingly unpleasant and they are used as a form of self-punishment. Neither of these ‘purposes’ is helpful and they must be put aside. If you are working at a program for restoring your eating habits to normal you must do only what is good for you and what will help you, and you should reward yourself for doing well, not punish yourself for lapses.
Diuretics, which are pills designed to reduce the body’s water content by encouraging urination, have no real effect on body weight; as with laxative use, any appearance to the contrary is the result solely of temporary effects on fluid balance. They are of no benefit to you at all and you should not take them (unless, of course, they have been prescribed by a doctor for a medical reason).
Exercise is much encouraged these days because of its positive benefits to health; and many people with bulimia nervosa say that they definitely feel much better about themselves when they are taking regular exercise. However, it is also the case that many people use excessive exercise as a method of compensating for overeating. This is not healthy and serves to perpetuate concerns about food, eating, weight and shape. If you are using exercise primarily as a means of weight control, you should keep a record of exactly how much time you are spending exercising. This can then be reviewed and you can institute a program of appropriate exercise. You may well find this difficult and it may be necessary for you to reduce the amount you exercise in stages. The aim is for you to exercise because you enjoy it and because it is physically good for you. Any exercise which is taken principally for weight control reasons or to compensate for overeating is not advisable.
Drugs which suppress your appetite (like amphetamines) do have a temporary effect on eating. However, they also have a number of physical and psychological side-effects. They are also addictive. It is most inadvisable to take them to help you to avoid eating. They should never be taken unless under medical supervision. Most importantly, when people stop taking them their eating returns to just the same state as it was in before they took them.
Note: Read through all of Step 1 before beginning to try to implement the principles outlined in this section.
If you are going to begin trying to change your eating habits then it is important that you know exactly what is happening with your eating at the moment. For this reason it is essential that you keep a detailed record every day of when you eat, what you eat, where you eat, whether you felt that what you ate was excessive, whether you felt out of control, whether you vomited or took laxatives, and other circumstances that might be relevant to reorganizing your eating habits. At first keeping such a record might seem both tedious and pointless. It might even seem like a punishment, in that by making you more aware of your eating habits it makes you feel worse. However, for you to begin to change it is necessary that you do become aware of exactly what is happening with your eating; and it will soon become apparent that this record is an invaluable aid in this process.
In keeping this record, it will be helpful for you to stick to the following guidelines:
1 Use a standard form (see below for example).
2 Use a separate sheet (or sheets if necessary) for each day.
3 Record everything you eat (not just things you feel happy about having eaten), and do not abandon monitoring when your eating goes wrong.
4 Write down what you have eaten immediately after having done so, rather than trying to remember everything at the end of the day.
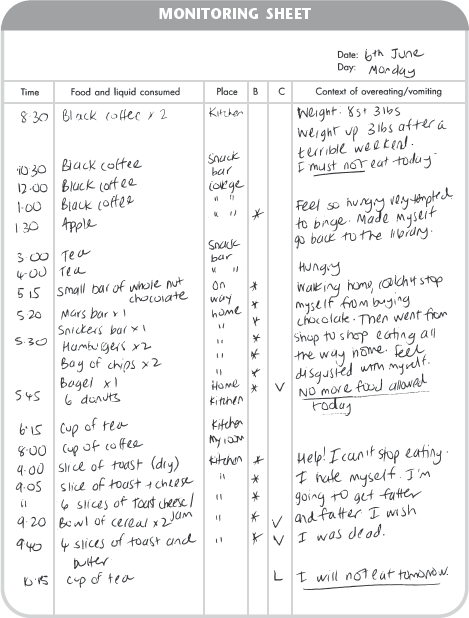
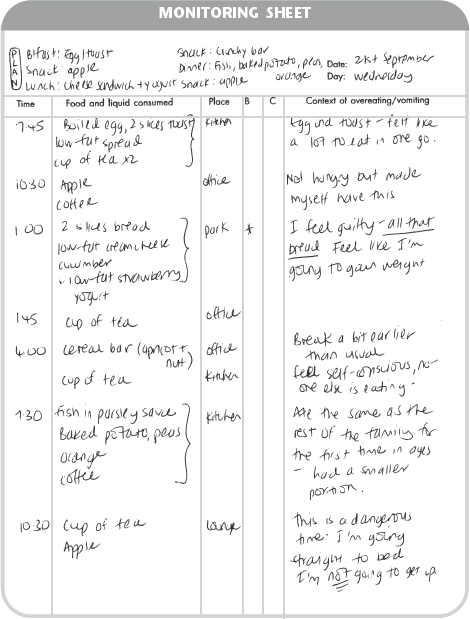
An example of one person’s monitoring sheet for one day is shown in Figure 4.
1 The first column is for recording the time when food is eaten. Try to be reasonably accurate about this because, as will emerge later, it is important.
2 The second column is for recording all the food (and liquid) that you consume during the day. As already noted, it is important to write this down soon after the episode of eating. To do this it is obviously necessary that you carry the monitoring sheet or notebook with you at all times. When writing down the food you should be reasonably precise about what you have eaten. So if you eat two chocolate bars, rather than just writing down ‘chocolate’, you should record it as, say, ‘two Mars bars’. However, you should not be so precise as to weigh food and record the weights (like ‘100 grams All Bran’, when ‘a small bowl of All Bran’ would do); and you should not record the calorie content. A simple description of what you ate is perfectly adequate. Since the aim of your following this self-help program is to restore healthy eating habits, it is important that you indicate on your monitoring sheets when you ate a normal meal. It may be difficult for you to decide on what is and what is not a ‘normal meal’. What is meant is an episode of eating where food is eaten in a controlled and organized manner. The amount eaten should not influence your decision here. As long as you intended to eat certain food, and did so in a normal fashion without feeling out of control, then this can be regarded as a meal. These episodes should be distinguished from all other eating by marking them with a bracket (see Figure 5, page 132).
Figure 4 Example of a monitoring sheet
3 The third column is for recording where the episode of eating took place. Again, you should be fairly precise about this: it is better to say ‘the kitchen’ than just ‘home’.
4 The fourth column, headed B, is for recording whether or not you felt the food eaten was excessive. This should be done by placing an asterisk in this column next to any item of food which you felt at the time was excessive and which you wish you had not eaten. You may regard food as excessive for one of two reasons: first, because of the quantity eaten (e.g. three potatoes when you felt you should have had only one); second, because of the type of food eaten (e.g. a chocolate bar, when you feel you ought never to eat chocolate). It is important that all food eaten in a binge is recorded on the monitoring sheet and, in such cases, each item will be asterisked.
5 The fifth column (headed C for compensation) is for recording episodes of vomiting and taking laxatives or diuretics. If you exercise as a method of compensating for having overeaten then this too should be recorded here.
6 The sixth and final column is for recording how you feel at the time you eat anything, particularly after episodes of overeating but also when you have a planned meal or snack (see Step 2, ‘Instituting a meal plan’). This could include everyday events of life, such as having a minor argument with a friend or parent. It could be an event concerned specifically with eating, such as having been obliged by social pressure to eat something with which you were not happy. The circumstance could also be directly related to feelings of unhappiness, anger, anxiety, boredom or frustration. These might be related to your eating problem, to your concerns about your weight or shape, or they may be related to other aspects of your life. If you have overeaten, it is important that you try to specify for yourself what the circumstances were in which this episode occurred and what you were feeling and thinking at the time. This process is crucial to your coming to understand what sorts of things lead you to binge. A detailed knowledge of these factors is a major step towards intervening and overcoming your eating problems (see below under Step 3, ‘Learning to intervene’). This column should also be used for recording occasions when you weigh yourself (and how much you weigh). If you check your shape, you should record this here as well so you can get a good idea of how often this happens and what effect it has on you.
