Electromagnetic field exposure is so prevalent that the possibility of even a modest increase in disease incidence from this source is worthy of attention.
—David Savitz et al., 1988
In considering the plausibility of biological effects of electromagnetic fields, such an evaluation must depend on quantitative measures of the agent. Only homeopaths will dispute that there must be some level of field strength that cannot possibly affect biology.
—Robert Adair, 1998
With the growth of electrification starting in the late nineteenth century and continuing throughout the twentieth, exposure to weak extremely low frequency electromagnetic fields from man-made sources, unknown until slightly more than a century ago, has become virtually ubiquitous in the United States and other technologically advanced societies. As a result, we are constantly exposed to these fields from the electrical power distribution system, the wiring in our homes and workplaces, household appliances, and industrial and office equipment. It is worth noting that, although we live our daily lives in an intimate relationship with electric power, we are rarely aware of it, except when a major breakdown of the electrical power grid occurs, as happened, most recently, on August 14, 2003, in the eastern United States.
There had been early reports from Soviet scientists in the 1960s of adverse symptoms in workers exposed to very high electric fields, and in the mid-1970s the U.S. government and the electric power industry set up research programs to study the biological effects of electromagnetic fields.1 However, the idea that exposure to the extremely low frequency electromagnetic fields emanating from power lines and other sources might cause cancer or other serious disease did not become a focus of societal concern until 1979, when a paper entitled “Electrical wiring configurations and childhood cancer” by Nancy Wertheimer and Edward Leeper came out in the American Journal of Epidemiology.2 The reasons for this lack of concern are straightforward. Extremely low frequency electromagnetic radiation is at the low end of the electromagnetic spectrum (fig. 4.1). The energy of electromagnetic radiation is characterized by its wavelength (e.g., in centimeters) or, equivalently, by its frequency (e.g., Hertz, or Hz) because energy (E) = Planck’s constant X frequency, and frequency X wavelength = speed of light. Thus, the energy of electromagnetic radiation is directly proportional to its frequency and inversely proportional to its wavelength. The lower the frequency, the lower the energy and the less it can affect the cells in our bodies. Ionizing radiation, including gamma radiation, X-rays, and ultraviolet radiation, has extremely high energies that can damage the DNA of living organisms and have other effects on cells. Fields in the microwave range, with very much larger wavelengths (several inches), have enough energy to cause heating in conducting material. Extremely low frequency electromagnetic radiation, with frequencies below 3,000 Hz and with wavelengths of more than 5,000 km, has extremely small energies, which cannot cause heating or ionization. Furthermore, the extremely low frequency electromagnetic fields encountered in everyday life are weaker than the Earth’s magnetic field. Finally, the strength of electromagnetic fields decreases rapidly with increasing distance from the source, thus further diminishing the fields to which humans are exposed.
In spite of the inherent implausibility of adverse human health effects stemming from exposure to extremely low frequency electromagnetic fields, the publication of the Wertheimer and Leeper study and subsequent studies throughout the 1980s were seized on by the media and by regulatory bodies, such as the World Health Organization and the U.S. Environmental Protection Agency, as evidence of a potential health hazard. The fact that the fields produced by electric current at 60 Hz (50 Hz outside North America) were both invisible and ubiquitous, that exposure was largely beyond one’s control, and that the alleged health consequences were depicted as catastrophic helps to account for the intense fear that came to be associated with this question in the public mind.
The story of how EMF (for the sake of convenience, I will use the terms “electromagnetic fields, “EMF,” “extremely low frequency electromagnetic fields,” “ELF-EMF,” and “power-frequency electromagnetic fields” interchangeably) from power lines and other sources came to be seen as a serious threat to the nation’s health sheds light on the way in which preliminary scientific findings can be isolated from their appropriate context, overinterpreted, and given wide currency. In this case, epidemiology by merely following its own internal logic and by generating inconclusive but suggestive results contributed to the creation of an apparent hazard, which was then acted on by society as if it were a real hazard. The social costs resulting from this perceived hazard have been substantial, including not only monetary costs to utilities and the public in the tens of billions of dollars3—from the relocating power lines and the abandonment of properties—but widespread and needless anxiety on the part of property owners and parents.
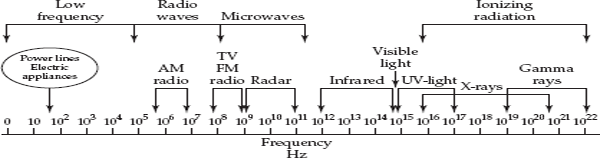
FIGURE 4.1 The electromagnetic spectrum. Adapted from Savitz and Ahlbom, 2006.
The enormous public attention that came to be focused on the question of potential health effects from exposure to power-frequency electromagnetic fields created a long-running drama involving many different players: the electric utilities and their research arm [the Electric Power Research Institute (EPRI)], epidemiologists, physicists, biophysicists, risk assessors and regulators, lawyers, print and television journalists, and the public. Members of these different parties had very different perspectives and stakes in the issue and, to a large extent, could not understand each others’ language or assumptions. For this reason, each party saw in the EMF problem what it was disposed to see by its training and narrow objectives. Thus, statements regarding EMF could rarely be taken at face value but, rather, needed to be interpreted in the context of who was making them.
One major axis in the drama was the conflict between concerned property owners and businesses on the one hand and the powerful electric utilities on the other. Owing to its enormous financial resources and political clout, the industry’s attempts to discredit early reports of adverse effects from power lines helped to create the impression of a cover-up. Another major axis entails the very different views of the issue held by scientists engaged in research on electromagnetic fields and scientists who were “outsiders” to this field of research and had no particular stake in the issue. This latter group comprised both physicists and a small number of epidemiologists who questioned how much weight should be given to epidemiologic studies of a weak and difficult to measure exposure. Accomplished academic scientists testified on behalf of the utilities—in one case six Nobel laureates (two in medicine) and nine other scientists signed an Amici Curiae to the Supreme Court of California to the effect that weak electromagnetic fields were unlikely to harm health—while other scientists, including prominent epidemiologists, testified on behalf of plaintiffs in suits attempting to block the construction of new transmission lines near communities.
Another symptom of how problematic and contentious this issue was is that the U.S. Environmental Protection Agency’s 1990 risk assessment report on power-frequency EMF, which determined that EMF was a possible carcinogen, was never released, apparently due to harsh criticism not only from industry but also from independent scientists. Furthermore, shortly after an expert panel concluded in 1992 that power-frequency electromagnetic fields were not a research priority, the U.S. Department of Energy and the National Institute of Environmental Health Sciences launched a special program devoted to basic research and risk assessment in the area of EMF. In this climate, marked by intense public concern, high stakes for a major industry, strong disagreements among scientists, and keen regulatory interest, each new report, regardless of its specific findings or its validity, served to reinforce the perception of a hazard.
Among the scientific disciplines addressing the EMF issue, epidemiology was the lynchpin in the emergence of EMF as a high-profile problem, and it has continued to play a pivotal role. For this reason, in the examination that follows, epidemiology occupies a central position, since the other disciplines and institutions responded—in specific ways and at key junctures and according to their own perspectives—to the epidemiology.
Before considering the epidemiologic studies, a few basics about EMF and units of measurement are in order. Electric and magnetic fields differ in important ways. With respect to possible health effects, most important is the fact that electric fields are easily shielded or weakened by various conducting materials, such as buildings, trees, and even human skin, whereas magnetic fields are not. For this reason, most research into health effects of EMF has focused on magnetic fields.
