A 9-year-old boy was on the ketogenic diet since age 5 for his intractable absence type seizures. However, he had significant behavior problems, which the diet was helping, but it still became difficult to keep him on the diet. In August 2001, on her own, his mother switched him to the Atkins diet. His seizures remained under control with less episodes of cheating. Seizures worsened when his mother added carbohydrates, so our natural impulse was to put him back on the stricter ketogenic diet. After 2 more years of dealing with food battles, his mother switched him back for the second time to the Atkins diet, which he remains on still to some degree today, now 10 years in ketosis.
In March 2003, a young 7-year-old girl was 1 month away from her scheduled week-long admission for the ketogenic diet. Her seizures were occurring 70–80 times per day, and she had failed 8 anticonvulsants. In preparation for the ketogenic diet, we suggested a gradual reduction of high-carbohydrate items, such as bread, pizza, cake, and breakfast cereal in order to get the child used to the foods that would be given. Her mother asked for more information to help reduce carbohydrates, so we suggested buying Dr. Atkins’ New Diet Revolution and reading about the induction phase. That was Friday; by Monday her seizures had totally stopped.
Needless to say, we were shocked. When we saw her in clinic later that week, her urine ketones were large. Our dietitian calculated she was receiving about 10 grams per day of carbohydrates, which we recommended she continue. We also started a multivitamin and calcium and began to check cholesterol periodically. After 1 month of seizure freedom, we cancelled her admission for the diet. She remained on the modified Atkins diet for about 4 years before seizures returned and she eventually stopped it to pursue epilepsy surgery (which did eventually lead to seizure freedom).
After these first two children, others were tried on a modified Atkins diet of 10 grams/day of carbohydrates. Details of these children and some adults can be found in the next chapter. Although the induction phase of the Atkins diet allows 20 grams/day of carbohydrates, our dietitian believed that the ketogenic diet generally allows 5–10 grams/day, and therefore 10 grams/day was a more appropriate starting point for children. She felt the Atkins diet was likely approximating a 1.5:1–2:1 ratio.
Since the Atkins diet creation in the 1970s, families that were told to start the ketogenic diet often asked “Is this the Atkins diet?” Our typical answer was “Of course not!” Although we were quick to point out the many differences, there were just as many similarities.
The Atkins diet was created in the 1970s by the late Dr. Robert C. Atkins as a means to combat obesity. It has become very popular since the year 2000, as a result of several high-profile articles in the New England Journal of Medicine, the clear failure of the obesity epidemic to improve with the “accepted” low-fat diet, and the widespread availability of pre-packaged low carbohydrate snacks and meals in stores and restaurants. Similar to the ketogenic diet, it encourages fat intake and restricts carbohydrates. Foods on the Atkins diet are very similar to what is eaten on the ketogenic diet. Both diets can induce weight loss, although with the Atkins diet, it’s the major goal compared to the ketogenic diet! For many years the medical community described both diets as voodoo medicine, unsafe, unlikely to work, and dangerous … but has recently changed their minds.
TYPICAL 2 DAYS OF FOOD FOR A CHILD ON 10 G/DAY MODIFIED ATKINS DIET
Day 1
Breakfast
Scrambled eggs
Bacon (2 strips)
36% heavy whipping cream diluted with water to make milk
Lunch
Bologna/ham, lettuce, Dijon mayonnaise “roll-ups”
Raspberries (1/2 cup)
Cucumber slices (1/2 cup)
Flavored, calorie-free, sparkling water
Snack
Just the Cheese™ (crunchy) snacks
Dinner
Hot dog
Spaghetti squash with butter and salt (1/4 cup)
Sugar-free flavored Jell-O™ topped with whipped heavy cream
Day 2
Breakfast
Sausage links
Low carbohydrate yogurt
Water
Lunch
Cheeseburger (no bun)
Cole slaw
Heavy whipping cream, water, and unsweetened cocoa powder
Snack
5 macadamia nuts
Mozzarella cheese stick
Dinner
Sliced chicken, coated in egg and CarbSense™ baking mix then fried in olive oil
Steamed, mashed cauliflower with salt, butter, and pepper (mashed
“potatoes”)
1/2 cup of strawberries topped with heavy whipping cream
The big similarity between the two diets: ketosis. Throughout the book Dr. Atkins’ New Diet Revolution, there are references to using urine ketone strips to monitor ketosis as a sign of burning fat and weight loss. In fact, in the “induction phase” of the Atkins diet, 20 grams/day of carbohydrates is advertised as leading to a ketotic state, but above that would not. The high levels of ketosis, although surprising to us, turned out to be no surprise to the Atkins Foundation. When contacted, they were extremely friendly and helpful with information.