The example monitoring sheet shown in Figure 4 (page 119) is a real account of one person’s eating during one day. You will see that her day began badly because she weighed herself and discovered that her weight had increased by three pounds over the previous weekend. In the light of this discovery she resolved not to eat at all that day. She managed not to eat until 1.30 p.m., when she had an apple. She regretted this (indicated by the asterisk), because she feared that to eat anything at all raised the chances of her losing control later. In fact she managed to avoid eating until 5.15 p.m. At this point, having felt terribly hungry all afternoon, her resolve weakened and she had a bar of chocolate. She deeply regretted this; then she completely lost control and had a full-blown binge (all items marked with an asterisk), after which she immediately made herself sick (indicated on the monitoring sheet with the letter V). She was determined not to eat anything further that day, but she was not successful. At nine o’clock she succumbed to the powerful urge to eat and had another binge which was followed again by vomiting (twice). She also took ten laxative tablets (indicated on the monitoring sheet with the letter L). She was terribly upset by the loss of control and was very much afraid that her weight had consequently increased even more.
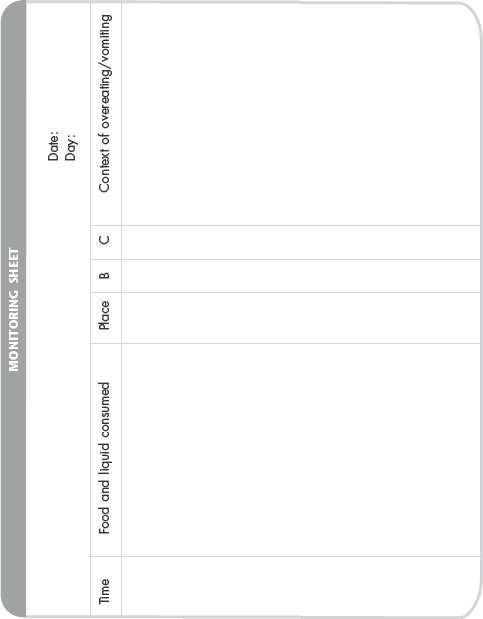
Two blank monitoring sheets are provided overleaf. Use these to record all the food you eat over the next day or two. In this way you can refer directly to the principles you are supposed to be following, outlined in the preceding pages. Having used these two pages, you should make your own monitoring sheets in a separate booklet, which you should then keep as a record of your progress.
Once you have been monitoring your eating for a week, you should review the week as a whole and begin to try to identify any patterns in your eating. This reviewing process will continue throughout the self-help program and will provide valuable information which you will use in deciding which techniques and methods will be helpful to you in regaining control of your eating. The kinds of questions you should ask yourself at this stage include:
These questions, continually reviewed, will provide you with a clearer understanding of the nature of your eating problem, which is crucial to your further attempts to stop binge-eating and restore your eating habits to normal. It is particularly important at this stage to begin to identify times and situations when you are especially vulnerable to binge-eating. Advice on how to deal with these situations is presented in Steps 2 and 3.
You should make a fixed appointment with yourself each week to review your monitoring sheets, record what you can learn from them, and make definite goals for the next week. If you are seeing a helper or advocate, it is useful to take along the results of these review sessions.
Note: Read through all of Step 2 before beginning to try to implement the principles outlined in this section.
The next stage of the program involves learning to eat regularly and in a controlled fashion. More specifically, it means that from now on you must eat three meals and two or three snacks a day. Many people, having read this, will be feeling that the prescription of a meal plan is a recipe for disaster. They will be saying to themselves: ‘If I abandon my efforts to diet and start eating meals and snacks I will gain weight and inevitably get fat.’ Well, of course, this would be perfectly correct if you ate meals and snacks and continued, in addition, to binge. But the meal plan is intended to displace the binges and, as a consequence, you will almost certainly be eating less overall than you were before. It is definitely not the case that by eating regular meals you will become fat.
The idea is to decide in advance exactly when you should eat and, by implication, when you should not eat. You will also have to decide what sorts of food you should eat and in what quantity. It is important at this stage that you eat according to a predetermined plan, and not according to when you feel hungry. At this early stage, you cannot trust your sensations of hunger or fullness and they should be ignored.
It is necessary for you to decide on a meal plan that will lay down when you should eat. The idea here is to decide in advance on the times when you will eat. This has a number of benefits. In particular, it permits or legitimizes eating at certain times; and it makes it explicit that at other times you are not supposed to be eating. Once you have decided on an eating pattern it is very important that you make every effort to stick to it. What this means is that at the times you have specified for eating, you must eat, even if you do not feel hungry and feel that you could manage to go a few more hours without eating. And during the periods between the times specified for eating, you must try your hardest to refrain from eating anything at all. The point of all this is to replace the pattern of alternating between not eating at all and overeating with a pattern of regular eating. For this to be successful it is necessary that there should rarely be more than a three- or four-hour gap between episodes of eating. This means that the meal plan must consist of three meals a day and two or three snacks. It is important to reiterate that once you have decided on a plan, the specified meals and snacks are not optional but obligatory; that is, you must eat when you have planned to do so, and you must try not to eat when you have not planned to do so. Clearly, the exact times of these meals and snacks must be tailored to your own particular circumstances; and it is probably wise to have a special plan for weekends, holidays and other times when your usual daily routine does not apply.
The following is an example of what would constitute a sensible meal plan:
You may well be alarmed by this example because it includes so many times for eating. However, it is important that your meal plan does not differ greatly from this example. The reason for this is that such a plan is effective at displacing binge-eating because the time between episodes of planned eating is quite short. So if ever you feel like eating when you are not supposed to do so, you can reassure yourself with the knowledge that it is not long until you will have a meal or snack.
Figure 5 Example of a meal plan and monitoring sheet
It must be stressed that each of the meals and snacks specified above would represent times when you must eat. As far as your monitoring is concerned, each time one of these episodes came up and you ate something in a controlled and organized fashion, you would indicate this on the sheet with a bracket. It is important that you stick closely to the times specified on your meal plan and do not eat before a meal or snack is scheduled; and, similarly, it is important that you do not postpone or skip a meal or snack. A typical monitoring sheet of someone who has established a meal plan (and is doing rather well) is shown in Figure 5 page 132).
If you have children you will need to decide whether to eat with them or to eat separately. For some people the children’s mealtime routine can provide a useful structure on which to map their own meal plans. For others, children’s meals represent a major problem as a time when there is a lot of food around which they find difficult not to eat. Leftovers can be a particular problem. You must decide in advance which system is going to be most helpful to you in sticking to your meal plan.
In the box provided (page 134), write down your meal plan: that is, the times when you should eat planned meals and snacks. The constraints of your life may make it necessary for you to have more than one plan. You may, as mentioned, need a special plan for weekends. Or there may be particular days when your work or other demands mean that you are traveling or are otherwise occupied at certain times. You need to specify plans which will cover all these known possibilities. Remember that there should never be more than three or four hours between planned meals and snacks.
It is not terribly important at this stage what you eat in your meals and snacks, as long as it is food with which you are happy: that is, food you can eat without it leading to a binge and food you can eat without having to vomit or take laxatives. This almost certainly means that it will be low-calorie food and, probably, diet food. This is not necessarily a problem, provided you are getting enough to eat. Most people with bulimia nervosa who begin a meal plan do, in fact, restrict their eating to low-calorie food and eat rather little. This can become a problem, particularly if you are rather thin, because you will be starving and unable to stick to your meal plan as a consequence. Thus, if, for example, for every meal or snack you ate a single apple, you would simply not be getting enough to eat and at some point in the day your control would break down and you would binge. It is, therefore, important, as already noted, that you get enough to eat.
What constitutes ‘enough’ is likely to be a problem for many people. There are three ways of dealing with this difficulty. The first is a simple matter of seeing what is happening to your eating: if you are trying to stick to a program of three meals and three snacks a day, and you find that an hour or so after your lunchtime meal you feel like a binge, then it might be the case that you are physiologically deprived and your lunches are too small. In such circumstances, if you increased the amount you ate for lunch, you would probably not feel hungry before the next scheduled snack and would be less likely to lose control and binge. A second strategy is to use someone else as a reference point. That is, choose a friend or relative who you feel is a ‘normal’ eater, and examine the quantities she eats in a meal. This might help you get an idea of how you should change how much you include in your meals. The third strategy is to buy some (non-diet) prepared meals for one from a supermarket as a guideline to how much food a meal should contain. As part of this process of deciding how much to eat you might even discuss the problem with a trusted friend or relative (see the section on ‘Talking to someone’ in Step 3). Or you could discuss it with your helper/advocate.
