Words slip out of your mind, suddenly you can’t seem to spell simple words, you forget the tasks you wanted to do, you forget where you put your To-Do list, you walk into a room and then wonder what you wanted to get, you can’t find your keys, you feel scattered in your thinking, and you can’t seem to focus like you used to. Does any of this sound familiar? If so, you aren’t alone. You aren’t imagining it. You may be in the beginning of menopause. What’s happening? Why do changes in the ovaries seem to affect your brain so profoundly?
During my residency at Johns Hopkins, one of the specialty rotations was the Dementia Research Program. I remember being very struck upon learning that dementias of all kinds are about four times more common in elderly women compared to elderly men of the same age. I was bothered by this statistic because, at the time, no one had any explanation for this marked difference in dementia rates between women and men, and researchers were not thinking about studying female hormone effects on the brain.
Based on current projections, a female born in 1994 has a one in six chance of developing Alzheimer’s, if she lives to an average life expectancy of about eighty years. For women, this lifetime risk is greater than the lifetime risk of breast cancer. A male born in 1994, who lives to the average male life expectancy, has a one in sixteen chance. It’s about time we begin to research the role of decline in estrogen after menopause as a possible factor in women’s higher rates of dementia. This crucial research has now been underway for more than two decades, particularly in Canada, Australia, and Japan to determine the effects of estrogen on nerve cells in the brain, memory pathways, and cognitive function. The United States has lagged behind these other countries in paying attention to the importance of ovarian hormone effects on the brain but has recently begun such studies. Let’s look at what has unfolded in our knowledge about the many ways estradiol helps preserve our critical thinking and memory abilities. But first some definitions and explanations that will help you understand these complex neuroendocrine connections.
Dementia is a term that means generalized loss of the brain’s ability to retain, perceive, integrate, utilize, retrieve, and act appropriately on information, called cognitive function. It is a group of brain diseases with a hundred or more different causes. Some types of dementia are treatable and reversible if the cause is caught early. An example is hypothyroidism. Loss of adequate thyroid hormone causes marked decrease of cognitive function and even full-blown dementia if left untreated, but is reversible if treated with thyroid hormone replacement. Alzheimer’s disease is another type of dementia that involves progressive, irreversible degeneration of global brain function. At present, we do not have any treatments that completely restore normal brain abilities in Alzheimer’s patients, even though some medications may help to delay progression for a while. Estrogen has a significant role in preserving normal nerve cell growth, repair, and function. Studies in Alzheimer patients now suggest that estrogen has the potential to reduce our later risk of developing Alzheimer’s disease by 40–50 percent.
Milder forms of memory changes that women describe during pre- and perimenopause are generally not the more serious dementia syndromes. Dementia is an illness that affects about 10 percent of the population on average. Menopause, of course, is a normal transition for all women who live long enough, and does not alone cause dementia. But if hormonal decline in women is one contributing factor that would help explain the gender differences in the terrible disease of Alzheimers, then we must consider this issue in helping women. To make a wise and balanced decision about whether to use supplemental hormones when our ovaries no longer make what we need, we all need solid information to guide us.
As I worked with hormonal effects on many parts of the body and the effects on brain-mediated phenomena, I began to wonder whether hormonal changes in women were more a factor than we had thought. When women talked about memory changes, they typically said these problems were worse, “before my period” or “during my flow.” These menstrual-cycle phases are times of declining or low estrogen. Women’s descriptions have been so uniform in the way they have talked about what they notice with memory related to these menstrual phases that I felt certain it was not all due to life stress or women being oversensitive to body-mind changes. I became convinced that there is an important effect of estrogen on memory. Fortunately, in the last several years, there are a number of new research studies in animals and humans that show some of the ways estrogen works in the brain to maintain normal memory function. I will describe these later in this chapter. But first, listen to the voices of these women.
I remember the poignant first appointment with Ann, a forty-six year old homemaker and community leader, who sat in my consult room in tears as she admitted her most terrifying fear:
My mother died of Alzheimer’s and it began when she was in her early fifties. I’m beginning to have memory problems, and I’m so embarrassed. I’m afraid someone will notice, and deep inside I’m really afraid it’s the beginning of Alzheimer’s for me too. I can’t seem to focus on my lists like I used to, I forget names, I go to say a word I know and suddenly it’s not there and I feel stupid. I can’t seem to add like I used to, and my mind wanders a lot. I’m really frightened. I just don’t want to end up like my mother. What’s happening to me? I do everything right, and I really try to take care of my health, there’s just nothing in my lifestyle to cause this memory problem. That’s why I’m sure it must be the beginning of Alzheimer’s. What can I do?
Her mother had an earlier menopause at about age forty-six, and then was told she had Alzheimer’s dementia at age fifty-five. Her sister’s menopause was at age forty-seven. Ann had a hysterectomy four years earlier at age forty-three, but had not had her ovaries removed. She was in good health, was not overweight, did not smoke cigarettes, rarely drank alcohol, exercised aerobically four to five days a week, and also followed a weight-training program. She even made sure she took all the vitamins that were supposed to help memory! She really was “doing everything right.”
Kay, a fifty-one-year-old writer, was disturbed by her growing awareness of difficulty finding the right words for her articles, as well as having trouble keeping her attention focused on getting a story finished on deadline. She described her observations:
My thoughts are fragmented, and I get distracted so easily. I never used to be like that. I was always one of the most focused people I know. My husband said I could tune out a freight train coming through the room. Now I feel like the slightest thing distracts me. I feel like my mind is flying in a million directions. What is happening to me? I’m really worried that I’m developing something like Alzheimer’s. What can I do? I don’t want to talk with my other doctors about this. They will just think I’m crazy, or tell me I’m under too much stress. But I’ve always lived with stress, and I used to thrive under the pressure of a deadline. That’s when I did my best writing. I just don’t understand this, and I’m frightened. This isn’t me.
Kay had not yet gone through menopause, although she had noticed her time of bleeding getting shorter each month, and the flow had decreased significantly. She had less bloating and breast tenderness before her periods now but said her irritability and difficulty concentrating were clearly getting worse and seemed to be much more noticeable the few days before her period and the days she was having her menstrual flow. In the past, the week of bleeding had been a week she typically felt better. She had also noticed a marked loss of interest in sex, and said she felt more tired than usual for her. She had not noticed any hot flashes, but said she had “these funny tingly feelings, like something crawling on my arms, and they come and go.” She thought she slept “pretty well.” She did not smoke and drank wine occasionally when out to dinner. She had no other health problems but did not exercise and was about ten pounds over her desired weight. Her mother went through menopause at fifty-four and never took any hormones. About twelve years later in life, Kay said her mother became “senile,” but she did not know any further information about what her mother’s memory problems had been. Her mother died at seventy-one of a heart attack.