Exposure to magnetic fields is expressed in terms of milligauss or microtesla: 1 mG = 0.1 µT. For reference, 1 T is the strength of a typical magnet used in a medical MRI scan. There are 10,000 G in a tesla, and 1,000 mG in 1 G. Thus, the field strength of an MRI magnet is 106 mG. In contrast, ambient magnetic field exposures recorded in epidemiologic studies are in the range of hundredths of a milligauss to 10 mG.
THE INITIAL STUDY: WERTHEIMER AND LEEPER
In the mid-1970s, Nancy Wertheimer, a researcher at the University of Colorado in Denver, with a Ph.D. in psychology, became interested in studying the causes of childhood leukemia. Scientists had long suspected that an infectious agent might play a role in the disease, and this led Wertheimer to visit the neighborhoods of children who had developed leukemia in order to study sociodemographic factors and particularly overcrowding. In the course of exploring different neighborhoods, she made the observation that the homes of children who had contracted leukemia appeared to be located closer to electric power lines and substations than the homes of healthy children. With the help of a physicist, Ed Leeper, Wertheimer developed a novel method of estimating residential exposure to electromagnetic fields by characterizing the power lines in proximity to the homes. They distinguished between four exposure levels on the assumption that the greater the distance from the power lines and the thinner the wire, the lower the current flowing through it, and hence the weaker the resulting field. Using this method, Wertheimer and Leeper identified 344 deaths occurring in cases of childhood cancer diagnosed between 1950 and 1973 in the greater Denver area and compared the wiring configuration—or “wire codes”—of the homes occupied by their families with those of the homes of 344 healthy children.
What their data showed was that the homes of children who had developed cancer were between two and three times more likely than the homes of healthy children to have wire configurations suggestive of high-current flow. This was true whether they restricted the analysis to cases and controls who had lived in a single home or in more than one home, and the results appeared to hold independent of potential confounding factors such as urban-suburban differences, socioeconomic class, birth order, sex, and traffic density. The association was seen when different types of cancer were considered individually (leukemia, lymphoma, central nervous system tumors, and “other”) (table 4.1). Perhaps most intriguing was the existence of a dose-response relationship when exposure was categorized into four levels ranging from very high to very low.
However, a number of serious problems in the Wertheimer and Leeper study were apparent from the outset and were noted by the authors as well as by other researchers. First, the fact that wire coding was not done in a blind fashion—that is, with the technician performing the mapping of the wire configuration without knowledge of whether a given home was that of a case or a control—could have led to a biased assessment of exposure. Second, as the authors acknowledged, wire codes provide only a “remote proxy” for the actual fields due to power lines, which they were not able to measure. Furthermore, wire codes do not take into account fields due to electrical appliances, ground currents in the home, or other sources outside the home. A third problem was the possibility of selection bias due to differences between cases and controls. If controls are selected in a different manner from cases and represent a different underlying population, this could produce a spurious result. The method of control selection used by Wertheimer and Leeper was so complicated that it was difficult to assess its validity. Finally, the finding that wire codes appeared to be equally associated with different types of cancer in children raises a question since there is no known exposure that elevates the risk of all cancers. As can be seen in table 4.1, when stratified by type of cancer and wire configuration level, the number of cancer cases in each cell were quite small.
In their brief discussion, Wertheimer and Leeper discussed a number of explanations for their findings. They noted that the extremely low frequency electromagnetic fields created by power lines are extremely weak and that there was no evidence suggesting that they could cause cancer. They appropriately acknowledged that the association observed in their data was modest, on the order of a two-to threefold increase in risk. Wertheimer and Leeper also correctly observed that the lack of specificity with a particular form of childhood cancer militated against a causal relationship, unless EMF acted in such a way as to promote the growth of tumors generally. Yet, in spite of the implausibility of their results and the lack of any supporting evidence, they offered an exceedingly vague rationale for how ELF-EMF might affect physiology:
TABLE 4.1 Wire Configurations and Type of Cancer, Colorado, 1976–1977
HCC, high current confi guration; LCC, low-current configuration.
Source: Wertheimer and Leeper, 1979.
AC magnetic fields might affect the development of cancer indirectly, through some effect on physiologic processes. It is conceivable, for instance, that contact-inhibition of cellular growth, or the basic immune reaction of recognizing ‘self’ from ‘not self,’ involves electrical potentials occurring at cell surfaces. Against an electromagnetic background different from that provided during evolution, any such cell mechanism might be altered.4
Since virtually nothing is known about what causes leukemia or other cancers in children, the possibility that neighborhood power lines and substations played a role was of potentially enormous public health as well as medical significance. The fact that the paper was published in the respected American Journal of Epidemiology lent it credibility and caught the attention of epidemiologists interested in the causes of cancer and in preventable hazards in the environment. But many questions are studied by scientists that never gain any notoriety with the public. The potential threat from electric power struck a nerve in a society with a greatly heightened consciousness of pollution from coal-burning power plants and fears about the safety of nuclear power. In this atmosphere, the notion that electrical current from power lines extending from these plants and reaching into every neighborhood could pose a threat made a kind of intuitive sense. It is noteworthy that when scientists were interviewed in connection with news reports of new findings concerning the health effects of EMF, the producers invariably used an image of ominous-looking high-voltage transmission lines as a backdrop.
Given the serious methodological questions about the Wertheimer and Leeper paper, it is surprising that it received relatively little critical comment in letters to the American Journal of Epidemiology. Without much critical discussion, this single paper provided the stimulus for all subsequent epidemiologic studies of EMF and cancer, as well as regulatory interest in EMF. Over the ensuing twenty-five years, a large number of studies were published addressing the issue in a variety of ways, using different types of data, and looking at different disease endpoints. In the early phase of epidemiologic research, the focus was on “hematopoetic cancers” (mainly leukemia but also lymphoma) and central nervous system tumors because Wertheimer and Leeper had found excesses for these cancers in children. These diseases, in adults as well as in children, continued to be a focus of research, while the field widened to include other diseases. Early responses to Wertheimer and Leeper’s report included analyses of occupational data, some of which suggested that workers with presumed high exposure to EMF had elevated rates of leukemia and brain tumors. (It should be noted, however, that the predominant type of leukemia occurring in adults is different from that in children.) Then, in the early 1990s, three studies of electrical workers reported an increased risk for male breast cancer, and a modest increase in risk of breast cancer was later noted in a study of women in electrical operations. Since breast cancer was already a focus of intense public concern and epidemiologic research, several large studies of female breast cancer were initiated in the 1990s to address EMF. At the same time, researchers extended their investigations to diseases other than cancer, specifically neurological diseases [including Alzheimer’s disease, Parkinson’s disease, ALS (amyotrophic lateral sclerosis)], depression, and cardiovascular disease. Other outcomes such as miscarriage were also studied. In this way, epidemiologic research proliferated to include an array of chronic diseases as well as other conditions potentially caused by exposure to EMF. Thus, what began as a single question led to a series of linked but independent questions. There was a continual extension of the object of study to new entities. At the same time, as research progressed, there was a concomitant improvement in methodology and measurement of exposure. In this way, once the question of a hazard from power-frequency EMF became a focus of interest for epidemiologists, it took on a life of its own.