It is common for people at this stage to have considerable difficulty knowing what foods to include in their meal plan. The important point here is to try to eat only what you are happy with. You should avoid eating anything which you know will be likely to trigger a binge. This may well mean that you are the only person not having a second helping or not having a dessert. This can be embarrassing, but at least you will have the satisfaction of knowing that you have stuck to your meal plan and not gone on to binge.
Deciding what to eat can be a problem, particularly when you are feeling hungry. It is advisable, therefore, to plan in advance what you are going to eat. Some people find that this is best done immediately before a meal or snack; others find it helpful to sketch out a plan before going to bed at night. A good method is to use the back or top of your monitoring sheet for planning the next day’s eating (Figure 5, page 132). You will then be able to check how you are doing as you fill in the sheet throughout the day. If it is difficult for you to specify exactly what you will have for each meal or snack, put down a few limited alternatives with which you will be happy. You will have to discover whether planning immediately before a meal or a day in advance is best for you.
It is useful to remove all decisions about your eating from the actual time when you are eating. Planning meals and snacks ahead of time, as advised above, is one way of doing this. Another is to decide before you begin a meal exactly how much you are going to have. This can be helpful because otherwise it is easy to find that you have eaten more than you are happy with and then feel that you might as well go on and binge. A useful strategy here is to set out your meal or snack before you and decide that one item (say, a piece of fruit) will be the ‘full stop’ to the meal. When you have eaten the ‘full stop’, the meal is over.
It is essential that you stick to the decisions that you have made in advance. If, having eaten your ‘full stop’, you think that you still feel hungry, you must try to ignore this feeling and abide by your decision not to eat any more. The reason for this is that your feelings of hunger or fullness cannot be relied upon; and if you do modify your eating plan in the light of these feelings your eating will soon become disorganized again. Perhaps the plan you devised in advance was wrong in certain respects and ought to be changed. However, it is generally unwise to make changes as the day proceeds. Rather, you can make a new plan for the following day having learned from the mistakes of today. Indeed, it is useful to examine your monitoring sheet at the end of each day to see what you can learn from it about the particular meal plan you devised and any difficulties in sticking to it that you may have encountered. This can help you improve the plan for the next day.
In rare cases, for some people who are fasting for long periods or who binge repeatedly throughout the day, the idea of instituting a meal plan for the entire day is too daunting a prospect. In these circumstances it is best to divide the day up into three or four chunks and begin by instituting an eating plan just for the easiest chunk (usually the morning). Once order is restored to this first segment and you are able to stick to a plan, you can then concentrate on the next least difficult part of the day, and so on.
Once you decide on an appropriate meal plan, do not assume that you will immediately be able to stick to it. You are almost certain to run into difficulties. The aim of the exercise at this stage is for you gradually to reduce the times of difficulty so that binge-eating becomes less and less frequent and normal meals and snacks become more and more the norm. And by examining your monitoring sheet at the end of the day you can learn from your mistakes and make changes to your future plans. Whatever has happened on a particular day, it is essential that you begin the following day afresh, committed to your meal plan for that day.
If you run into difficulties during the day you will probably feel tempted to abandon all efforts to adhere to your plan for the rest of that day. For example, you may be offered a piece of cake, eat it (when you should not have done so because it was not planned) and then go on to binge; and then immediately resolve not to eat at all for the rest of the day to compensate for having overeaten. This is a grave mistake and will almost certainly lead to further overeating. The important thing to do when something goes wrong is to get yourself back on your plan as soon as possible. So, assuming, in the example above, that the cake that led to a binge was offered at four o’clock, the right way to proceed is to resolve to eat the meal planned for supper. This may seem silly when you have just overeaten, but getting back on to the plan is your only real protection against further episodes of loss of control. Of course this is going to be extremely difficult and when you have overeaten the temptation to diet or to fast is likely to be very strong. This temptation must be fought and overcome. To give in and cut back on your eating is to undermine the value of the meal plan. The most you should allow yourself to do is to sit down in advance of the meal with your meal plan and replace certain filling items (like a sandwich or baked potato) with lighter, less filling food (like fruit or yogurt). Even this process of making substitutions in your meal plan can be dangerous, because the urge not to eat at all could be very strong and you may be tempted to replace the entire meal with, say, a few grapes. This will not work. The important thing here is to have the meal and for that meal to be a genuine one.
It is often very difficult to follow this advice, especially after a full-blown binge. At such times you are likely to feel disgusted and ashamed of yourself, and to feel particularly acutely the loneliness of trying to sort your problems out on your own. Although it is, of course, terribly difficult to do so, it is important that you find a way of picking yourself up and carrying on. It might be helpful at such times to ask yourself: ‘Have I made any progress at all? Because if I have, then, however bad I feel at this moment, it is this progress which is really important.’
It is inevitable that there will be slip-ups in the course of your making progress towards recovery. And they will make you very unhappy; at times, they might make you feel hopeless about ever really changing. But, if you do not allow such slip-ups to overwhelm you, it is possible to learn from them and to move forward. It is particularly useful to discuss these slip-ups with a helper, and to talk about your reaction to them, and how you can learn from them.
There will be occasions when, through no fault of your own, your plans for the day are disrupted. For example, just before you sit down to have lunch, a friend arrives and insists that you accompany her to a restaurant. The way to cope with this is to accept that, from time to time, your plan will have to be revised in the light of unexpected events. Try not to panic when this happens, but instead take a moment to yourself to make changes to your plan for the rest of the day on the basis of the new developments. In general, you should try to change as little as possible, so that the revised plan remains close to your original plan.
Special occasions will arise when you will not be able to stick to your usual plan. You may be obliged to go to a wedding reception, or you may be taken out to dinner by friends or parents, and so on. It is not always possible to avoid such circumstances and, although it is best to be fairly strict about adhering to your meal plan, especially in the early weeks, such occasions can present you with a useful exercise. In such circumstances, although your normal plan will not be appropriate, it is essential that you do have some plan for that particular day, and that the plan is as close to your usual meal plan as possible.
It is a bad idea to attempt to deal with a special evening occasion by fasting throughout the day. It might seem like the safest strategy, given that you know you will be eating a large meal in the evening. But it would be far better to make a minor adjustment to your routine by, say, planning to eat as usual until the special evening meal, planning to have only a starter and a main course at that meal (choosing light food with which you will feel comfortable), and, given that the meal is likely to go on for a rather long time, planning to skip the late evening snack. It is essential that you do not attempt to eat less the following day because of the previous evening’s meal: you should immediately return to your normal meal plan. If you try to compensate by eating less it is very likely that at some point in the day you will binge. It is worth remembering that no one meal can have a significant effect on your weight.
The purpose of establishing a meal plan is to displace binge-eating with ‘normal’ eating. For most people, as this becomes increasingly successful, the number of times they feel it necessary to make themselves sick will correspondingly decrease. If you don’t binge you won’t feel the need to vomit. For this reason, it is often not necessary to direct any special attention at trying to stop vomiting.
There are two exceptions to this. Some people find that, on occasion, even when they have stuck to their meal plan and eaten exactly what they planned to eat, they feel full, perhaps even bloated, and they become anxious that if they don’t vomit they will become fat. If this happens you must try to resist the urge to vomit. Remember that vomiting encourages overeating and will therefore work against your efforts to stop binge-eating. If you experience such feelings and fears, it is important to try to distract yourself until the urge to vomit has passed. The first time you do this it may take some time for the urge to vomit to pass; but, if you do resist this urge, the next time it arises it will pass more quickly and after a while the urge will disappear altogether. You must experiment with what sorts of distractions work best for you. Most people find that activities like reading or listening to music are not helpful. In fact, apart from going for a walk, which some people do find helpful, solitary activities are probably best avoided if possible. Being with people can have a calming effect and also makes it difficult to escape to vomit.