Both Ann and Kay had a common finding on their evaluations: Each one had high FSH levels and low estradiol levels, typical of menopause. Both Ann and Kay had not thought they were menopausal. Kay was still menstruating (although her periods had gotten lighter, a clue that her estrogen was decreasing), and Ann’s doctor had told her she was too young to be menopausal. Kay’s doctor told her that since she was still menstruating her problems couldn’t be due to menopause. And since neither woman had experienced any of the usual symptoms, such as hot flashes, they had not considered the idea of menopause. All of Ann’s other laboratory studies were normal, but she did have a significant degree of bone loss for her age, in spite of her excellent health habits and exercise program. Kay’s evaluation revealed no other health problems except high cholesterol with a lower-than-desirable level of HDL.
Although it was the memory problems that brought each woman to see me, the bone loss for Ann and the cholesterol changes for Kay, along with the high FSH, were indications that each woman’s estrogen had been declining for longer than either one was aware. After reviewing all of their evaluation data and talking in depth about their respective options and their specific desires, both Ann and Kay decided to try estrogen therapy. Ann wanted to be sure she took steps that would help prevent further bone loss, and Kay thought her risk of heart disease was high, given her own cholesterol picture and her mother’s death from a heart attack. I talked with each one about what we know about the effects of estradiol on brain centers governing memory. I explained that in my clinical work with women, I had seen noticeable improvements in memory if the estradiol levels were restored to the normal levels of the first half of usual menstrual cycles.
That was two years ago. Ann called a month after starting the estradiol, and in an upbeat voice, said, “it’s better, I feel like I’ve got my own mind back again!” By the time she had been on the estradiol for six months, she reported that all of the previous negative changes in her intellectual ability had now resolved. “I’m back to my normal self. I feel great. I didn’t realize just how scared I had been than I might be getting Alzheimer’s like my mother. I am so relieved to know that what was happening was just the hormone changes of menopause and it could be helped.”
Kay also had a positive outcome: Her cholesterol profile improved, and she described feeling “my ability to focus on my writing has dramatically improved. I didn’t realize until I felt better just how much I had been slipping in my concentration. I can keep on track, the problem with words has gone, and I seem to do fine with organizing my thoughts again. I had no idea hormone drops at menopause could create such mental changes. Why doesn’t anyone talk about this?”
I think one reason not many physicians address these issues is that, in general, they have not been taught to think about the brain as a target organ of hormone changes. The focus has been on reproductive organs and the breast for the most part, with more recent attention turned to heart and bone health after estrogen declines. Frequently, when women ask health professionals about things like memory symptoms, the explanation is that memory and concentration changes are due to the stresses that women experience in this phase of life. As one woman succinctly put it, however, “Stress is ubiquitous throughout most women’s lives, and the memory changes don’t seem to be a problem in earlier years, so why now? It has to have some connection with hormone changes.”
Often, women don’t even want to admit to friends that these subtle memory changes are happening. Many are reluctant to talk any more about it, fearing they really are going crazy or developing some type of dementia, so they end up experiencing their uncertainty and fear alone. In health care settings, the questions and connections women think are important all too often get “written off” and go unanswered, leaving the fear and worry to intensify even more.
There was B.J., a fifty-one-year-old woman who wrote me a note after one of my seminars:
I had not been told that memory problems could be related to menopause. No one explained about memory problems, libido changes, insomnia, etc. I was mainly told about hot flashes. I really didn’t have anyone to talk to. None of my friends said they had these problems. Thanks for a wealth of information. It makes me feel better, I had really thought I was beginning to get Alzheimer’s and it had really bothered me. Now I have some ideas to talk with my doctor about.
May was fifty-three when I saw her for a consultation. She had gone through menopause at forty-nine, and had started estrogen therapy shortly thereafter to help her severe hot flashes. She was also concerned about osteoporosis, since her mother had lost two inches in height in the years after menopause and had died of complications following a hip fracture in her late sixties. May had been on conjugated equine estrogens, 0.625 mg for twenty-five days a month, with a progestin added on Days 16 through 25 of the month, since age forty-nine. She felt the estrogen had really helped her hot flashes and energy level, but she was concerned about continuing problems with memory. She talked about having trouble remembering what she had gone into a room to do, frequently forgot a word she was getting ready to say, had to write down telephone numbers as soon as she looked them up, and said she felt her brain “had a cloud pulled down over it. I just feel foggy, and that’s not like me, what’s happening?”
May’s evaluation was normal on all the tests for other possible causes of her memory problems. Significantly, her estradiol was low and her FSH was still in the menopausal high range even though she was on estrogen therapy. She was a tall woman and very physically active. I thought there were potentially two factors to consider in fine-tuning her hormone therapy: First, I thought she needed a different amount of estrogen, given her body build and level of physical activity that increased her metabolism of the hormones: second, I thought she would see a better improvement in the brain-related symptoms if she changed to a natural human form of 17-beta estradiol instead of the conjugated equine estrogens that she had been taking for so long. In my clinical experience, I find that women generally have a better response on brain function using the natural human estradiol since it is the bioidentical hormone the ovary made before menopause, and it fits properly, like a key in a lock, at the specific brain receptor sites that help to regulate memory and information processing.
She took my suggestion and changed to Estrace (17-beta estradiol) in a better dose for her, and we made sure this was providing what she needed by checking her blood level in about a month and-tracking her symptom improvement. In about a month, she described how she felt: “My memory is back, I can concentrate and focus well again. They really are greatly improved, I feel like I have my full abilities back. It’s hard to explain, but I just feel like my mind is clearer somehow.”
I do not think estrogen is a cure-all for memory problems. But it is, however, one of the most frequently overlooked factors affecting memory function for women. There are still many questions to be answered about exactly how estrogen works in the brain and what types of estrogen are needed for these brain pathways. There are many, many types of medical disorders and lifestyle habits that can affect the brain and cause memory changes. Most importantly, if you are having these kinds of symptoms, you need a careful and complete medical evaluation for the various types of problems, hormonal and otherwise, that can result in these mental and physical changes. While I think probably all of us could use more time and practice in relaxing, I do not think that’s the whole answer. Body physiology affects brain function, too. It’s that basic.