SUBSEQUENT STUDIES IN THE 1980s
In the years immediately following the Wertheimer and Leeper paper, a number of reports on the possible association of EMF with cancer were published in medical and epidemiologic journals. The most important of these was a study from Stockholm, Sweden, that examined the occurrence of leukemia in children and adults in relation to the distance of the residence from high-voltage transmission lines, as well as one-time measurements of EMF at the front door of residences.5 (In Europe, unlike in the United States, most secondary distribution lines are buried underground.) This study reported a strong positive association with brain cancer in children with exposure to very high measured fields and with historically reconstructed fields but not with leukemia. Several other residential studies showed no effect.
In addition, a number of letters to journals presented information on the mortality and incidence experience of workers with presumed high exposure to EMF, such as telephone linemen.6 These early occupational studies were even more problematic than the residential studies. First, most of them were based on comparing “proportionate mortality” (that is, the proportion of deaths due to leukemia, or some other cause, as a proportion of all deaths) of workers in jobs presumed to entail elevated EMF exposure with that of the general population or of workers in jobs judged to have no or low exposure. This type of study is difficult to interpret because higher proportionate mortality does not necessarily imply higher mortality rates. Second, all occupational studies lacked direct measurements of fields and, therefore, had to rely on job titles to infer exposure. However, actual exposure could vary greatly among people with the same job title, and tasks as well as exposures are likely to have changed over time. Third, these studies were not able to take into account other concomitant occupational or lifestyle exposures that might affect cancer risk. In spite of the inconsistencies between studies and the many methodological limitations, these studies were taken in the aggregate as providing some support for an association and, therefore, justifying further epidemiologic research.
One consequence of the Wertheimer and Leeper paper was to attract the interest of David Savitz, who in the early 1980s was a young assistant professor of epidemiology at the University of Colorado in the same department as Wertheimer and was looking to develop his own research program. In contrast to Wertheimer and Leeper, neither of whom was an epidemiologist, Savitz had received rigorous training in epidemiology and, for this reason, had the credibility to carry out a study in Denver designed to confirm or refute his colleagues’ controversial findings. In the early 1980s, Savitz obtained a grant for a second study of childhood cancer in Denver from the New York State Power Lines Project, which had been set up with funding from the electric power industry. In describing that period, Savitz told me that, to most scientists at the time, the idea that EMF from power lines could cause cancer seemed “flaky,” and he himself was ambivalent about studying such a fringe question.7 Yet little was known on the topic, and, given the nearly universal exposure to extremely low-frequency electromagnetic fields, even if there was only a low probability of health effects, he felt it was justified to carry out careful epidemiologic studies. Such studies, he argued, would provide valuable information needed for decision making by the electric power industry as well as regulatory agencies and the public health community.
Savitz’s study, which did not appear until 1988, represented a clear improvement over the original Denver study.8 He and his colleagues enrolled all 356 residents of the Denver metropolitan area under 15 years of age who had been diagnosed with any form of cancer between 1976 and 1983. Controls were recruited via random digit dialing, a standard technique used in this type of study to obtain a representative sample of the healthy population. Exposure assessment entailed both wire coding (performed by technicians who were unaware of the case-control status of the residence) and spot measurements of electric and magnetic fields in a number of rooms and near the front door. The researchers included all new cases of childhood cancer, as opposed to deaths in the Wertheimer and Leeper study.
As reported by the authors, measured magnetic fields under low power conditions showed “a modest association” with cancer incidence. Contrasting homes with fields of 2 mG or higher with homes having fields of less than 2 mG resulted in an apparent 40 percent excess for total cancers, a doubling of leukemias and lymphomas, and a threefold increase in soft tissue sarcomas. No association of measured fields with total cancers was seen under high power use conditions. Contrasting the two highest wire code categories with lower categories yielded a 50 percent excess for all cancers combined.
In spite of its superiority to the original Wertheimer and Leeper study, Savitz recognized that his study had a number of serious limitations. These included poor compliance with the measurement component of the study (64 percent of cases and 20 percent of controls lacked measurement data), resulting in limited data on specific types of cancer, differential mobility between cases and controls (controls were more residentially stable than cases), and the fact that the measurements taken were only “imperfect surrogates for long-term magnetic field exposure history.” Perhaps most importantly, the elevations in risk were not statistically significant, and there was no indication of a dose-response relationship with increasing level of exposure to measured fields (table 4.2). The elevations in risk noted for individual cancers when high measured exposure was contrasted with lower exposure (2 mG or higher versus less than 2 mG), were not even close to being statistically significant, and the estimates were extremely “imprecise” due to the exceedingly small numbers cases and controls in the highexposure category. Finally, no trend was seen with longer duration of occupancy of the home in which measurements and wire codes were made.
TABLE 4.2 Cancer Risk in Relation to Measured Electric and Magnetic Fields, Denver, Colorado Standard Metropolitan Statistical Area
mG, milligauss. Source: Savitz et al., 1988.
In discussing his results, Savitz carefully described the limitations and weaknesses of his and similar studies. First, consistency was lacking in the detailed findings of the five residential studies of EMF and childhood cancer. Second, the magnitude of the associations found by Wertheimer and Leeper was larger than those observed in his study. Also, Savitz pointed out that “it would be erroneous to interpret the literature as a series of replicated positive results.” In other words, the individual studies were different enough in their methods, populations, and results to make it ill advised to interpret them as providing unambiguous confirmation of an effect. In spite of these careful distinctions and caveats, Savitz’s study was interpreted by many epidemiologists and lay persons as confirming the findings of the original study, which had raised the issue of power lines and childhood cancer, or at least providing enough suggestion of a possible association to justify carrying out further studies to resolve the “uncertainties.”
DIVERGENT ASSESSMENTS OF RISK
By the late 1980s and early 1990s a sufficient number of studies (approximately fifty by 1990) had appeared to enable epidemiologists to review the whole body of evidence. Such critical reviews provide an opportunity to examine the consistency of results from different studies as well as the strengths and weaknesses of individual studies. For this reason, they can be influential in directing further research as well as influencing the regulatory process. For our purposes, they also allow one to gauge the range of interpretations of the EMF issue among epidemiologists roughly ten years after the appearance of the Wertheimer and Leeper paper.
A lengthy review article by Savitz and colleagues published in 1989 critically reviewed the early studies and proposed methods for improving the quality of future research.9 Savitz’s role all along had been to press for increased methodological rigor. He reasoned that if there was a causal link between EMF and disease, as the methods improved, more compelling evidence of a risk from EMF should emerge. First and foremost, Savitz and colleagues argued that the assessment of EMF exposure needed to be strengthened. Use of wire configurations and spot measurements were only crude surrogates for what one wanted to know, that is, long-term exposure to EMF from all sources. Exposure assessment could be improved by making use of personal dosimetry (that is, using personal monitors that record EMF exposures over a period of a day or more) to attempt to validate the surrogate markers (including stationary measurements and wire codes). This could be done in both residential and occupational studies. A second area was the assessment of confounding by means of analyzing data on other factors, which are correlated with wire codes or field measurements and which might themselves be risk factors for cancer. Traffic density, an indicator of air pollution, was one such potential confounding factor. Third, selection bias was a major concern since controls tended to be harder to enroll than cases, and some factor related to participation might be influencing the association of EMF with disease. Finally, Savitz and colleagues emphasized the importance of evaluating the temporal dimension of exposure and testing different assumptions since the relevant timing of exposure for leukemia and other cancers is not known. Since EMF is not a cancer initiator and is not mutagenic, it was considered more likely to act as a promoter or growth stimulator. This could mean either that duration of exposure over a number of years might be a key variable or, alternatively, that exposure shortly before detection of clinical disease might be most relevant.