The second exception concerns those people who get into the habit of vomiting not only after a binge, but after eating anything at all. If this is what you do it is essential that, in addition to establishing a meal plan, you work towards eliminating vomiting altogether. Some people can manage this by simply saying to themselves: ‘I shall only include in my planned meals and snacks the sort of food I am prepared not to vomit, in the sort of quantities I am prepared to hold down.’ Other people find achieving this end more difficult and if you are one of them it is best to proceed more gradually. Divide the day up into six chunks (early morning, late morning, early afternoon, late afternoon, early evening, late evening). Ask yourself during which of these would it be easiest (or least difficult) to eat the planned meal or snack without vomiting. Once you have made this decision, you should eat without vomiting during this time. Use the same sort of distractions as those described above for coping when you have eaten. Once you can eat regularly without vomiting during this chunk of time you should decide which is the next easiest time and eat the planned meal or snack without vomiting during this time (as well as during the time you have already eliminated vomiting). In this way vomiting should be gradually eliminated altogether.
A common complaint of people who are putting a lot of effort into planning ahead and trying to stick to a meal plan is that they find that they are having to think about food and eating even more than they did when their eating was completely out of control. In a sense, they complain, the treatment is making them feel worse! This can be distressing but it should not be a cause for real concern because it is a phase which passes in a matter of a few weeks. It is simply the case that, if your eating habits have become very disorganized, to restore them to normal it is necessary, for a period of time, for eating to occupy a particularly important place in your life.
Many people who begin eating according to a meal plan of the sort described above also find that they become increasingly concerned about their weight and their shape. They are convinced that they are gaining weight and they feel fat. This is an understandable reaction in someone who has previously been attempting to eat very little. However, if you find that you react in this way, it is important to remember that it is a psychological reaction to the change in your eating habits rather than a genuine signal of what is happening to your weight and shape. You will be checking your weight weekly, so you will be able to confirm that replacing binges with regular meals and snacks is not in fact causing you to gain weight or become fat. These concerns and preoccupations will gradually diminish as you become more confident of your control overeating.
It is important to be clear about what constitutes a ‘good day’. Until now you may well have seen as a ‘good day’ one in which you have been able to avoid eating altogether or, perhaps, managed not to overeat. However, once you establish a meal plan, a ‘good day’ is one in which you have been able to stick to your plan. You may have a constant struggle throughout an entire day fighting urges to binge when you were not supposed to be eating, forcing yourself to eat planned meals when you desperately wanted to fast, and resisting the urge to vomit; and, at the end of such a day you may feel exhausted and demoralized. However, if, despite the great struggle, you were able to stick to your meal plan, eat what you were supposed to eat at the scheduled times, and avoid eating in between scheduled times, then that day was a ‘good day’ – a personal triumph, in fact! And the more such ‘good days’ you have, the easier sticking to the meal plan will become.
It is important to add here that if you have one or two slip-ups during a particular day, this does not mean that the day has been ‘ruined’, and it is important for you not to see it in this way. If you regard an unscheduled bar of chocolate, for example, as a total disaster, there is a risk that you might be tempted to abandon your attempts at control altogether, feeling that the day has already become a ‘bad day’, so you might as well binge and start afresh the next day. This is a very common trap and one which you must avoid. If you find that you tend to think in terms of ‘good days’ and ‘bad days’, you might find it helpful to think of each day as being divided into smaller sections or units. Thus, the period between breakfast and the morning snack could be regarded as one unit, that between the morning snack and lunch as a second unit, and so on. Each unit during which you manage to keep control can then be viewed as a separate achievement. It will be apparent that a slip-up in the early afternoon has only ‘spoiled’ one of the six or so sections of the day; and if you can then return immediately to your plan for the rest of the day, as advised, you will still have had five ‘good’ sections out of six, which is certainly not a ‘bad day’.
Note: Read through all of Step 3 before beginning to try to implement the principles outlined in this section.
If you are trying to stick to a meal plan you have already gone some way towards replacing binge-eating with ‘normal’ eating habits. However, it is likely that it will, at times, be very difficult for you to stick to this plan; and it is also likely that, at times, you will have a powerful urge to binge. It is essential that you develop strategies for dealing with these difficulties. This section contains a number of suggestions designed to help you both in your efforts to stick to your meal plan and in your attempts to resist the urge to binge.
Establishing a meal plan and attempting to stick to it can be a formidably difficult task. It is asking a very great deal of yourself to expect to be able to manage this entirely on your own, even with the assistance of a detached helper/ advocate whom you consult for advice and support. It can be enormously helpful, additionally to enlist the assistance of a close friend or relative. This is not because they can then take control and make all the decisions. No one can take over this task and do it for you. But they can help by providing you with very particular kinds of practical assistance. For example, it can be a great help to arrange to have some of your evening meals with someone else and to spend time with them afterwards. Also, if you know that it is going to be difficult for you to resist eating at a particular time (when you are not supposed to eat), it can be helpful to arrange to spend time with someone else. Similarly, if you can drop in on someone or telephone them when you are feeling particularly like binge-eating, this can see you through a difficult time.
Now, of course, much of this can be achieved without confiding the real reason why you are seeking companionship. However, the secrecy and deceit that is so often such a major part of the lives of people who binge is a great burden which itself causes much misery. It can be a considerable relief to tell someone of your troubles and not to have to keep up the constant deception. Also, someone who knows of your particular difficulties can be much more help to you than someone who does not. You may well feel extremely apprehensive about telling anyone about your problems with eating for fear that they would not understand and would think poorly of you. If you choose someone you respect and trust this really is most unlikely. It is a sad fact that almost all women within our culture are concerned about their weight and shape, and a great many have problems of some kind with eating. It is not at all difficult for them to see how such problems can become more serious. Almost invariably the people in whom one confides are anxious to be as helpful as they can be. If this is hard for you to accept, think of a good friend and ask yourself how you would react if she came to you in distress and confided some personal difficulty (say, that she was secretly drinking excessively or was shop-lifting), and think how you would react. Surely it is reasonable for you to expect as much acceptance and sympathy as you would be prepared to give.
It is important to stress that the assistance such a friend or relative can provide you with is quite different from the help you could get from an outsider whom you consult as an independent advocate or helper.
However resolved you are and however much forethought you put into it, it is not easy to stick to a meal plan. Many things can happen during a day to disrupt your plan and sometimes you will feel unable to stick to your good intentions. It is very common for people who binge to think that once something goes wrong with their eating there is nothing they can do to intervene – a binge is inevitable. In fact there is a great deal that you can do to intervene and such intervention is possible at all stages in the process. So, spending time planning ahead, spotting potential hazards and taking some form of evasive action, and recognizing the urge to binge early in the process and having a plan for what to do about it, are all forms of intervention which are effective at preventing binge-eating. While it may be hard to believe at this stage, it is even possible to stop a binge once you have started.
There are a number of simple measures you should take to make the task of sticking to a meal plan easier for you. A complete list would be endless, but the following are some of the main tactics people find useful:
1 Restrict eating to one or two specified areas within the house, such as the kitchen and the dining room. The areas where you usually binge (typically some private space, such as the bedroom) should be designated as places where food is never allowed. If you usually binge in the kitchen, it would be best if you found somewhere else to eat and never ate anything at all in the kitchen. If you find it impossible not to ‘pick’ at food while you cook, keep some chewing gum handy in the kitchen, and when you feel like picking chew gum instead. If you only have one room available to you, then designate a particular area for eating meals and snacks (such as a particular chair or place at table) and eat there and nowhere else.
2 When you do eat, eat slowly. Do not do anything else while you are eating like reading or watching television.
3 Before eating a meal, plan exactly what you will do when the meal is finished.
4 Restrict your supplies of food. Buy food in small quantities and do not keep large supplies of food readily available.
5 When shopping for food have a list of what you are going to buy. Do not shop for food when you feel hungry or think that you are likely to binge. If shopping is a particularly difficult time for you, arrange to shop with someone else. When you are planning to shop for particular items do not carry with you more money than necessary or credit cards.
6 Do not leave leftover food lying around. In fact, it is far better to throw leftovers away than for them to represent a threat to your control over your eating. This may feel wasteful and wrong; but it is better to be wasteful as a temporary way of helping yourself recover than not to be wasteful and thereby to make it impossible for you to stop binge-eating.