For those of you reading this who have had memory problems, at least be aware that checking your ovary and thyroid hormones much more carefully and specifically as I have described are critical dimensions of your health measures to address along with other tests and therapeutic approaches you may be taking. You don’t have to sit there and be frightened that something terrible is happening to you. There are ways to properly and thoroughly address your questions and ways of arriving at feeling better. Speak up, and be heard!
Meanwhile, here’s the latest information on estrogen effects on memory from worldwide research. The brain is truly an exciting frontier of hormone interactions and effects.
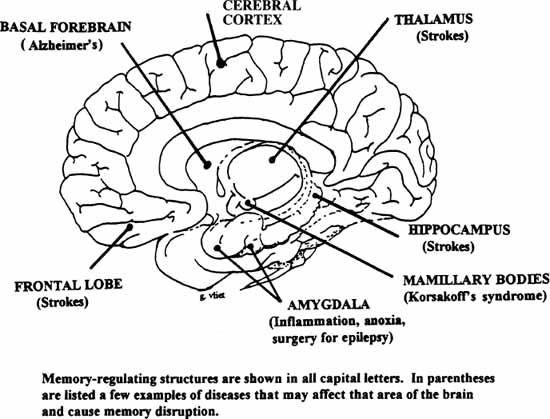
First some memory basics. To better understand what has been discovered about estrogen effects on memory, you will need to know some of the names of the brain areas involved in memory function, shown in the diagram below. Collectively, these structures make up the area called the limbic system, the mood-regulating area of the brain (rich in estradiol receptors, remember?) I described in chapters 3 and 4. Next to each of the memory-regulating structures, I have given an example of a disease process that typically affects that area of the brain and may cause memory disruption. The temporal lobes of the brain are major sites of these memory-regulating centers, so you may also see this term in discussions of memory.
The complex components of our memory system have only recently been mapped out. It used to be thought that memory traces were spread throughout the brain and could not be localized to any particular structures. More recent studies have shown the primary components of the memory system in the brain are the hippocampus, the mamillary bodies, the septal region of the limbic system, and part of the thalamus. There is a great deal that remains to be understood about how these various memory processes work in the human brain, but at present the memory system appears to consist of “storage centers,” which are located symmetrically in both hemispheres of the brain, primarily in the hippocampus and mamillary bodies. These centers in several parts of the brain provide back-up systems to prevent memory from being damaged or lost. If one hemisphere of the brain is damaged, memory will remain intact as long as the other hemisphere has not been injured. If both hemispheres of the brain involving memory centers are injured severely enough, the person has lost the ability to learn new material and store it for future retrieval. Memory function, having multiple memory circuitry centers in various parts of the brain, is thereby different from other brain functions, which tend to have more specific locations in one or the other hemisphere.
There are several different types of memory, but to simplify this we can conceptualize memory as short-term memory or long-term memory. Short-term memory comes into use in many day-to-day situations, for example, when you hear a telephone number or a name and remember it just long enough to use it. When a name, number or other piece of information is something you wish to remember for a longer period of time, it is converted to long-term memory. The hippocampus and mamillary bodies, along with the anterior thalamus and septal region, appear to be the major centers involved in converting short-term to long-term memory. Research does tend to suggest that this conversion process involves some type of actual physical change in the brain that may involve creation of new connections between nerve cells (estrogen stimulates growth of these new sprouts, or dendrites, to increase connections between neurons). Or this physical change may involve the creation of actual “memory molecules” that contain specific codes for the information involved. The brain also has a variety of mechanisms for remembering specific sound (auditory), sight (visual), touch (kinesthetic), smell (olfactory), and other sensory perceptions. These sensory memory centers are also widely distributed throughout the brain. Since memory is so crucial to survival, it makes sense that the brain has evolved multiple areas for memory storage of all kinds of information needed to keep the organism alive and functioning. The key role of the sex hormones in memory function also fits as part of the mechanisms that help species survive.
By now, many of you have seen the headlines in major newspapers about the research on estrogen and Alzheimer’s disease, and that estrogen deficiency may play an important role in causing, or worsening, some dementias. At the 1993 meeting of the North American Menopause Society, three researchers agreed that it is a significant, and underrated, factor in some of these aging-related disorders. Dr. Stanley Birge and his associates from Washington University in St. Louis believe that the new research findings support the theory that estrogen loss at menopause contribute to, along with genetic and environmental factors, the deterioration of the central nervous system known as Alzheimer’s disease and, potentially, other types of memory changes. Dr. Birge’s studies have also found that women over seventy who take estrogen have an improved ability in a balancing exercise, “tandem stance,” compared to women not on estrogen. He hypothesized that estrogen deficiency, through effects on postural reflexes and balance, may be a factor contributing to the unusually high rates of falls in elderly women.
Dr. Barbara Sherwin, at McGill University in Canada, has spent a number of years researching estrogen effects on the brain and her studies have shown improvements specifically in verbal memory in healthy postmenopausal women on estrogen compared to those who are not. In a separate study, Dr. Sherwin prospectively evaluated surgically menopausal women and found that those treated with estrogen did significantly better on several measures of cognitive function than the women given a placebo. Yet another prospective study of surgically menopausal women showed that taking estradiol specifically enhanced short-term verbal memory. None of these women had any type of dementia; they were all healthy postmenopausal and would not have been considered impaired in their memory abilities. Yet, the improved performance in the women on estrogen therapy was statistically significant and also fits with the self-reports I have heard consistently from patients in my practice.
At the Baylor College of Medicine and VA Medical Center in Houston, Dr. Karl Mortel studied postmenopausal women who were either neurologically normal or had mild cerebrovascular disease (CVD), which had manifested as transient ischemic attacks (brief periods of decreased oxygen causing symptoms similar to a mild stroke). He found that among women with CVD, women on estrogen therapy showed improved blood flow to the brain and improved cognitive function compared to the women with CVD who were not on estrogen. He concluded that estrogen therapy may be an effective addition to the treatment of older women with impaired circulation. His work fits with other research that has shown estradiol to have a relaxing effect on arteries, leading to more dilation and better blood flow to all organs in the body.
In 1991 and 1992 at the North American Menopause Society meeting, several researchers from Japan presented evidence of estrogen’s ability to improve cognitive function in elderly women who already had developed Alzheimer’s dementia. Dr. N. Hagino found that two-thirds of the fifteen study patients improved significantly in their communication with families, their ability for self-care, and memory for time and daily events. At the time, this research presentation did not get a lot of media attention. Since that meeting, we have seen a marked increase in the interest in, and attention given to, estrogen effects on brain function with additional studies now underway in the United States.