The program Savitz outlined, and to which he contributed abundantly, made an immense contribution to the strengthening of epidemiologic studies of EMF that took place during the 1990s. But there was an inherent conflict that made it difficult, if not impossible, to effectively advocate further study of the problem and at the same time give a thoroughly tough-minded assessment of the existing evidence. If Savitz was too critical and dismissive of the existing evidence, he might undermine the argument for the need for further research. Thus, it is interesting to note that his interpretation of existing studies, while accurate, is couched in language that betrayed this tension. He details their many methodological weaknesses and notes the inconsistencies among them. And yet, somehow these studies seem to add up to something more, although this “something more” is quite vague:
Thus, the literature on residential exposures provides some evidence of an effect of electromagnetic fields on childhood cancer. The findings are inconsistent among even the positive studies regarding the magnitude of effect of the specific cancers that might be most affected, but there is some consistency in the general direction of the findings. Adult cancers have been less consistently associated with these exposures.10
In the conclusion to the review, Savitz and colleagues refer to “several suggestions that prolonged magnetic field exposure . . . may increase the risk of leukemia and brain cancer.” However, they continue, “these studies fall short of providing conclusive indications for a causal association.” This is actually quite an understatement. In fact, there is a huge gap between the “suggestions” from the early studies and a strong case for causality. But Savitz, like many epidemiologists, needed to minimize this gap in order to obtain the funding necessary to do the work that he thought was important and justified.
A similar ambivalence is evident in Savitz’s references to experimental studies of EMF. He claimed that, “There is now growing evidence of numerous biologic effects at relevant frequencies,” even though he acknowledged that none of these effects offered direct evidence of carcinogenicity. Furthermore, it is now known that most of these results have proved to be not reproducible.
In this moot situation, with very weak epidemiological data “suggesting” a hazard from EMF, public perceptions and the potential public health implications took on a decisive role. Here is the conclusion of Savitz’s review:
The potential public health impact of this environmental agent argues strongly for continuing and expanding efforts to confirm or refute the reported associations with cancers in adults and children. Policymakers who address power line right-of-ways, home buyers, and even potential users of electrical appliances face decisions which implicitly include judgements about the likelihood of adverse effects. The present state of uncertainty makes it impossible for society or individuals to make these decisions in a scientifically informed manner.11
In contrast to Savitz’s review, an article published two years later, in 1991, by Poole and Trichopoulos provides a very different assessment of the question of EMF and cancer and how it should be interpreted.12 Poole and Trichopoulos gave an even more critical reading of the existing studies than did Savitz, including Savitz’s Denver study. Because of its importance and prominence, they devoted nearly two pages to a detailed discussion of that study. A major concern was that differences in socioeconomic status or residential mobility between cases and controls introduced by biased selection of controls could have affected the results in unpredictable ways. Considering the available studies, Poole and Trichopoulos concluded that, “there is little, if any, such coherence with respect to childhood cancers, even though many researchers seem to agree that the strongest evidence concerning hypothetical causation by ELF-EMF comes from the childhood cancer studies.” They then considered the possibility that the risk estimates might be underestimates due to the problem of misclassification of exposure (resulting from the inability to accurately measure fields). Poole and Trichopoulos showed that this could in fact be the case. However, they went on to argue that if the relative risks associated with “high wire code” exposure were on the order of 5 or 10 (rather than 1.5 to 3), given the four-fold increase in electric power consumption in the United States between 1950 and 1987, we would be witnessing an epidemic of childhood cancers. In fact, they noted, the incidence of childhood cancers has increased little, if at all, over this time period.
In closing, Poole and Trichopoulos discussed the plausibility of an EMF-cancer link. They referred to the two main types of evidence relevant to assessing the question: that from epidemiological studies on the one hand and from experimental studies in the laboratory on the other. These two types of evidence, they argued, are complementary. The stronger the evidence of an association (i.e., substantial relative risks) in well-designed epidemiologic studies, the less a causal interpretation hinges on a credible biological mechanism. Conversely, if there is strong experimental or other biological evidence of a mechanism, a weak or inconsistent association can be given a causal interpretation. However, neither of these conditions obtained in the case of EMF and cancer. In their judgment, “the notion that ELF-EMF can cause cancer is not impossible or absurd but it is hardly plausible.” In conclusion, Poole and Trichopoulos pointed out that research on ELF-EMF had been going on for only slightly more than a decade. This was less time, they observed, than was required for the link between cigarette smoking and lung cancer—a much stronger association—to achieve acceptance. Their final paragraph is worth quoting in full:
The hypothetical carcinogenicity of ELF-EMF represents an intriguing scientific problem and a potentially important public health issue but, at this stage, nothing more. It clearly is not possible to exonerate ELF-EMF. In order to do so, very large and valid studies showing very little or no association between ELF-EMF and cancer would be needed. This condition is not presently fulfilled. On the other hand, the empirical evidence linking ELF-EMF to cancer is weak and inconsistent. Causal interpretations are not supported by the available biologic data. This is an area in which more and better research, and an atmosphere conducive to dispassionate inquiry, are clearly needed.13
What Poole and Trichopoulos managed to convey is an unflinching view of the available evidence and a refusal to go beyond it. At no point did they relax their critical faculties, whether they were considering the evidence from epidemiologic studies, from laboratory experiments, or from changes in electric power distribution and in childhood cancer rates over time. They refused to play up the threat to public health angle because the available evidence was “weak and inconsistent.” And they made clear that they deplored the misappropriation of early epidemiologic findings by a sensationalizing media and by regulatory zealots. In accounting for Poole and Trichopoulos’s ability to render an impartial and intellectually rigorous judgment on this question, it is pertinent to note that neither of them has been engaged in primary research on the effects of EMF. Thus, their research support is not dependent on their taking a particular position on this issue.
Trichopoulos, who is a professor of epidemiology at Harvard, was also a member of an expert panel that reviewed the existing evidence on the carcinogenic potential of ELF-EMF for Oak Ridge Associated Universities in 1992. The panel reached the conclusion that further research on EMF was not a priority. In a letter to Science magazine in 199314 the authors of the Oak Ridge report subjected three Swedish studies to scrutiny, pointing out the many inconsistencies in their results, as Poole and Trichopoulos had done for the U.S. studies. In the final paragraph of the letter, the authors attempted to put the whole issue in perspective:
We have never stated that a causal association between EMF and cancer is impossible or inconceivable; we have indicated that the evidence for such an association is empirically weak and biologically implausible. We have not proposed that research concerning the health effects of EMF be discontinued; in fact, we have indicated areas of some scientific interest that warrant consideration for future research. However, given the decreasing resources available for basic health and science research, we believe that in a broader perspective there are currently more serious health needs that should be given higher priority.15
The kind of unrelentingly critical and logical assessment of the evidence presented in these two reports is in stark contrast to the message that was conveyed by epidemiologists involved in primary research on EMF and, even more so, to the message conveyed by the media and regulatory agencies.