7 Do not allow anyone to bully you into eating anything you do not want. It is very common for people to try and press food upon you (e.g. ‘Do have another helping of dessert’ or ‘Go on: have a slice of delicious chocolate cake. I made it specially for you’). It is, at times, difficult to refuse such offers without being rude. However, it is possible to be firm and polite in sticking to what you want to do (e.g. ‘No thank you. It was delicious but I couldn’t manage any more’ or ‘No thank you. I won’t have anything because I have just eaten’ or ‘I shall be eating later and I don’t want to spoil my appetite’). If you are particularly plagued by the tyranny of others trying to force you to eat, you might find it helpful to rehearse two or three such phrases which you can then produce when required.
8 Finally, as pointed out earlier, in attempting to follow a plan for the day, it is important to take each moment separately. It is very common for people to say: ‘Well, I got that one wrong, so I might as well abandon any attempt to eat normally for the rest of the day.’ Indeed, it is essential if something goes wrong that you go back to your plan and see what it is that you are supposed to do next. If you can get back on to your plan immediately and stick to it for the rest of the day then you know that you have made real progress.
Most of the measures you must take to prevent yourself running into difficulties, or to extricate yourself from situations which have become problematic, you will have to work out for yourself by examining your monitoring sheets and seeing what situations are particularly difficult for you, and what tactics you find most helpful. Similarly, by paying careful attention to the circumstances in which you do lose control and binge, you can see what sorts of situations are particularly problematic for you and require special attention. It is important for you to be one step ahead of trouble. Planning the next day’s meals and snacks ahead of time is part of this process. But you can be even more focused in planning ahead and try to spot particular episodes or circumstances which are likely to lead to your overeating. You can do this by examining your monitoring sheets. It is likely that, after a week or two of monitoring, certain patterns will become obvious to you. You may find that you invariably binge after particular events, such as going shopping or being on your own with no particular plans or appointments. This knowledge allows you to anticipate when you are likely to run into difficulty and to adapt arrangements to make things easier for you. So, for example, if you find that you invariably binge when you are unpacking the shopping, you could arrange for a friend to be around at this time.
It is very common for people to find that their eating is particularly difficult to control after they have been drinking because alcohol tends to undermine the resolve required to maintain control. If this is true for you it will be very apparent from your monitoring sheets. The solution is a simple one: either drink in moderation or, if this is difficult for you, do not drink at all. You should be very strict about this while your prime goal is attempting to restore order to your eating habits. Once you are no longer binge-eating and are confident of your control, you can review this matter and decide when it would be safe to drink and how much you can drink without alcohol becoming a problem for you. It must be stressed that if you drink excessively you will not be able to make full use of this program and it is unlikely that you will be able to overcome your problems with eating.
It is important to have plans prepared for what you will do if things go wrong. For example, you may well have an urge to eat just after you have finished one of your planned meals or snacks. It is very useful to have a list of things you could do instead of eating (like going for a walk, having a bath, telephoning a friend, etc.); and when you feel an urge to eat you would then start working your way through the list until the urge passed. It is common for people to say: ‘If I have a strong urge to binge, however long I postpone it, in the end I will succumb.’ They feel that it is almost as if the binge has a will of its own and that in the end, if it is lurking, it will get them. In fact, if you do intervene and prevent a binge, the urge to eat does pass; and, of course, it is soon time for a planned meal or snack when eating is quite legitimate. Intervening in this way is not easy. At first it might even seem impossible. But you can be reassured that each time you do intervene successfully you make intervening in the future that much easier. And the more often you intervene successfully the less often the urge to binge will arise.
You must give careful attention to the preparation of your list of things to do in order to overcome the urge to binge and delay eating until the next meal or snack. This list can include any activity which you feel might help in this regard, but the following guidelines may be useful:
The list you do make can obviously be added to or subtracted from as you try out the effectiveness of your activities in various situations. It is a good idea to carry the list with you, so that when you feel an urge to eat you can immediately consult it and decide which of the activities you might use in that particular circumstance to tide you over until the next meal or snack time. The two pages that follow are provided for you to write in your list. Use the first page to write in a provisional list; you should amend this as you gain experience of what does and does not work for you. Once you are confident of what the most effective activities are, write them down on the second page as your updated list. You can always update the list again if you discover anything particularly effective later.
Note: Read through all of Step 4 before beginning to try to implement the principles outlined in this section.
It is very common for people with difficulties controlling their eating to binge in response to all sorts of problems which overwhelm them. These problems can concern issues to do with food and eating as well as with countless other aspects of life, such as work, family, friends and so on. It is important that you develop a strategy for identifying problems, addressing them and generating solutions other than eating. Sometimes the identification of the problem is easy: you might see, when making plans for the next day, that some event represents a potential obstacle to your meal plan. For example, a friend you have not seen for a long time has announced that she will drop round and you feel you should make something special for the occasion; or you know you will be extremely nervous because of a job interview in the afternoon and will not feel like eating all day. At other times identifying the problem will be more difficult. You may feel anxious or miserable and know that this makes you vulnerable to the impulse to overeat. It is easy in such cases to identify the problem as an urge to overeat, when the real problem is whatever it is that is making you feel anxious or depressed. For many people with eating problems the urge to overeat is an automatic response to problems of any kind. When such an urge arises, it is therefore important to ask the question: ‘Why do I have an urge to overeat now? What is the problem that lies behind this feeling?’ Of course, the answer to this question often will have been that you have not eaten enough (or at all). But if you are sticking to your meal plan and eating a reasonable amount of food, then there must be some other answer. It is important for you to try to identify what the basic problem is. Once you have done so you will be in a position to deal with the problem and you will not then automatically overeat. The steps shown below should be followed in helping you deal with the problem.
1 Write the problem out as clearly as you can on your monitoring sheet. If there is more than one problem, try to untangle the problems into separate ones; then deal with these individually.
2 Produce as many solutions to the problem as you can think of. You can be quite uninhibited about this because you want to be able to look at all possible solutions.
3 Examine each of your possible solutions and think about its implications: that is, precisely what would be involved, whether you realistically could see it through, and whether it is likely to be effective.
4 Choose what looks to you like being the best solution (or combination of solutions) and decide to act on it.
5 At the end of the day, review what has happened and consider whether your solution was effective. If it did not work out as it was supposed to, try to think what you might have done to produce a better outcome.
Problem solving as described above may look rather tedious and somewhat complicated. However, it is a highly effective technique and, with a little practice, it can be managed quite easily.* Figure 6 (page 166) shows two examples of problems someone identified and the solutions she generated, together with a statement of the outcome or ‘evaluation’.
For some people problem solving in the way described above, comes very easily. It is largely a formalization of what they have been doing in a rough way before. For them, the benefits of doing the problem solving more formally, as described, will be obvious and they will experience these benefits rapidly. For others, formal problem solving is something quite alien to their way of thinking and behaving; and they may struggle to use this technique effectively.
The following blank pages headed ‘Problem solving’ are for you to try to use the problem-solving technique in the way described. Over the course of the next week, on two occasions identify a problem and try to come to a resolution, using the spaces provided. Then take these to your ‘helper’ and talk them over together. This discussion can be especially useful if you have gone through a problem-solving exercise and it has not worked as well as you might have hoped. You will then be able to look at what options you might have considered and how this might have affected the outcome.
Figure 6 Examples of problem solving
Feeling depressed can be a major obstacle to overcoming eating difficulties. People sometimes react to relatively minor setbacks in their efforts to deal with their eating problems by becoming totally demoralized and fiercely self-critical. As a result, their confidence and strength of purpose are undermined and they find it even harder to control their eating. It is important to accept that overcoming your problems with eating is likely to be a struggle and that you will inevitably not succeed all the time in everything you are trying to do. If you succeed at something you are making some progress and you should give yourself credit for this; and where you do not succeed you can learn something which can help you in the future.
Sometimes more general feelings of depression, not specifically related to eating or weight concerns, also lower morale and make it hard to control eating. If it is apparent from your monitoring sheets that this represents a pattern, you should try to think what it is that is making you feel depressed. Treat it as a ‘problem’ in the manner described above and try to find solutions. You might find a self-help book useful, such as Paul Gilbert’s Overcoming Depression.
Occasionally, people are so depressed that they are seriously incapacitated. They do not sleep properly; wake up early in the morning; feel tired all the time and completely without energy; find concentrating impossible because of their preoccupation with gloomy thoughts and are consequently unable to work; they cannot see any hope in the future for themselves and life to them does not seem worth living. If you are feeling persistently this depressed it is important that you go and talk to your doctor soon. You can get help; if you do, your mood will improve and you will then be able to make use of this manual and deal with your eating problems.