In an ongoing study of 8, 879 female residents of Leisure World, a retirement community in California, researchers at University of Southern California (USC) studied the medical records of those who died during the period from 1982 to 1991, and found 127 women whose death certificates mentioned either Alzheimer’s disease or dementia. These cases were then matched with those of the other women the same age who had not died of dementia. The resulting 635 cases were assigned to one of two groups: those women who had taken estrogen and those who had not. The researchers found that the estrogen users were 40 percent less likely to die of Alzheimer’s disease or dementia than women who had not taken estrogen. Another way of looking at it, the women on estrogen ran only about 60 percent of the risk of getting Alzheimer’s women had who did not take estrogen. The USC investigators further found that the higher the maximum reported dose of the estrogen, the lower the risk of Alzheimer’s. The risk of dementia also decreased with a longer duration of estrogen therapy. Women who had been on estrogen seven years or more had only 50 percent of the risk of dementia seen in women who did not receive ERT. JoAnn McConnell, senior vice president for medical and scientific affairs of the Alzheimer’s Association in Chicago, said “I think that these are very interesting results, and stronger than prior hints for an effect of estrogen.” These results are preliminary but bring up potentially important additional considerations in weighing the decision about hormone therapy for women who have a family history of dementia.
In 1986, H. Fillit and colleagues in a limited study found that some patients showed significant improvement in attention, mental function, and social interaction when on estrogen therapy. In 1989, another group of investigators using Premarin 1.25 mg daily as the estrogen therapy found that the women showed improvement in memory, orientation, and calculation. In 1994, Ohlura and colleagues did careful psychometric testing and showed objective improvement after ERT on measures of recent memory, distant memory, attention, orientation, personality, mood, and sleeping and feeding behaviors. Serum estradiol was measured in all study participants prior to and during ERT, with ERT resulting in mean serum levels of estradiol up to the values of mid-follicular phase of a healthy menstrual cycle in younger women. These study results suggest that the amount of estradiol given, and the serum levels achieved with therapy, have to reach such a desirable range to have the observed benefits on memory and other cognitive functions. The positive changes seen with ERT disappeared after estrogen was discontinued, thereby strongly suggesting estrogen’s major influence on these cognitive functions. An interesting outcome from this study was that the families of all of these patients had also seen the improvement in their relatives and requested that the estrogen therapy be continued long-term at the completion of the study. They didn’t need to wait for more controlled studies to be convinced of the positive cognitive effects of estrogen.
Since that time, a number of other studies worldwide have shown improvement in memory function in postmenopausal women given ERT, whether their menopause was a natural one or due to surgical removal of the uterus and ovaries. Ditkoff and colleagues showed an overall improvement in mood and quality of life in postmenopausal women on ERT. In a 1999 randomized double-blind, placebo-controlled clinical trial published in JAMA, Yale researchers found that even a three-week course of ERT changed brain activity in postmenopausal women performing memory tasks. This study went a step further in using magnetic resonance imaging (MRI) of the brain to show brain activation patterns both without and with ERT. The cerebral activity changes mimicked brain activation patterns typically seen in younger women. Sally E. Shaywitz, M.D., principal investigator, concluded that, “These alterations suggest a plasticity in the memory systems of mature women and that these neural systems are neither fixed nor immutable.” While the full mechanism of estrogen’s effects on the brain memory and cognitive pathways has not yet been clarified, there are a number of intriguing hypotheses about how it works, as we shall now see.
A number of studies argue for a direct effect of estrogen on memory, specifically on verbal memory, and there appear to be a number of neurochemical and structural ways estrogen exerts its effect. The biochemical and nerve structure studies have been done in animals. While animal studies cannot always be extrapolated to humans, what we have learned about rat brains in other areas of research seems to also apply to human brains at the biochemical level. There is no practical way to measure these types of biochemical and nerve cell structural changes in people, so the animal research provides a working model of what to look for in humans in later clinical trials. Dr. Bruce McEwen, head of Rockefeller University Neuroendocrinology Laboratory, and investigators from other countries, have done extensive research on the effects of estrogen on brain tissue, and have collectively found the many estrogen effects summarized in the chart that follows.
Dr. McEwen and other neuroendocrine researchers have concluded that the brain is an important target organ for estrogens and that effects on the brain functions, such as memory and cognition, must be considered in relation to the decline of estrogens in women after natural or surgical menopause. I agree. I think it’s time we looked at the brain as connected to the body and affected by the same kinds of changes that affect other parts of the body. Psychological symptoms, like memory changes, clearly may have physical causes as well as stress-related causes.
ESTROGEN EFFECTS ON
MEMORY AND COGNITIVE PATHWAYS
• 17-beta estradiol, the primary estrogen produced by the ovary before menopause, has specific receptor binding sites in many different areas of the brain, and these receptor sites appear to be quite specific for the native human form of the molecule. (All of my clinical work with patients strongly supports these basic science findings in animal models.)
• Estradiol promotes growth of new dendrites between nerve cells, making more synaptic connections, while progesterone breaks down the nerve-cell connections. More synapse connections mean nerve cells can handle more incoming signals.
• When estradiol declines, synapse density in the hippocampus (memory and learning center) decreases as well. (My comment to readers: Denser synapses allow better cell-to-cell information flow.)
• Estradiol enhances nerve cells’ ability to take in nerve growth factor (NGF). In animals without ovaries, those who did not receive estrogen had a marked (56 percent) decline in the number of nerve cells; the animals given estrogen had only a slight decrease in nerve cells.
• Estrogens regulate cholinergic nerve cells in the basal forebrain of rodents. (My comment to readers: This is one of the regions of the brain involved in cognitive function and one of the areas that degenerates in humans with Alzheimer’s disease.)
• Estrogens increase the production of choline acetyltransferase, an enzyme needed to make acetylcholine (ACh). Estrogen thereby prevents the marked loss of ACh found in patients with Alzheimer’s. (My comments to readers: ACh is the brain’s most important chemical messenger for storing new memories in the brain, regulating memory retrieval, and cognition. Loss of the cholinergic nerves and chemical messengers is the most marked brain change in Alzheimer’s disease.)