ENTER PAUL BRODEUR
In 1989 the investigative reporter and staff writer for the New Yorker Paul Brodeur published a series of three articles in that magazine claiming that “radiation” from power lines, electric blankets, and video display terminals posed a hazard to the nation’s health and that this danger had been systematically suppressed by the government and industry. Later that year the articles appeared as a book entitled Currents of Death: Power Lines, Computer Terminals, and the Attempt to Cover Up Their Threat to Your Health.16 Brodeur’s chatty, fact-filled account of research into these hazards made gripping reading. Through the articles, the book, and his appearances on prime time television, his exposé reached a wide audience and had an enormous impact.
What made Brodeur’s account so compelling was the unequal contest he dramatized between a small number of researchers who were convinced that their data demonstrated harmful effects and the monolithic “establishment” consisting of the military, the government, industry, and most of the scientific community committed to denying the existence of a hazard. Brodeur’s protagonists were a handful of maverick scientists and medical researchers who were portrayed as selfless and courageous, whereas their opponents in the establishment were depicted as cynical and corrupt. It is revealing that, in introducing his protagonists, Brodeur humanized them by describing their physical appearance and their accomplishments, but when he introduced his villains, their physical attributes and their substantial accomplishments did not merit mentioning. All the reader was told was that a given scientist had testified for industry or authored a report that was allegedly favorable to the government or industry. In this way, the reader always knew what the author wanted him to think of a given scientific figure and how to judge his position. Brodeur needed this device in order to fashion a fast-paced narrative in which every building block fitted in with his thesis. While he was not wrong to be skeptical of the military-industrial complex, he seemed unaware that this is not the only methodological tool needed to decode reality. He saw conspiracy everywhere and saw reality as monolithic. The National Academy of Sciences was as suspect as the Pentagon. Furthermore, the only vested interests he acknowledged were those of big industry and government. He showed no awareness that there are subtler forms of vested interest, including that of scientists—and journalists—in selecting results that support their position.
Brodeur’s predisposition to credit evidence of a hazard led him to elevate studies that had not been confirmed and to ignore or impugn the work of outstanding scientists. The resulting tissue of misrepresentations, biased reporting, and outright errors was so extensive that, in 1991, the Committee on Man and Radiation of the Institute of Electrical and Electronics Engineers (IEEE) published a 36-page critique of the book entitled “Currents of Death Rectified” in which scientists whose work had been distorted by Brodeur addressed specific points to set the record straight.17 Brodeur’s style was designed to persuade the reader of his ability, as a rigorous investigative journalist, to penetrate to the truth behind biased testimony and obfuscatory government and industry reports. However, as the IEEE report documents in detail, throughout his account he conflated distinct phenomena and failed to make crucial distinctions. For example, he discussed the radiation from VDTs as if it were the same as that from power lines and electric blankets, when in fact they are quite different. At key points, he failed to make a fundamental distinction between electric and magnetic fields. And he confused pulsed radiation generated by radar systems with the phenomenon of amplitude modulation. For all The New Yorker’s vaunted reputation for checking the facts in its articles, no one detected that Brodeur’s whole narrative was vitiated by his willingness to select those findings that supported his position.
While Brodeur may be less than trustworthy as a science writer, ironically he probably did more than any other individual to galvanize research into the effects of EMF. His writings and the general news media, along with the more balanced newsletter Microwave News, helped create a level of urgency in the general public and the government to assess the alleged threat from power lines and other sources of EMF. As mentioned above, in spite of the recommendation of the Oak Ridge expert panel that research on EMF was not a priority, in 1992 the Congress mandated the creation of the EMF-RAPID program funded by the Department of Energy and administered by the National Institute of Environmental Health Sciences to promote basic research into the health effects of ELF-EMF. This program focused on laboratory and experimental studies and on carrying out a risk assessment of EMF. In addition, substantial epidemiologic research was funded by the National Cancer Institute, the National Institute of Environmental Health Sciences, and the Electric Power Research Institute (EPRI), which was supported by the electric power industry. The existence of a high level of public concern worked in favor of scientists involved in studying the effects of EMF since it permitted them to remain impartial and sober, merely pointing out that even a small excess risk applied to the large exposed general population would constitute a significant pubic health problem. Epidemiologists could do what they are professionally disposed to do, focus on conducting further research and attempting to synthesize the available data and explain apparent inconsistencies and anomalies. Brodeur and others had created an avid constituency for their work.
ISSUES PREOCCUPYING THE EPIDEMIOLOGISTS
Once the question of the health effects of EMF was raised by Wertheimer and Leeper and subsequent studies in the 1980s, epidemiologists devoted themselves to carrying out better studies of this question. Research focused on the technical difficulties of studying an exposure as complex and variable as ambient EMF, and epidemiologists focused on a small number of key issues.
First and foremost was the task of assessing exposure to electromagnetic fields. As Wertheimer and Leeper had pointed out, wire codes were only a poor surrogate for the current flowing through power lines, and their use assumed a constant level of current, when in fact the actual level was apt to vary over time. In addition, use of wire codes did not take into account other sources of EMF, like household appliances, ground currents, and exposures outside the home. What epidemiologists wanted to know was how informative were wire codes and short-term measurements as markers of long-term exposure?
Other questions preoccupying epidemiologists studying the health effects of EMF included confounding (the possibility that some other factor that was correlated with exposure to EMF was responsible for the observed association between EMF exposure and disease), selection bias (which could occur in case-control studies if the controls are not drawn from the same underlying population as the cases), the timing of exposure relative to the development of disease, and the appropriate exposure metric (that is, what aspect of EMF exposure actually exerted a biological effect?).
Epidemiologists applied themselves to addressing these issues, and over a period of twenty years the quality of the studies improved substantially. The assumption underlying this research was that following the logic and methods of the discipline should lead to a clarification of the relationship of EMF with cancer. This clarification might take one of three forms. First, a stronger association of EMF with disease might emerge from better studies. Second, improved studies might show no evidence of a relationship. Third, some other factor might be identified that would explain the initial association of wire codes with cancer. This program occupied epidemiologists working in this area from the 1980s through the late 1990s. However, the tendency to work within the confines of one’s discipline and to focus on technical and methodological issues—understandable though it is—can be an occupational hazard. Their inward looking posture made the epidemiologists less disposed to pay attention to questions that lay outside their area of expertise. The possibility that there might be no biological effects from the very weak electromagnetic fields encountered in everyday life was rarely acknowledged.