It is common for people who are monitoring their eating to find that binges are triggered by problems in their relationships with their parents, husband or boyfriend, or other close friends. If you find that this is the case for you, it is worthwhile trying to deal with this area as a ‘problem’, in the way described above, and trying to specify exactly what the nature of the difficulty is and what you can do about it. Often a pattern emerges from the monitoring sheets which makes it clear where the problem lies. It could be something very specific, like your mother unwittingly forcing you to eat food you do not want; or it might concern a more general issue with parents, such as difficulties with independence. Similarly, with a husband or boyfriend it could relate to something concerning eating, or some more general aspect of the relationship. There are, of course, any number of possibilities here. The point is that by writing down what the nature of the problem is and by thinking about what sorts of solutions might be possible, you create the possibility of breaking a cycle. You may even decide that your relationship problems are of such importance that you should seek professional help in resolving them.
It is very common for people who have difficulties controlling their eating to report that they feel fat, and that this feeling makes them diet; but at the same time, feeling fat distresses them and makes them want to eat. Most people do not question this feeling. It regularly occurs and they assume that it is a feeling which is a genuine reflection of the state of their body. However, if you record on your monitoring sheet every time you have a strong sense of feeling fat, it is likely that you will discover an interesting fact: namely, that this feeling arises in all sorts of different contexts, some of which are clearly related to circumstances surrounding food (such as after having eaten a meal) or shape (such as wearing a tight dress or going out with a thin friend), but many of which have nothing at all to do with food or eating. In fact, you may well discover that, like so many people whose eating is out of control, for you ‘feeling fat’ has come to constitute an automatic response to any negative emotion. You may just feel ‘bad’ and immediately convert this into feeling ‘fat’. But there are many events or circumstances which could be responsible for your feeling bad and they should be recognized for what they are and addressed and resolved. The way to proceed is to record on your monitoring sheet whenever you feel fat and ask yourself: ‘What is the real problem that is making me feel bad?’ Once the problem has been identified you will be in a position to think about appropriate solutions.
Preparing food for friends or relatives and eating with them should be a pleasurable experience. But it can be a nightmare for people with bulimia nervosa. All sorts of basic issues cause anxiety and confusion, such as: ‘What shall I cook?’, ‘How much should I prepare?’, ‘Do I serve everyone’s food myself or do I leave them to do it for themselves?’, ‘What size helpings should I serve?’, ‘Do I offer second helpings and, if so, how forcefully?’, ‘How long should the meal take?’, ‘What do I do with leftover food?’ These questions all pose serious problems which need resolving.
Two general principles might be helpful. First, try to avoid doing anything which you know will create difficulties for you. So, if you are preparing a special three-course meal and including a conventional dessert would be a problem, why not prepare some exotic fruit instead? And, if leftovers are going to be difficult for you to resist, arrange for someone else to remove them or, if this is not possible, throw them away. Second, as a general rule it is a good idea to treat others as you would like to be treated yourself. So, for example, do not force food on to people, and give them as much choice about what is going to happen as possible.
REVIEW BOX 4
Note: Read through all of Step 5 before beginning to try to implement the principles outlined in this section.
It is possible that you will have managed to stick to your meal plan by eating a fairly restricted diet. So, you may well be managing to stick to three meals and two or three snacks a day, and in this context you may well have stopped binge-eating or reduced it to an occasional occurrence. But your control will remain precarious while you are only eating small quantities of low-calorie food. It is also the case that the effort involved in sticking to such a regime will mean that the degree to which you are preoccupied with thoughts about food and eating will not diminish and may even increase. It is essential to your continued progress that you make a real effort at reducing your tendency to diet.
There are essentially three ways in which people diet (as mentioned on page 16):
1 Simply trying not to eat: that is, going for long periods without eating, even to the point of fasting for days. The establishment of your meal plan will have eliminated this.
2 Attempting to eat very little (e.g., eating less than 1,000 calories a day). This method of dieting cannot be sustained if you are to be sure of avoiding binges.
3 Eliminating from your diet particular foods which are high in calories or which you feel make you binge. This method will also have to go because, as long as you retain the concept of ‘bad’ foods, or ‘forbidden’ foods, or ‘banned’ foods, or ‘dangerous’ foods, or ‘binge’ foods, or whatever you call them, you will be vulnerable to binge-eating under certain circumstances.
You should not attempt to deal with your desire to diet until you have managed to establish a regular meal plan and it has had a significant impact on normalizing your eating habits. This could take anything from two weeks to a few months, depending on the point from which you started. No definite guideline can be provided here but, as a rule of thumb, if you are sticking to your meal plan and not binge-eating on most days, you are probably ready to start tackling the dieting.
The meal plan has dealt with the first method of dieting: that is, fasting will have been eliminated by your eating regular meals and snacks.
It is often very difficult for someone who has been attempting to restrict the amount they eat for some time to have any idea of what constitutes a ‘normal’ amount of food. In fact, people vary considerably in how much food they require and no strict guidelines can be provided which would apply to everyone. It is necessary, therefore, that you experiment and discover for yourself what is right for you. Initially, it could be helpful to ask someone for assistance. Earlier it was suggested that examining how much others eat could help. This is certainly true. However, it is even better if you can talk to someone you trust about this and seek their advice and assistance. Better still is to arrange to have meals with them, as suggested above, and use these occasions as an opportunity to discover what constitutes a reasonable amount of food.
A word of caution must be added here. Many women diet and it would not help you to try to copy the eating habits of someone who is restricting her eating. In choosing a friend with whom to discuss this matter, and possibly with whom you might eat, try to find someone who is not particularly concerned about her weight and who is not dieting.
It would be a mistake to try to deal with the problem of deciding how much to eat by trying to follow some exact formula. In the end you must come to know what amounts are right for each meal and snack. For many people the prospect of such knowledge might seem an impossibility, and they may well feel that some guidance, at least at this early stage, is essential. In order to help them, as a very rough guide, an account of three days of ‘normal’ eating is given in Figure 7 (page 177). The amount of food eaten is roughly what an average weight woman who is eating normally would eat. The relative proportions of fat, carbohydrate and protein are also typical of someone whose eating habits are perfectly normal. These examples are merely illustrative and you should definitely not attempt to copy them. You may well need to eat more than shown in the examples and you should not be alarmed if this is the case.
An examination of your monitoring sheets will reveal that the foods you eat in a binge are usually those very foods you are especially attempting to exclude from your diet because they are ‘fattening’ or because you think that they trigger binges. It is very common for people to say ‘I never eat chocolate’ and then to discover that their binges contain a variety of chocolate bars. It is important that you come to be able to eat in moderation those foods you are avoiding, so ultimately you can make a rational choice about what you want to eat. If you continue to avoid particular ‘trigger’ foods, there will always be the threat that if you are presented with them you will binge. It is worth making the point here that no food is in itself fattening; and, conversely, that eating too much of any food can be fattening.
If you are still concerned that eating even a small amount of your ‘forbidden’ foods might make you gain weight, you might want to try a small experiment to convince yourself that this is really not the case. This experiment will involve weighing yourself more frequently than usual for a short period. If, for example, chocolate bars rank among your most difficult foods, decide to have a bar of chocolate on a particular day. Weigh yourself on that day before eating the chocolate and record your weight on your monitoring sheet. Then weigh yourself the next morning and record that weight. You will find that, contrary to your fears, eating the chocolate bar the previous day has made no difference to your weight. Acquiring this sort of concrete proof may seem silly, but it can be very effective as a counterbalance to irrational but habitual and powerful fears about the fattening effects of particular foods.
Figure 7 Three days of ‘normal’ eating: an example (showing UK/US equivalents of foods where appropriate)
You may still argue that, although one chocolate bar makes no difference to your weight and shape, you would certainly become fatter if you were to eat many of them every day. And you may be afraid that if you allowed yourself to eat any chocolate at all, you would be unable to control yourself and would eat large amounts constantly. This fear derives from your previous experience of avoiding forbidden foods only to find that you then ate large amounts of these foods in binges. It is very important to realize that the reason you ate large quantities of ‘forbidden’ food in binges was because you avoided them at other times. The fact that you binge is not proof that you cannot control your eating; it is proof that you have been exercising inappropriate control over your eating. Although this may seem difficult to accept, if you examine your monitoring sheets you will see that it is clearly the case. The truth is that by widening your diet and getting rid of the idea of ‘forbidden foods’, you will be less likely to binge.