© Elizabeth Lee Vliet, M.D., 2000
Listen to the comments of these women who experienced the benefits on memory that came from making appropriate changes in their estrogen therapy:
After a hysterectomy at age fifty-two, I took Premarin for nearly eight years. My memory began to deteriorate. Never one to be particularly concerned about getting old, I made fun of it at first. I reached a point, however, around age fifty-six when my memory loss was downright embarrassing. I felt I was in a mental fog. I couldn’t remember common words, stumbled through sentences, lost my train of thought, had difficulty following complex conversations or instructions, and even skipped words when I wrote. My work suffered and I could tell my family and friends were being kind and patient with me. Loving and generous of them, but humiliating for me. Dr. Vliet suggested I use Estrace for my hormone replacement therapy. In a short time, I began to notice I was no longer constantly apologizing for lapses in speech and memory. The fog had lifted. Of course, my memory isn’t what it was when I was twenty, but I have regained my pride and self-confidence. At last, I’m enjoying this stage of my life and all it has to offer.
—A.F., age 62.
I later received the following letter from this patient’s mother, who is in her eighties, after she had seen the improvement in her daughter from the change in type of estrogen:
I believe the first thing I noticed after changing from Premarin to Estrace was a cloud lifting from my skull [mind]. Prior to that I seemed to be going around in a perpetual fog, never feeling as though I was thinking clearly. That was such a relief! I seemed to remember things much more clearly, not stumbling over names that I had known for years, once again being able to reconcile my bank accounts and being able to reply to questions that had previously left me with complete blanks. One of the things that had bothered me a lot was the shaking of my hands. There were days when I could hardly make out checks and when I finished, they looked like some person with palsy had written them and were almost illegible. Physically, I feel 100 percent better, and I am so grateful to you for recommending the Estrace to my daughter so I could ask my own doctor to make the change for me.
—F.L., in her eighties
Don’t suffer in silence. Know that help is available, and there are a number of such changes in hormone therapy that can improve your memory, improve your clarity of thinking, and give more of that feeling of energy and zest if you are having these problems.
After about age forty, women have approximately five to eight times the incidence of thyroid disorders found in men of similar ages. We do not yet have a clear explanation for this gender difference. Diminished thyroid function becomes more frequent in women as they age, and must be included in the proper evaluation of women in the perimenopause and menopause years. One of the concerns is that brain symptoms of hypothyroidism such as memory loss, decreased concentration, difficulty organizing one’s thoughts, and depressed mood are often so subtle that many women are not properly diagnosed until the disorder has progressed to produce the more obvious physical signs of dry skin, hair loss, weight gain, cold intolerance, slowed heart rate, decreased reflexes, high blood pressure, and high cholesterol, to name a few. The subtle brain symptoms tend to occur first, and memory loss is among the early changes when thyroid hormones are not adequately produced, or when their effect is blocked by antibody production as occurs in Hashimoto’s thyroiditis. Since the changes found in thyroid disorders may overlap the symptoms women experience with menopause, it is particularly important that both hormonal systems be checked fully. If left untreated, hypothyroidism can progress to a dementia syndrome similar to Alzheimer’s disease. I have also had quite a few patients who had been misdiagnosed with Alzheimer’s dementia, but when proper tests were done were found to have a treatable hypothyroidism causing their memory impairment. The evaluation of thyroid function is significantly overlooked in women’s health, particularly as women get older.
Of course, it is important not to overtreat thyroid disease and take too much thyroid hormone, since excessive amounts of thyroid hormone can cause heart damage and bone loss. These complications occur whether you take “natural” thyroid extracts or the medications made by pharmaceutical companies. Excessive amounts of thyroid cause your body’s metabolic engines to be overly “revved up,” with increased heart rate, jitteriness, irritability, excessive weight loss, and increased bone breakdown. Thyroid imbalances, either too high or too low, can produce marked effects on brain function, with resulting mood, behavioral, and cognitive changes. Low thyroid causes memory loss, difficulty concentrating, slow mental processes like a “gray cloud of fog” has dropped down over your brain. Excess or “hyper” thyroid states cause scattered thinking, difficulty focusing, memory disruptions (similar to power surges affecting your computer circuits!), and other brain symptoms much like what we call attention deficit disorder. For optimal function of your brain, including memory, balance is the key with all of these critical hormones.
Tossing and turning, waking up wide-eyed, looking at the clock, going back to sleep, waking up, looking at the clock. This is a common scenario I hear from midlife women. As estrogen levels drop before a period, after ovulation, or decline with menopause, the drop in estradiol triggers a firing of the “alerting” centers in the brain. These centers then discharge a burst of an adrenaline-type chemical messenger, which has an arousing effect and wakes you up. In addition, the burst of adrenaline hits the brain’s heat-regulating center and triggers the hot flash or flush, followed by sweating. These episodes of awakening at night may occur only a few times or may be quite frequent, leaving you feeling tired when you get up in the morning. Sleep disruption over an extended period of time is associated with daytime drowsiness, fatigue, feeling “foggy” mentally, and also with disturbances in memory, concentration, focus, and even loss of libido. Prolonged sleep disruption can even be a cause of the biochemical changes that lead to a major (clinical) depressive episode. Getting a good night’s sleep is more crucial to our health than most women realize.
I had always been a good sleeper until I hit age thirty-nine. I thought I was much too young to even think about something like premature menopause. I couldn’t figure what in the world was happening to me. My doctors just thought it was the stress of medical practice (made sense to me, given how busy I was), and I acquiesced to that idea. A few years later, I realized, as many of my patients have also said, that I had been under a lot of stress at other times in my medical career and did not have the same problems sleeping. So what was this? It turned out that I was actually in premature ovarian decline. The loss of estrogen was causing the frequent waking episodes. Extensive sleep research in recent years has helped us understand the many beneficial functions of sleep to maintain normal body restoration and repair each twenty-four hour-cycle. The role of healthy sleep patterns in optimal memory function has not yet been fully defined, but researchers have identified a strong correlation between failing memory and abnormalities of the sleep cycle. Estrogen balance in women is important for regulation of both sleep and memory.
The normal sleep cycle and sleep stages are adversely affected in significant ways when women lose the active form of estrogen (17-beta estradiol), a process that begins long before you stop menstruating. I described in chapter 5 some of the current studies that have shown estrogen replacement results in improved sleep, even in women with severe forms of sleep disorders like sleep apnea syndrome. Of course, I recognize that there are many factors that cause disruption in sleep (see list), and these must also be addressed. But, the one factor frequently overlooked for women is the effect of estrogen change in triggering fragmented sleep. I think women should have their hormone levels properly tested in their medical workups before sleeping pills are prescribed.
SOME COMMON CAUSES OF INSOMNIA
• hormonal changes (ovary, thyroid, adrenal, pituitary, etc.)