THE MELATONIN HYPOTHESIS
No one had ever proposed a plausible biological mechanism by which power-frequency electromagnetic fields could cause leukemia or brain cancer. However, starting in 1987, an intriguing hypothesis was put forward that identified a specific mechanism by which electric power might be implicated in a much more common tumor, breast cancer. Richard Stevens, an epidemiologist at Battelle Pacific Northwest Laboratories, proposed that electrification might be associated with increased rates of breast cancer owing to its effects on the hormone melatonin.18 Stevens cited limited evidence suggesting that two aspects of electric power—exposure to EMF and to artificial light-at-night—could decrease the normal nocturnal rise in melatonin. Melatonin, a hormone produced by the pineal gland in response to darkness, has a number of physiologic properties that are relevant to carcinogenesis. First, it inhibits the production of estrogen and other hormones believed to fuel the growth of breast cancer. It also inhibits tumor growth in experimental animals and humans and is a free-radical scavenger. Finally, melatonin has immunostimulatory properties. Thus, suppression of melatonin by exposure to EMF or to light-at-night might increase the risk of breast cancer either through the deregulation of estrogen or by other means. While human data supporting an effect of EMF exposure and light-at-night on melatonin levels were scant, many epidemiologists agreed that the hypothesis was worthy of further study. The “melatonin hypothesis” provided epidemiologists with an attractive and seemingly plausible rationale for how by-products of electric power could contribute to the development of breast cancer, and a number of studies were initiated in the 1990s to explore this possibility. Adding to the appeal of the hypothesis was the recognition by the mid-1990s of the failure of large prospective studies to confirm the influential hypothesis that dietary fat intake was an important risk factor for breast cancer. The new hypothesis’ focus on electric power also fitted in with the growing interest in the possible role of environmental pollution in the etiology of breast cancer.
THE PHYSICISTS GET INVOLVED
By the early 1990s, a number of physicists had begun to turn their attention to the issue of health effects of extremely low frequency electromagnetic fields. They were concerned about what they saw as the grossly distorted public perception of a threat from ambient exposure to EMF fostered by the media and by regulatory agencies and fed by epidemiologic studies. Furthermore, they felt that valuable resources were being wasted on the study of this dubious threat. The involvement of physicists was to have an important impact on the further course of the controversy.
In the late 1980s, Robert K. Adair, a physicist at Yale University, became interested in the claims regarding health effects from EMF. He had devoted a thirty-year career to research in elementary particle physics, was a member of the National Academy of Sciences, and held the title of Sterling Professor of physics at Yale. As he approached retirement age, he had looked around for a problem he could work on without having to run a large laboratory typical of research in high-energy physics. Through this wife Eleanor Adair, an environmental biologist and authority on microwave radiation, he attended several meetings on the biological effects of EMF and got to know many of the key figures in that area. Adair saw that there was “a bit of a gap” in the physics of biological interactions of low-frequency EMF, which he wanted to understand better. In 1991 he published a major paper in the journal Physical Review in which he used fundamental physical principles to call into question the possibility of health hazards from ambient exposure to power-frequency EMF.19 Entitled “Constraints on biological effects of weak extremely-low-frequency electromagnetic fields,” the paper started out from the position that, due to the low energies of such fields, any contribution to cancer or leukemia incidence could not be due to the breaking of bonds in DNA. Rather, it would have to involve “less catastrophic effects” that are not well characterized or understood.
Adair defined weak fields as electric fields below 300 V/m in air (the mean electric field at the Earth’s surface is about 100 V/m) and magnetic fields no greater than 50 µT (or 500 mG), the strength of the Earth’s magnetic field. In order for an externally generated electric or magnetic field to have an effect on cellular physiology, the fields would have to exceed the level of endogenous “thermal noise.” As he put it to me, all of the molecules in our body are “jiggling around” at a temperature of 36.7 º C. This normal level of thermal noise is referred to as kT, that is, a constant times temperature in degrees Kelvin. If the mean energy of the molecules in one’s body is altered by as little as 3 percent, “then you’re going to be dead.” In his 1991 paper, Adair demonstrated that due to the resistivity of tissues and cell membranes, fields actually penetrating the body are in fact far weaker than the thermal noise effects—by many orders of magnitude—and therefore cannot be expected to have any significant effect on the biological activities of cells. Having described the properties of thermal noise within tissues and cell membranes, Adair proceeded to consider different aspects of EMF—electric fields, static and changing magnetic fields, pulsed magnetic fields, and different types of resonance—demonstrating for each scenario that the fields produced are well below the level of thermal noise. In each case he invoked the principles of classical physics to bring clarity to the discussion of specific mechanisms by which EMF could affect biology. He concluded that “there are good reasons to believe that weak ELF fields can have no significant biological effect at the cell level—and no strong reason to believe otherwise.”
In spite of the paper’s thoroughness and provocative conclusion, Adair was not certain that he was right. As he put it in an e-mail to me in 2004:
Negative arguments, such as those that say that weak fields cannot affect biology are always suspect as being possibly incomplete. I was not completely converted myself for a long time. When I published the 1991 paper, I rather expected that someone would come up with an angle that I had missed. Indeed, it was much later, after I had considered matters at greater length—and published perhaps ten more papers on the subject—that I became a complete convert myself to the view that environmental fields of 10 mG indicted in the epidemiology cannot possibly affect biology. By that time, no one had found any convincing theoretical process—or convincing experimental data—that would allow power-line frequency fields less than 500 mG to affect biology. Since any effects near threshold must increase with the square of the magnetic field (for AC fields, the average field strength is always zero) or the energy density, the safety factor is not 500/10, or 50, but 2500.20
In an article written for the layman in the late 1990s and entitled “The fear of weak electromagnetic fields,” Adair was both more outspoken and more accessible.21 He likened concern over weak EMF from power lines to the fear that leaves falling from trees could fracture a person’s skull. “Electric fields alleged to be carcinogenic and generated in humans by the 60 Hz, 5 milligauss (mG) magnetic fields from an electric power distribution system will be only about ten millionths of a volt per meter (V/m) and cannot induce an energy transfer to biologically significant molecules greater than one-millionth kT.” “Direct magnetic effects are also possible. . . . But at 60 reversals a second, the magnetic forces cancel out and the energies transmitted to magnetic elements in animals by 60 Hz, 5 milligauss, fields can be expected to be less than 1/10,000 kT. Neither birds, bees, fishes, nor humans can even detect such weak 60 Hz fields, let alone be harmed by them.” How then was one to account for the numerous experimental studies purporting to show effects of exposure to EMF? Adair pointed out that after more than twenty years of research, there were no reproducible, agreed upon effects, and he attributed most findings to experimental error. He contends that much of the research in this area, fed by public concern and the availability of funding, was published and accepted uncritically by many who had a stake in there being health effects of ambient EMF. As an experimentalist in high-energy physics, Adair judged the vast majority of experimental work on this question to be of extremely poor quality.22 The reporting of an exciting new finding was typically followed by a failure of other researchers be able to reproduce it. To give just two examples: a key experiment by one prominent researcher was judged to involve scientific misconduct;23 another piece of work by the Environmental Protection Agency’s lead EMF researcher was shown by Adair to be explainable only if the data were somehow corrupted.24 If Adair is right, the failure of reviewers and editors to assess research in this area with the requisite degree of rigor and skepticism has contributed to a distorted perception of the issue.
A colleague of Adair’s at Yale, William R. Bennett Jr., had also used basic physical principles to clarify the EMF issue. Bennett holds professorships in both engineering and physics and is the coinventor of the gas laser. He had served on the Oak Ridge Associated Universities panel, which produced the highly critical report in 1992. Bennett’s involvement in the controversy over potential human health effects of EMF led him to write a book on the topic, as well as an article published in Physics Today.25 The article gives a carefully reasoned account of how EMF from man-made sources compare to natural fields present in the environment and in our bodies. Having undertaken a survey of electric and magnetic fields typically encountered in the urban environment, Bennett determined that the highest sustained ELF fields were associated with electric railroads. As a “worse-case scenario,” he calculated the fields that would be experienced by a person standing barefoot on the wet tracks of an electric railroad. Although the external electric field near the barefoot railroad walker’s head would be 12,000 V/m, the peak internal field would be only about 80 µV/m (or 1/10,000,000th the external field). This last value is many orders of magnitude smaller than the electric fields normally occurring within the body.