The process of widening your food choice is a difficult one and one that can easily, if things do go wrong, create more difficulty rather than less. For this reason a precise set of guidelines is specified below. It is advisable to follow this program carefully. Although this may not seem necessary to some people, there is considerable potential here for difficulty and it is not worth running unnecessary risks.
1 Draw up a list of those foods you are avoiding either because you feel they are too ‘fattening’ or because you regard them as invariably, or often, triggering binges. If you find this task difficult, take a trip to a supermarket, armed with only a pen and paper (and definitely no money), and wander around the entire shop examining the shelf contents and writing down all items you would avoid for the reasons noted above.
2 Organize the list into a specific order or hierarchy with the item which presents the least difficulty (i.e. the one you regard as least fattening or threatening) at the bottom and the one which presents the most difficulty at the top. Figure 8 overleaf contains an example of what such a hierarchy might look like; but, obviously, every person’s own list would be different.
3 Divide the hierarchy into three classes of difficulty, grouping together those items that would cause you minor difficulty, those that would cause moderate difficulty, and those that would cause extreme difficulty. An example of one person’s hierarchy is given in Figure 8. Using the blank page which follows, create your own hierarchy of difficult foods in the way described above.
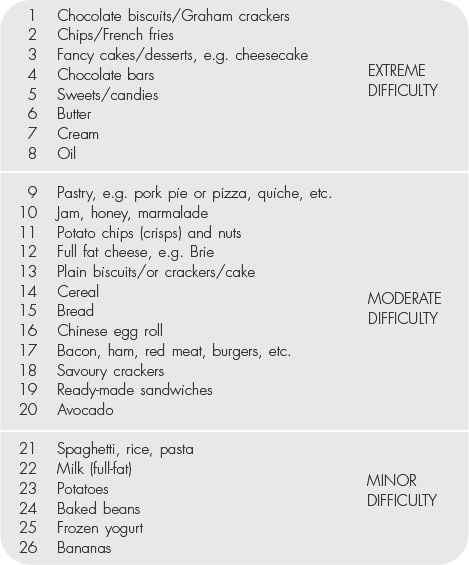
Figure 8 Example of a hierarchy of ‘difficult’ foods (UK/US equivalents shown)
4 Beginning with the group of foods which presents you with minor difficulty, using your established planning process, every second or third day, plan to eat one item from the list as part of your planned meals or snacks. Start with the least difficult or problematic item in the class. It is important that you plan this at a time when you feel you will be particularly safe, such as when you are eating with a friend or when it would be impossible for you to get at other food supplies. If, when the time comes, you have any doubts about whether you will be able to manage to eat the particular item without trouble ensuing, then do not eat it. If necessary, throw it away.
You should stick with the ‘minor difficulty’ class until you feel able to eat all the items in this category without difficulty and you feel that they ought no longer to be on your list of avoided foods. It is not possible to say how long this will take. But two or three weeks at each level is probably how long most people will need. Some will be able to move up the hierarchy more quickly and some will need to move more slowly. Once you are comfortable with the food in the first class, those items which used to present minor difficulty, you can go on to the ‘moderate difficulty’ class. However, it is much better to proceed with too much caution and to remain with the ‘minor difficulty’ class for an extra week, rather than move on when you are not really ready to do so. However long it takes, you should not move to increasingly difficult classes of food until there is nothing you cannot eat without anxiety in the one you are tackling at present.
5 Finally, having learned that you can eat anything you want, you should decide roughly how often you would like to eat that sort of food and in what quantity. Clearly, it would be unwise to fill your day with the high-calorie and bulk food you previously ate in binges. It would also not be healthy. But it is important to remember that if you decide never to eat these foods at all they will again come to represent a threat to your control over eating. For example, if you were avoiding chocolate, it might be sensible to decide to have a chocolate bar as ‘dessert’ for lunch, or as a mid-afternoon snack, three or four times a week. Again, if this prospect is alarming to you, it is worth reminding yourself that, if chocolate bars are the issue for you, eating three or four a week as part of controlled binge-free eating is probably a tiny fraction of the number you would be eating if you were still bingeing.
It is not possible to be precise about the length of time it will take to work through this program of eliminating dieting, because it will differ for each individual. The time taken is really not important, provided that progress is being made; and progress means being able to eat a wider and wider range of food without fear. The job is done when you can eat anything, in moderation, without becoming afraid that it will cause you to get fat or to lose control and binge. If you are not sure whether you have reached this point, it might be helpful to ask yourself whether you could go out for dinner to a restaurant with a group of people, with whom you are comfortable but whom you do not know well, and order a three-course meal, or whether you could go to a dinner party with friends and eat whatever it was that was served. If you are able to say to yourself: ‘Neither of these situations would present a serious problem to me because I can eat anything I like without overeating and without it making me fat,’ then this particular job is done.
You may be unsure how to judge the significance of the progress you have made. You may have reached the point where you can stick to your meal plan, where you no longer binge or have the urge to overeat, and where there are no foods that you cannot include in moderation in your meal plan. While this would be wonderful progress, there are two further issues which need to be addressed. One concerns your ideas and beliefs about weight and shape (see Step 6 below). The other concerns your ability to deal with all situations in which food has previously presented you with difficulty. For example, many people find it a great problem to eat food someone else has prepared and served, because they have no control over the composition, quantity or calorie content. Some people find eating in certain social situations difficult, such as at a dinner party where they feel their eating is under the public eye. It is very common for people to be unable to manage situations where small amounts of food keep appearing, such as cocktail parties, or where virtually limitless amounts of food are laid out, such as buffets.
To be completely secure about your eating you should come to be able to deal with any situation. The way you achieve this is by following the same principles outlined above for being able to eat all sorts of food: you make a list of all the situations you know you would find difficult, and then you practise coping in them under safe circumstances, starting with the least threatening and gradually moving on until you feel able to manage any situation in which you might find yourself.
An example of one person’s list of difficult situations is shown in Figure 9 (overleaf). In the box headed ‘Difficult situations’ (page 187) write down as many different situations as you can think of where you might experience problems in dealing with food. Then, whenever you are able to do so, try coping in the particular circumstance and make some notes about how you have managed.
Figure 9 Example of a list of ‘difficult’ situations
* In fact, there is very good evidence for problem solving being a highly effective treatment in itself. In one study published in the British Medical Journal, it was found that, among a group of patients consulting their general practitioner for treatment of a major depressive disorder, those who received six fortnightly sessions of problem-solving training improved as much as those who received antidepressant medication.
It is almost certainly the case that if you had not been concerned about your weight and shape in the first place you would never have started dieting and would never have lost control of your eating and experienced all the problems that followed. In some sense, for your eating problems to be put completely behind you, you need to change your mind about how important weight and shape are to you. It would be quite unreasonable to say that they should become unimportant to you, since nearly all women in our society are concerned about their weight and shape to some extent and it is not realistic to expect you to become less concerned than is usual. However, it is important in your case that these concerns change in their intensity and their form so that they do not dominate your life and dictate how you behave, especially your eating. Clearly, this is going to be a long and difficult task. For some people, as their eating becomes increasingly ‘normal’, and there is space in their lives for them to develop their interests and commitments, their concerns about weight and shape naturally become increasingly less important. Others have to give special attention to changing the way they think about themselves and the importance of their shape and weight.
There are a number of books which deal with the question of why weight and shape are of such major importance to women. They are mostly feminist works which expose the social pressures to be thin and the consequent tyranny under which women suffer. It is worth reading one or two of these books and considering the wider social origins of women’s weight and shape concerns. Examples are Susie Orbach’s Fat is a Feminist Issue and Naomi Wolf’s The Beauty Myth.*
It is likely that, at present, how you feel about your weight and shape is central to how worthwhile you feel you are as a person. If your weight falls, you feel you are a better person. If your weight rises, you feel a failure, incompetent and unlikeable. You can judge the extent to which this is true for you by examining your monitoring sheets to see how you have felt after weighing yourself. This tendency to judge self-worth in terms of weight and shape almost always underlies eating problems. Indeed, holding these attitudes probably explains why you began dieting in the first place and why you continue to be so deeply concerned about your weight and shape.