• drug and alcohol abuse (acute effects and withdrawal), tobacco use
• excess caffeine, other stimulants (sodas, coffee, tea, chocolate, “metabolic” or “energy” boosters with phenylpropanolamine, herbs with ephedra, weight loss and herbal products that contain Gotu kola and other stimulants)
• medical disorders: examples are COPD, congestive heart failure, asthma, diabetes, fibromyalgia, sleep apnea, and many others
• medications: especially allergy and cold medicines with decongestants, some antidepressants, testosterone, or DHEA (if taken at night), many others
• jet lag, shift work that disrupts normal sleep-wake cycles
• clinical depression, generalized anxiety disorders
• life stress, persistent worries, bereavement, posttraumatic stress disorders
• poor sleep habits (making your bed a second home office doesn’t help you relax!)
© Elizabeth Lee Vliet, M.D., 1995
Sleep architecture is the term used to describe the normal pattern of sleep stages (shown in the table on facing page). Each of these is characterized by different electrical activity or “brain wave” patterns, measured on electroencephalogram (EEG) tracings, eye movement measures (EOM), and muscle activity (EMG). Non-REM sleep (NREM) are the four stages in which dreaming does not occur. REM sleep is the stage in which dreaming occurs, along with other physiological responses like penile erections in men. Sleep problems (apnea, narcolepsy, and others) can be evaluated in sleep laboratories to determine the specific type of disorder, which in turn directs the physician to the proper treatments.
As you sleep each night, you experience seventy- to one-hundred-minute cycles of these stages, with more NREM sleep in the first half of the night, and more REM (dreaming) sleep in the second half toward morning. Sleep quality decreases with age in all of us, even in healthy individuals. The presence of medical problems, obesity, alcohol use, and cigarette smoking may all contribute to even more rapid deterioration in quality of sleep and may disrupt the normal sleep stages. If you become sleep deprived, the brain actively directs restoring the normal sleep patterns by lengthening total sleep time and the amount of slow wave sleep on the first recovery night. On following recovery nights, there is an increase (rebound) of REM sleep to compensate for lost REM during sleep deprivation. REM rebound causes intense dreaming for several nights or longer.
One of the reasons sleeping pills become a problem with prolonged use is that they interrupt the normal sleep patterns and the balance of the various stages. Stopping sleeping pills abruptly after more than two weeks of use will typically cause REM rebound, making it harder to sleep normally. Eventually, sleeping pill use makes it harder for the body and brain to function normally and will further impair energy, mood, and memory independent of the specific medication’s effects on memory (more about this in the next section). This is another reason I do not like to see women have prescriptions for sleeping pills without looking carefully for the underlying causes of sleep problems, including hormone changes, and more serious kinds of sleep disorders (e.g., SAS), which could be dangerous in combination with sleeping pills.
For most women during the menopause transition, sleep disruption does not require sleeping pills. Restoring optimal estradiol balance, learning relaxation techniques, having a carbohydrate snack before bedtime to increase brain tryptophan, which will then boost serotonin production (skim milk and cereal is good), or a trial of herbal remedies such as St. John’s Wort or 5-hydroxytryptophan or valerian root may all help to restore normal sleep. There is a positive synergistic effect from using a combined approach with all of these options. I have some women who did not want to take a full therapeutic amount of estradiol who reported good results for sleep improvement with a lower dose combined with serotonin boosters. You should talk with your physician about these approaches to see what fits YOU best.
All of the sleeping pills on the market today, both prescription and over-the-counter ones, adversely affect your memory. The other “drug” that many people, particularly women, use to help them fall asleep is alcohol. It, too, impairs memory, along with its many other negative effects on health. Alcohol not only causes direct damage to nerve cells, but it also depletes your brain and body of crucial vitamins that are needed for the brain’s memory circuits to work properly. For example, the B vitamins are significantly depleted when you drink alcohol on a regular basis, and all of the B vitamins are needed for the brain to make its memory-regulating neurotransmitters. Each class of medication acts by different means to decrease memory, but all of them contribute to memory loss over time. Fortunately, much of the memory loss produced by alcohol, sedative sleeping pills, and over-the-counter sleeping pills can be reversed if you stop using these substances. After prolonged overuse of alcohol, however, the nerve cells are permanently damaged, and memory loss does not return when a person stops drinking. The progression of further memory loss may be stopped by eliminating alcohol, but once tissue damage has occurred, normal memory function does not return. This is another reason to limit alcohol to occasional, moderate intake. Let’s look at what happens to the brain with each of these “memory robbers” to help you understand why memory changes occur.
These are generally grouped under the term sedative-hypnotic medications and include (1) the older barbiturates (Meprobamate, Seconal, and others), which are not used as much today due to their toxicity and addictiveness; and (2) the benzodiazepine group (Ambien, Dalmane, Restoril, Halcion, Doral, ProSom; other benzodiazepines that are sometimes used for sleep include Klonopin, Valium, Libruim, Xanax, Ativan, or Tranxene). All of the drugs in this category will initially improve sleep by inducing more rapid sleep onset and helping to maintain sleep. After about ten days to two weeks, these medications lose their effectiveness on sleep and also cause a disruption in the normal stages of sleep (mainly loss of stage 4 sleep). The sedative-hypnotics as a group all cause memory loss if used for an extended period of time, usually longer than two weeks. For some people, the memory impairment can come much more quickly than that. These drugs typically also cause a hangover effect of daytime “brain fog,” feelings of tiredness or excessive fatigue, and daytime drowsiness; this problem will be worse with long-acting ones (Klonopin, Dalmane, Valium, Librium) and less noticeable with shorter-acting ones such as Ativan, Ambien and Xanax.
The high potency, very short-acting sleep medications, such as Halcion, produce much more memory impairment the next day and also tend to cause rebound anxiety when the drug wears off. I was concerned about the very short action of Halcion and its high potency; even when it first came out, I rarely prescribed it. With the subsequent publicity about the potential adverse reactions, I do not prescribe Halcion at all. I have personally treated many women who have had severe mood changes (anxiety, irritability, memory impairment, and other problems) from Halcion, and I do not recommend its use. The benzodiazepines have an additive effect on sedation and potential respiratory depression if you drink alcohol when taking them. All of the drugs in this category produce dependence and cause withdrawal syndromes if stopped abruptly after more than about seven days of use. It can also be dangerous to use sedative-hypnotics if you have sleep apnea, since these medications further suppress respiration. It is uncommon for me to prescribe sedative-hypnotic medications. I much prefer to first see that the sleep problem is properly diagnosed and then to help the individual develop good sleep habits, use nutritional and other natural methods of improving sleep, consider hormonal options if appropriate and desired, and as a last resort use lowdose serotonin-augmenting medications.