Another difficulty confronting epidemiologic studies of EMF was raised by Adair in a paper published in the Proceedings of the National Academy of Sciences in 1994.26 For the most part, epidemiologic studies had assumed that the pertinent exposure metric was the mean field strength. Adair commented that this assumption “seems to have been made by default with no guidance from biophysical models.” In actuality, he argued, biological responses to weak 60-Hz electric and magnetic fields must vary as the square of the field strength. This argument directly addressed the question acknowledged by epidemiologists that in investigating the effects of EMF they were operating in the dark as to what metric—that is, what parameter of EMF—was pertinent in inducing biological effects. If Adair was right, the parameterization of exposure in the epidemiologic studies was wide of the mark, and their elaborate statistical analyses might be meaningless. It is symptomatic of the disjunction between the epidemiologists and the physicists raising fundamental questions about the biophysical effects of EMF that this paper was not cited by the epidemiologists.
The vocal case mounted by Adair, Bennett, and other physicists for consideration of fundamental biophysical properties in the evaluation of the health effects of EMF was instrumental in persuading the American Physical Society and the National Research Council of the National Academy of Sciences to undertake independent reviews of what was known about the health effects of EMF. The American Physical Society’s report was published in 1995 and the National Research Council report in 1997.27 Both documents came to the overall conclusion that there was no compelling evidence of adverse health effects on humans.
However, these reports from prestigious institutions did not put an end to the controversy. When the National Research Council report was published, three members of the panel, all former presidents of the Bioelectromagnetics Society, put out their own press release to counter that of the National Research Council. Furthermore, the tension between skeptics and those who felt that, although weak, the data could not be completely dismissed left its imprint on the report itself. The report’s executive summary was written by the chairman of the committee, Charles Stevens, a neurobiologist at the Salk Institute, and presents a forceful conclusion that the existing science provided no evidence of a hazard from exposure to 60-Hz EMF:
Based on a comprehensive evaluation of published studies relating to the effects of power frequency electric and magnetic fields on cells, tissues, and organisms (including humans), the conclusion of the committee is that the current body of evidence does not show that exposure to these fields presents a human health hazard. Specifically, no conclusive and consistent evidence shows that exposures to residential electric and magnetic fields produce cancer, adverse neurobehavioral effects, or reproductive and developmental effects.28
If one reads the body of the report, and particularly the section on the epidemiology, the message is quite different, leaving open the possibility of effects.29 However, whatever the tensions within the committee, most people only read the executive summary, and it was the overall conclusions that got reported in the media. The American Physical Society and the National Research Council reports represented important milestones in putting the EMF problem in a scientific perspective.
A NEW GENERATION OF STUDIES
By the early to mid-1990s the emphasis of epidemiologists, like Savitz, on improving the quality of epidemiologic studies of EMF began to bear fruit. In 1991 a study from Los Angeles reported results on 232 cases of childhood leukemia and an equal number of control children.30 In contrast to previous studies, assessment of exposure in this study included a 24-hour measurement in the child’s bedroom and a number of spot measurements in other locations within the house and outdoors in addition to wire coding. Measurements were made in up to two homes lived in during relevant “etiologic period” between the estimated date of conception and a date preceding diagnosis. Although wiring configuration was associated with leukemia, with a doubling in the odds ratio for very high relative to very low current and underground configuration combined, the researchers found no association of measured fields with leukemia risk.
A major study of magnetic fields and cancer in children residing near Swedish high-voltage power lines was published in 1993 by Feychting and Ahlbom.31 The study base consisted of all children under the age of 16 years who had lived on a property within 300 m of any of the 220 and 400 KV power lines in Sweden between 1960 and 1985. Using the Swedish Cancer Registry, a total of 142 cancer cases were identified, including 39 cases of leukemia and 33 central nervous system tumors. A total of 558 healthy children were selected from the base population for comparison. Exposure was assessed by spot measurements and by calculation of the magnetic fields generated by the power lines, taking distance, line configuration, and historical information on the loads into account. When historical calculations were used, a nearly threefold excess risk of leukemia was found for children with higher exposure, whereas no association was seen for central nervous system tumors, lymphomas, or all childhood cancers combined, contradicting the earlier study carried out in Stockholm.
This study had a number of strengths, including the availability of national statistics on historical power loads and a nationwide cancer registry. The design made use of the fact that residents near transmission lines would have significant exposure compared to those living at a greater distance. Of great importance was the fact that selection of controls from the same base population as the cases greatly reduced the likelihood of selection bias, which was a concern in studies carried out in the United States.
Feychting and Ahlbom interpreted their results as “providing more support for an association between magnetic fields and childhood leukemia than against it.” However, in spite of making use of the entire Swedish population under age 16 over a twenty-five year time period, the number of cancers of specific types was limited. Also, as was pointed out in a letter to the American Journal of Epidemiology, the reported association with leukemia was one of a very large number of comparisons made by the researchers and hence could well have arisen by chance.32 Furthermore, as the writers of the letter pointed out, one of the study’s key results was not statistically significant, to which Feychting and Ahlbom replied that they never claimed that it was.
In July 1997 the results of a large case-control study of childhood leukemia carried out by the National Cancer Institute appeared in the prestigious New England Journal of Medicine.33 This study was considerably larger and methodologically more rigorous than most of the previous studies. The researchers enrolled 638 children with acute lymphocytic leukemia (ALL) who were under 15 years old and 620 matched controls. Exposure to EMF was assessed by means of a 24-hour measurement in each child’s bedroom, spot measurements in other rooms and near the front door, and wire coding (conducted in a blinded fashion) of the subjects’ current and former homes. Using the measurement data, the researchers computed a time-weighted average residential magnetic field. They reported that risk of ALL was not increased in children who had resided in homes in the highest wire code category or in homes with higher average measured fields (0.20 µT or greater) compared with 0.065 µT. Furthermore, there was no suggestion of an increased risk with increasing level of exposure. The main results are shown in the table 4.3.
Publication of the National Cancer Institute childhood leukemia study and the National Research Council report represented serious challenges to the notion that power-frequency EMFs posed a cancer hazard. It is fair to say that these two reports, following the American Physical Society report, marked a turning point in the widespread, uncritical acceptance of EMF as serious threat to the nation’s health. However, not all parties were willing to conclude that there was no compelling evidence of a hazard. The final report from the National Institute for Environmental Health Sciences EMFRAPID program, which was published in 1999, stuck a somewhat different note.34 If a tension was discernable in the National Research Council report between the overall conclusions announced in the executive summary and the section on the epidemiology, in the NIEHS report this tension emerged into the conclusions themselves. While acknowledging that virtually all of the experimental and mechanistic studies failed to demonstrate adverse effects and that the epidemiologic evidence was weak and inconsistent, a majority of the NIEHS working group, nevertheless, on the basis of the admittedly weak and inconsistent epidemiologic evidence, voted to classify EMF as a “possible carcinogen.” The Director of NIEHS, Kenneth Olden, recommended that, in view of the remaining uncertainty concerning health effects due to EMF, passive regulatory action aimed at reducing exposures was warranted. But in the key paragraph of the report summarizing the epidemiologic evidence, the reasoning is strained and highly questionable:
TABLE 4.3 Risk of Childhood Leukemia (ALL) by Time-Weighted Average Summary Levels of Residential 60-Hz Magnetic Fields
Source: Linet et al., 1997.