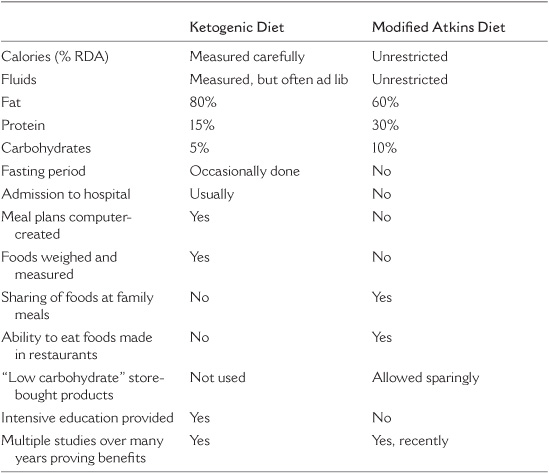
Yes. There are many important differences between the modified Atkins diet and the ketogenic diet. They are listed in Table 18.1. It has less fat and more protein and carbohydrates, but still it’s different than the standard diet. The modified Atkins diet does not restrict protein or calories and can be started without a fast or hospital admission. Certainly some centers do not fast or admit their children, but the modified Atkins diet can be started quickly in the clinic with limited teaching and dietitian support. It usually takes our center about an hour to teach a family how to do it. Unlike the ketogenic diet, pre-made products such as baking mixes, candy bars, and shakes are available in many groceries and restaurants. It allows a child to choose items off a menu at a school cafeteria or restaurant, which is nearly impossible on the ketogenic diet. Families can buy Dr. Atkins’ New Diet Revolution or a carbohydrate gram counter (e.g., CalorieKing guides) in almost any bookstore or online nowadays and begin the diet at home. Although less restrictive, there is less dietitian support, so families need to be more independent. Constipation, acidosis, and weight loss seem to be less common, but the two diets have never been studied against each other prospectively to compare. Lastly, parents can do the Atkins diet themselves, along with their child. Even your doctor can do it!
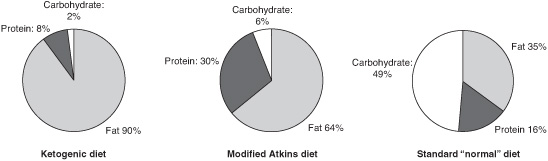
FIGURE 18.1
Compositions of ketogenic, modified Atkins, and standard diets.
Other than perhaps the MCT oil diet and availability of Nutricia KetoCal®, the ketogenic diet in use today is remarkably similar to that created 80 years ago.
Do we need something new? Maybe.
We have found the modified Atkins diet to be helpful for children with significant behavioral problems in which the ketogenic diet’s restrictiveness would cause problems. Not all epilepsy centers in the world offer the ketogenic diet, as it requires a specially trained dietitian and medical team; the Atkins diet may be a partial solution. Some children have had difficulty with high cholesterol and poor growth; this may be less of an issue with a lower ratio (and higher protein) diet. Adolescents and adults, commonly discouraged from trying the ketogenic diet (whether this is right or wrong!), might be the ideal candidates for the modified Atkins diet. Lastly, if it is truly easier to start and stick to, maybe the modified Atkins diet could be used early in the course of seizures, in some cases before medications?
TABLE 18.1
Differences Between the Ketogenic Diet and the Modified Atkins Diet
The modified Atkins diet is now over 8 years old. It works in 49% of children (and adults) who start it. Over 200 patients have been started just in the medical literature, with likely double that number who haven’t been published in any trial. The percentage of patients who it works for is strikingly similar to the ketogenic diet. However, they have never been formally compared in the same study with large numbers as a randomized trial. Although this has been discussed, we are not sure it would sway parents or physicians to use one diet over another no matter what the results were. We see these diets as complementary and not competing.
At Johns Hopkins, we generally advocate the ketogenic diet but are willing to use the modified Atkins diet for local patients who need a diet quickly or clearly do not want the ketogenic diet for various reasons. We use it for teenagers and adults. In our Adult Epilepsy Diet Center, the modified Atkins diet is the diet of choice. Many of our long-term patients on the ketogenic diet for over 10 years are being switched over. For young babies and children, however, we lean toward the ketogenic diet due to both the easy availability of ketogenic diet formulas and the need for more careful monitoring in this age.
Work is underway to get this diet to developing countries in which there is limited dietitian support. Projects are underway in Honduras and parts of China and India. We have discussed its use for emergency outpatient situations (e.g., Doose syndrome with drop seizures) where children should not wait 1–2 months to start the ketogenic diet. As neurologists and oncologists look at dietary treatments for nonepilepsy uses, the modified Atkins diet may be a more reasonable option for potentially years of use than the ketogenic diet if the condition is not perceived to be as serious as epilepsy (e.g., migraines).