Older sedating antidepressants that boost serotonin, such as Desyrel (trazodone), Elavil (amitriptyline), Sinequan (doxepin), Tofranil (imipramine), as well as newer medications like Zoloft, are often useful in very low doses to help with insomnia. These medications are not addictive, do not disrupt the normal stages of sleep, and if used in low doses, have fewer side effects than typically encountered in the higher doses used to treat depression. These all have mild to moderate antihistamine effects, enhance serotonin activity, and produce drowsiness at low doses. At higher doses used for treating depression, they decrease nocturnal awakenings, increase non-REM sleep, decrease REM sleep, and normalize the disturbed sleep that is characteristic of biological depression.
I think these medications are safe and potentially helpful, but some of the side effects of all except trazodone are particularly bothersome to midlife women (weight gain, dry eyes, constipation, among others), and these medications also have potential for many drug interactions with other medications you are taking. You will need to discuss these options with your physician and see if they might be appropriate for you. The serotonin-boosting antidepressants are especially valuable in improving sleep in people with perimenopausal hormone changes and chronic pain syndromes. You may want to read more in the chapter on fibromyalgia about how these drugs work to reduce pain. The antidepressants are nonaddictive, but if stopped abruptly, you may experience “REM rebound,” which results in several days to a week of intense dreaming, irritability, and mood swings. If you are taking these medications, even in a low dose, it is best to taper them off gradually.
Another natural serotonin booster is 5-HTP (5-hydroxytryptophan), a building-block molecule used by the brain to make serotonin. Although 5-HTP is widely available without a prescription, there have been FDA reports of contamination in these products similar to that seen with L-tryptophan a number of years ago. As a result of these concerns, I do not recommend that you use an over-the-counter product of 5-HTP. I recommend getting a pharmaceutical-grade form of 5-HTP from a compounding pharmacist you trust. The one we use is Belmar Pharmacy in Lakewood, Colorado (800-525-9473), and we have found that their prices for the prescription pharmaceutical grade 5-HTP are lower than many of the over-the-counter products.
These include non-prescription products such as Sleep-Eze, Nytol, Sominex, and a variety of others. These products typically contain antihistamine compounds (diphenhydramine is a common one) that are central nervous system depressants and produce drowsiness and sedation. Daytime sleepiness and difficulty with memory and concentration is common. Weight gain and cravings for carbohydrates are other common side effects of antihistamines. You should let your physician know if you use these OTC sleep aids, because they all can potentially interact with other medications you may be taking. This group has an additive effect on sedation if you also drink alcohol. I have also found that many of my patients have the opposite reaction to antihistamines and become anxious and agitated rather than sleepy. Be cautious if you use these sleep aids, communicate with your physician and do not use them for an extended period of time without having your sleep problems fully evaluated medically.
There are many herbal remedies that have been used to promote sleep. Some of these include valerian root, lemon balm, chamomile, and passionflower. These can be helpful for some people but may trigger allergic reactions in sensitive individuals. If you would like to use these approaches on a short-term basis, I suggest you consult with a knowledgeable herbalist rather than just taking the advice of a salesperson in a health food store. If you are someone with a lot of allergies to trees, grasses, and other plants, remember that these herbal remedies are derived from plants and have the potential to aggravate allergies. It is surprising to me how many people usually do not associate their allergies to plants with the possibility of a reaction to an herbal product.
A number of vitamins are crucial cofactors, or “helpers,” for the brain to make important chemical messengers involved in normal memory function. Several of these, especially B12 and folate, have been known for decades to play a role in maintaining normal brain function, in particular memory and mood regulation. More recently, research in a number of countries had continued to identify the role of various vitamins and minerals in memory processes. Iris Bell, M.D., Ph.D., at the University of Arizona, has significant research documenting the effects of vitamins B1, B2, and B6 in improving both depressive symptoms and cognitive function in elderly patients. Dr. Bell has found that thiamine (B1) deficiency impairs brain glucose metabolism and also contributes to high levels of homocysteine, a risk factor for cardiovascular and cerebrovascular disease that can then lead to memory loss. It appears from a number of studies that significant numbers of patients may have laboratory values of these B vitamins that appear to be in the “normal” range, but may not be adequate for optimal nerve cell function in the brain.
Another area of research into factors affecting memory is the role of antioxidant vitamins in prevention of plaque formation in arteries, thereby improving blood flow to the brain. Oxidation, or “free-radical damage,” is the process of cell damage and death associated with aging, environmental pollutants, poor nutrition, tobacco smoke, radiation, and other causes. What are free radicals? These are “crippled” oxygen atoms that have lost electrons in the chemical reactions of our body’s natural metabolic processes, or as a result of trying to make up for poor nutrition, environmental pollution, and other causes. These free radicals roam the body trying to replace their lost electrons by combining with electrons from healthy cells. This causes damage to the membranes and structures inside healthy cells, much like rust damage to your car. What are antioxidants? These are molecules, such as vitamins E, C, beta-carotene, and selenium (estradiol has also been found to act as an antioxidant), which have the capability of losing electrons to free radicals without initiating a damaging chain reaction of electron robbing. Antioxidants serve as “scavengers” to clean up these damaging free radicals and help prevent some of the damage to DNA and cell death. Brain neurons and nerve fibers are particularly vulnerable to damage and death from these free radicals. The antioxidants reduce much of this oxidative damage and help keep brain cells working properly. The effect is to produce modest improvements in memory. Antioxidants, as I will describe in chapter 14, also play a role in helping decrease the risk of certain cancers.
Unfortunately, as most of you now know, nutrition has only received brief mention in most medical school curricula. The critical role of vitamins and minerals in brain function is rarely addressed as an important clinical issue. Consequently, most physicians think that a balanced diet is enough and hardly anyone needs vitamin supplements. I must admit that this was my notion, too, when I first started medical practice. Over the years, with more collaborative work with dietitians interested in preventive medicine, and my own study of nutritional factors affecting mood, energy, memory, and a host of other problems, I have come to clearly see that probably most of us would benefit from vitamin supplements. That’s quite a turnaround from where I was when I graduated from medical school. I am now diligent about taking my own vitamin-mineral supplements daily.