In order to reduce the intensity of these concerns, and thus make it easier for you to maintain control of your eating, it is important to reconsider the link between your self-esteem and the shape or weight of your body. One way of doing this is to make a list of the attributes which you consider valuable in other people. What things do you value about your friends, for example? Such a list might include things like how reliable and trustworthy they are, how devoted as parents they are, how dedicated to their work they are, as well as things like sense of humour, and so on. It is likely that their physical appearance, and especially their weight and shape, would rank very low on your list of valued attributes. If you are not sure about this ask yourself whether you would stop being a friend of, or start to despise, a friend if she were to gain, say, ten pounds (while retaining all her other positive characteristics).
Another useful thing to do would be to ask a trusted friend to provide you with a list of your ‘good’ and ‘bad’ qualities, as she sees them. Again, you would almost certainly find that your weight and shape do not feature in any major way on either of these lists. Thus, it should become apparent that weight and shape are not important in how you value others; and they are not important in how others value you. Part of changing your mind, therefore, involves adjusting your method of self-evaluation so that you apply to yourself the same standards which you apply to others and which they apply to you. This is not achieved merely by making a decision to think differently about yourself, but the first step is to be aware of when you are giving an exaggerated importance to your weight and shape. It is useful to record on your monitoring sheets examples of instances where you attributed negative events or feelings to your weight or shape, and then enter into a kind of debate with yourself to try and reach a reasoned and rational perspective. For example, if a person to whom you are attracted does not pay much attention to you at a social gathering, you might find that you instantly think something like ‘he’s not interested in me because I’m too fat’. On reflection there might be many other possible reasons why he behaved as he did, including reasons which have nothing at all to do with you. If you continue to monitor your reactions and deliberately look for other perspectives in this way you will find that gradually awareness of your weight and shape will assume a less prominent role in how you evaluate yourself and your circumstances.
Problems with eating often arise in the context of other sorts of attitudes which are more generally problematic, and which you might usefully address. Although these will differ from person to person, two types of habitual ways of thinking seem particularly common and you might find it useful to become aware of them as potential areas of self-exploration.
This is a tendency to have unrealistically high expectations of yourself. You might find that over the years you have, consciously or not, developed a set of rules for yourself about how to behave or how to be as a person, and that you are particularly hard on yourself when it comes to evaluating success or failure in living up to these rules. As an example, you might think ‘it is wrong to feel angry’, and then feel extremely guilty and self-critical when you do lose your temper, even in very provoking situations. Associated with this might be the tendency to be very unforgiving of yourself when you do make mistakes or fail to achieve a desired goal.
This harsh approach to your own ordinary human frailty means that your eating problem makes you feel even worse about yourself. This, in turn, makes you feel bad about your weight and shape, which makes you want to diet, which is the sure route to your binge-eating again. Changing these unrealistic expectations of yourself and such harsh self-evaluation is not easy, but it is worth trying. Again, you might begin by considering how you would evaluate a friend in similar circumstances. Would you be very critical of a friend for losing her temper in provoking circumstances, as in the example mentioned above? Would you condemn a friend for making a mistake? In any situation where you feel guilty or self-condemnatory, ask yourself whether you would accept or forgive similar behavior in your best friend and, if you would, try to apply the same sympathetic approach to yourself. In effect, treat yourself as you would your own best friend. If you find that perfectionism is a significant problem for you, you will find it helpful to read Overcoming Perfectionism by Roz Shafran, Sarah Egan and Tracey Wade.
This is a tendency to view things in absolute, ‘all-or-nothing’ terms. This principally affects thinking about weight and shape and about eating, but it can also affect more general aspects of life. For example, some people tend to see themselves at some times as a success and at other times as a total failure. In relation to their weight, they see themselves as either thin and attractive, or as fat and loathsome. They might think of a day when they ate very little as a great success, and one where they ate a little more than they were happy with as a total disaster.
Thinking in this all-or-nothing, black-and-white way can lead to considerable difficulty. Seeing small deviations from what you are aiming at as catastrophic can make you feel that you might as well give up altogether. In reality, things are never this clearly black-and-white; everything falls somewhere between the two extremes, and a realistic appraisal of the true nature of your circumstances will allow you to make a reasoned response.
It is not easy to change an all-or-nothing style of thinking. However, it is possible to do so. Whenever you find yourself responding in an extreme negative way to a situation (e.g., ‘This is a complete disaster’ or ‘this is absolutely terrible’ or ‘I am completely useless’), use your monitoring sheets to slow yourself down. Before accepting your immediate response, consider what evidence there might be against it. You will find that there is often considerable evidence against the catastrophic or disastrous conclusion; and if you allow yourself to consider alternative conclusions, you will be in a position to move forward positively. It is helpful to use your monitoring sheets to write down these extreme negative thoughts and your reasoned responses to them.
There are a great many groups run by people with eating problems, where people with similar problems meet to discuss their difficulties. Few people whose eating is seriously disturbed find that attending such a group is sufficient to help them overcome their problems with eating. However, some people find that a group of this kind can be particularly helpful in revealing how concerns about weight and shape dominate and destroy ordinary life. It is sometimes only possible to see the nature and implications of your views when you hear someone else expressing them. It may be worth considering attending such a group with this purpose in mind. However, there is a danger of which you must be aware: many people have very strong views about why people have eating disorders and about what sort of help sufferers ought to be receiving. If you are attempting to overcome your eating problems on your own with the help of this manual, it will not help you to have your efforts undermined. Therefore, before you commit yourself to attending such a group it would be prudent to try to find out exactly what sort of group it is and what its purpose is. Information about groups can be obtained from eating disorders associations (see the list of addresses and telephone numbers given in Appendix 1).
For people who overcome their problems with eating and resume ‘normal’ eating habits, disruption to the reestablished control over eating is always a possibility. So, after a year of normal eating, you might find, for example, that after having had an argument with your mother or your partner, or after a particularly stressful period at work, suddenly, out of the blue, you lose control of your eating and binge. Another way that control is sometimes lost is when, for a variety of possible reasons, people gradually slip back into dieting; their weight may fall, and suddenly they binge.
This can be very distressing and invariably the immediate conclusion drawn by the person is that she is back to square one. However, this is not so. The important thing to remember is that the significance of such a lapse (and a lapse is all that it is) has less to do with what actually happens than with how you react to it. So, if you react as if struck down by a catastrophe and go into a deep depression resigning yourself to a lifetime of binge-eating, you may well find it very difficult to restore order to your eating habits. If, on the other hand, you are able to see that there were special circumstances that led to the lapse and that it represents an unfortunate minor setback which you have the skills and the will to overcome, you will be able to get back on the track of normal eating quite quickly. If you are at all concerned and feel at all vulnerable to overeating, you should immediately go back to the beginning: reinstate monitoring, specify a precise meal plan, plan your eating ahead of time, and so on. You will find after a few days of such effort that your confidence will return and you will again be able to be more relaxed about your eating.
Once your eating is under control it is enormously tempting to say to yourself: ‘Thank goodness that is over. Now I need never worry about my eating again.’ This is a very natural and understandable reaction. However, it is one of which you should be wary. The concerns about your weight and shape which were the driving force in your eating disorder, even if they seem to have disappeared, remain an area of vulnerability in your life. So, at times of stress, when others in the same circumstances might become depressed or anxious or drink too heavily, you are liable to become concerned about your weight and shape and to want to diet. It is important that you are alert to such feelings and take steps to avoid acting on them. Indeed, if such concerns do arise you should treat them as a problem which needs to be dealt with formally (as described in Step 5). The danger signals to which you should be particularly alert are feeling badly about yourself because of dissatisfaction with your weight and shape, and the desire to diet.
REVIEW BOX 6
* Susie Orbach, Fat is a Feminist Issue, London, Paddington, 1978; Naomi Wolf, The Beauty Myth, London, Vintage, 1991.