Very few Americans really eat a balanced diet to begin with, and even fewer women have enough caloric intake and food variety on a daily basis to provide even the RDA for many vitamins and minerals. A classic example is magnesium. The average American woman has a daily intake of about 100 mg. The RDA is 400–600 mg a day. Magnesium is critical for nerve and muscle function, mood and memory processes, and bone development among many other roles in the body. Several years ago, I was struck by a nutritional study done by Angelica Cantlon, R.D. She calculated the amount of calories and variety of food that would be required for the average woman to get her RDA of all the basic vitamins and minerals. She found that daily calories needed to be 1400, and the food groups needed were far more diverse than any patient’s food diary I have seen in my entire career in medicine! I was shocked, and so were the women in my seminars when I showed them the results of this study. An average woman who is chronically dieting to lose weight, and this is certainly more common in the premenopausal years when everyone seems obsessed with losing weight, has a daily calorie intake of 800 to 1000 calories, followed by marked increases on the weekends at social functions! No wonder there seem to be more memory problems in midlife: not only are important estrogen levels changing, but also women are not eating well enough to sustain the brain’s activity at optimal function. Fueling the brain with healthy, quality “fuel” is the best way to have sharper memory.
Start with a basic healthy meal plan, but consider that a good multivitamin with additional calcium, magnesium, beta-carotene, and vitamin E and vitamin C will give you added antioxidant insurance. Magnesium and vitamin E in particular are both difficult to obtain in the typical American diet in order to give you the full antioxidant dose. For best absorption, try a liquid formula of the multivitamin you select. Centrum is a good one that is available in major drugstores and not very expensive. I don’t endorse megavitamin supplements, since I think these are frequently more expensive than necessary and I have seen many of my patients end up having significant side effects and subtle toxicity syndromes.
A variety of these products are being promoted as “brain enhancers.” I continue to be surprised at the amount of money patients spend on these supplements and how many they typically take. It is difficult to make any comments about the effectiveness of these products, since it is often difficult to know exactly what is in the product, and there so far is not a great deal of sound research to document positive results with their use. Deprenyl (selegiline) is one drug in this group that has been shown to be of help in reducing the nerve deterioration characteristic of Parkinson’s disease. It has been used in Europe as an antiaging drug and a memory enhancer. I have had a few patients who have been on it for preventing the progression of Parkinson symptoms, but I have not seen dramatic changes in memory or other of its purported actions. It has the potential to cause high blood pressure reactions when taken along with the amino acids tyrosine and phenylalanine, as well as tyramine in certain foods. Since these amino acids are also found in foods, persons on Deprenyl have to watch dietary sources as well as supplements. I do not encourage its use simply as a cognitive enhancer, but if you take it, I urge you to notify your physician. I have worked with a number of women experiencing anxiety symptoms, only to find out later that they were taking ephedra supplements or Deprenyl, and these were causing the anxiety problems. Please be sure to talk with all of your health care professionals about everything you take, even if it is an over-the-counter, nonprescription product.
A promising new Alzheimer’s drug called galantamine (Reminyl) was recently approved in Sweden and is being evaluated for approval in the United States and several other European countries. Galantamine preserves the memory-enhancing neurotransmitter, acetylcholine, in the brain by blocking the enzyme, acetyl-cholinesterase, that breaks it down to inactive forms. Increasing the levels of acetylcholine in the brain is thought to lessen the memory loss, cognitive decline, and functional impairments that occur in Alzheimer’s disease.
Emerging work on the plant extract, Gingko biloba (GBE), is showing promising results to improve brain blood flow, memory, and cognition. Researchers at the Department of Geriatric Medicine at Whittington Hospital in London studied the effects of Gingko biloba on thirty-one elderly patients with mild-to-moderate memory impairment and found a statistically significant beneficial effect over placebo. Their study is significant in that it was a double-blind, placebo-controlled protocol over six months, and also included EEG brain wave results. In another European study, seventy-one outpatients with cerebral insufficiency at three test centers were randomized into a double-blind, placebo-controlled protocol for twenty-four weeks. Statistically significant improvements in short-term memory and learning rate were found in the patients taking the gingko extract (EGb 761) but not in the placebo group.
European research over the past thirty years suggests that Gingko biloba extract acts as a vasodilator, improves oxygen and glucose uptake, and also acts to help decrease platelet clumping (a factor in arterial plaque formation). At present, there is no regulation of gingko products, and they are proliferating rapidly (along with rising prices) as word spreads about these research findings. Most of the studies have been done on the original extract, EGb 761, and this is the brand Ginkold. Other brands may or may not contain the same percentage and compositions of the active compounds. If you chose to try GBE, look for a brand that is approved by the German Commission E, a regulatory body that oversees the quality control for herbal products sold in Germany. Brands that carry this approval generally contain the amount of standardized extracts that were shown in the clinical studies to be effective. Also I encourage you to use some common sense, and observe your body responses before you buy a year’s supply.
I do not have the space to go into all the other “smart drugs” currently being touted as wonder agents to prevent changes in brain function with aging. If you are interested in this subject, I encourage you to seek sound information and discuss it with your physician before adding numerous supplements to your daily routine. The best memory enhancers are still the basics I have discussed in this chapter, with particular attention to eliminating alcohol, tobacco, and fatty foods along with taking your vitamins, exercising regularly, and paying attention to optimal hormone balance.
Think of your brain as a “mental muscle” and exercise it. Research has shown that stimulating your brain with new learning actually helps increase the number of neuron connections. Take a class in an entirely different field, learn a foreign language, do crossword puzzles, practice solving brainteasers. When you want to remember something new, focus on it, repeat it several times, and perhaps write it down and look at it as well.
Some simple principles of paying attention to basic health habits also improve brain function and memory. These are summarized in the chart that follows.
DR. VLIET’S MEMORY-ENHANCING STRATEGIES
• Stop smoking (it deprives your brain of oxygen).
• Stop or reduce use of sleeping pills (talk with your doctor about how to do this safely, since these medications must usually be decreased gradually).
• Eat smaller meals at regular intervals for steady “fuel” to the brain
• Make sure you have healthy nutrition and balance of protein, fat, and carbohydrates.
• Have your thyroid, ovarian, and adrenal hormone levels checked, and consider hormone therapy if your levels are too low and your memory is fading.
• Reduce fat in your diet. It contributes to plaque deposits in the arteries and blocks blood flow to the brain.
• Exercise aerobically several times a week. Doesn’t have to be fancy—brisk walking is fine!
• Take a good basic multivitamin along with antioxidants like vitamin C, vitamin E, selenium.
• Eliminate or reduce alcohol.
• Practice relaxation exercises or meditation.
• Get enough sleep.
• USE IT OR LOSE IT—Stimulate your brain with new ideas, and practice!
© Elizabeth Lee Vliet, M.D., 1995, revised 2000