None of the individual epidemiologic studies provides convincing evidence linking magnetic field exposure with childhood leukemia. Hence, in making an assessment, one must rely upon the evaluation of the data as a whole using expert judgment and the meta-analyses as a guide. The pattern of response, for some methods of measuring exposure, suggests a weak association between increasing exposure and increasing risk. The small number of cases in these studies makes it impossible to firmly demonstrate this association. This level of evidence, while weak, is still sufficient to warrant limited concern.35
First, one should immediately be wary if the data are not compelling without resorting to “expert judgment” and meta-analysis. “Expert judgment” seems too suggestive of experts who have an investment in a field to which they have devoted years of work. Furthermore, the results of meta-analysis can be highly questionable when the studies being combined differ in the details of their methods and the biases that affect their results. It is hard to escape the impression that the reluctance of the NIEHS working group to close the door on the possibility of EMF as a cause of leukemia had more to do with its members’ stake in this area of research than with scientific rigor.36
The null results of the National Cancer Institute childhood leukemia and several other large studies in the late 1990s led epidemiologists to carry out further analyses of the existing data to determine whether distorting factors, such as confounding and selection bias, could explain the association between EMF and childhood leukemia.37 Although the results of studies differed, taken as a whole, they suggested that selection bias and confounding by such factors as socioeconomic status and traffic density could partially account for the observed association.
In addition, two pooled analyses of existing studies of EMF and childhood leukemia came out in 2000, in effect summing up twenty years worth of epidemiologic research on EMF and childhood leukemia.38,39 Both analyses involved going back to the original data from each of the studies in order to make full use of the available information, rather than relying solely on the published reports. By using the original data, the researchers were able to maximize the comparability of different studies carried out in different geographic locations. Furthermore, pooling studies greatly increased the sample size and made it possible to examine the dose-response relationship. It also made it possible to look at differences between studies (rather than assuming homogeneity amongst the studies) as well as interrelationships between different exposure measures (i.e., wire codes and measured fields). All in all, these two papers provide some of the most thoughtful discussions of the actual data from the epidemiologic studies that have appeared to date.
There was substantial overlap in the studies included in the two analyses, so that many of the same investigators are authors on both papers. However, the two analyses included somewhat different numbers of subjects and used somewhat different approaches, which could account for some of the divergences in their results. Both analyses failed to find clear evidence of a dose-response relationship between field strength and risk of childhood leukemia. In both studies, there was no indication of increased risk below the highest exposure category (>0.3 µT in Greenland et al. and >0.4 µT in Ahlbom et al.), but both reported a modest but significantly increased risk for the highest category (i.e., roughly a twofold risk in both studies). This high exposure group, however, represented only a minute fraction of the total population (2 and 0.8 percent, respectively). Both analyses yielded results that contradicted the so-called “wire code paradox,” but their findings differed. (The wire code paradox refers to the fact that use of wire codes—a crude surrogate—tended to show stronger associations with childhood cancer than use of actual measurements of fields.) Greenland and colleagues found that “very high” versus “very low” wire code was associated with increased risk and that wire codes were “strongly” associated with measured fields. (They noted, however, that these results were based on only four studies and were very unstable.) In contrast, Ahlbom et al. found no increased risk associated with residing in homes in high wire code categories. In fact, they noted that “the measured fields are low in all the wire-code categories.” This represented a striking reversal of the association of wire codes with measured fields, which had so preoccupied epidemiologists throughout the 1980s and 1990s, and cast doubt on the usefulness of wire codes. The authors went on to say, “The reasons for the elevated risk estimates for high wire-code categories in the earlier North American studies are unclear, although considerable potential for bias has been noted for both studies carried out in Denver.” (The difference between the two analyses regarding wire codes may be explained in part by the fact that Ahlbom et al. excluded the study by Savitz et al., whereas Greenland et al. included it.)
Both papers emphasized the methodological difficulties of epidemiologic studies of EMF, given the incomplete assessment of exposure, the potential for selection bias and confounding and the fact that the only hint of increased risk occurs in the miniscule group with the highest exposure. Greenland et al. were unsparing in articulating the uncertainty of the results of their analysis:
Biases due to measurement errors are undoubtedly present in and vary across all of the studies, but their assessment is not wholly straightforward. . . . Only under fairly restrictive conditions can one be certain that the net bias due to such error will be toward the null. Unfortunately, there is little or no evidence to establish such detailed attributes of the errors, and there is no basis for assuming such attributes are the same across studies and measures. . . . Furthermore, the associations are imperfect enough to indicate that probably all of the measures suffer considerable error as proxies for any biologically relevant exposure measure (if one exists). . . . These problems should further expand the considerable uncertainty apparent in our results.40
In their conclusion, Ahlbom et al. devoted a forceful paragraph to the resoundingly null evidence from laboratory studies, implicitly correlating those null findings with the lack of an association in 99 percent of the children included in the pooled analysis:
The results of numerous animal experiments and laboratory studies examining biological effects of magnetic fields have produced no evidence to support an aetiologic role of magnetic fields in leukaemogenesis (Portier and Wolfe, 1998). Four lifetime exposure experiments have produced no evidence that magnetic fields, even at exposure levels as high as 2000 µT, are involved in the development of lymphopoietic malignancies. Several rodent experiments, designed to detect promotional effects of magnetic fields on the incidence of leukaemia or lymphoma have also been uniformly negative. There are no reproducible laboratory findings demonstrating biological effects of magnetic fields below 100 µT.41
Noting that the elevation in risk observed in 0.8 percent of their data (the twofold increase in the risk of leukemia) needs to be explained, they suggested that selection bias may have accounted for part of the excess.
Both papers emphasized that, in order to clarify the nature of the association observed in the small group with the highest measured exposure, future studies would have to be conducted in highly exposed populations, preferably in densely populated countries like Japan. These two analyses of the existing epidemiologic evidence conveyed a very different picture from that found in the majority of epidemiologic papers and reviews (with notable exceptions like Poole and Trichopoulos).
EMF AND BREAST CANCER
In 2002 and 2003, three large studies appeared, doing for breast cancer what the National Cancer Institute study had done for childhood leukemia.42 The studies had been carried out in Seattle, Los Angeles, and on Long Island and incorporated at least one twenty-four hour measurement in the woman’s bedroom in addition to spot measurements in other rooms and wire coding. (I should note that I was a coauthor on the Long Island report.) These studies took measurements in multiple homes or limited their enrollment to residences that had been occupied by the study subjects for at least fifteen years prior to entry into the study. In this way, they attempted to assess EMF exposure relevant to the decade or two preceding the diagnosis of breast cancer. They also evaluated effects of “harmonics” (i.e., multiples of the 60-Hz fields) in addition to the fundamental 60-Hz frequency fields, ground currents, and electric appliances, including electric blankets. Strikingly, none of these studies showed any hint of an association of exposure to EMF with breast cancer, whether wire codes or actual measured fields were examined. Carried out in different areas of the country and published within a short interval, these studies went a long way toward ruling out the possibility that EMF was an important cause of breast cancer.
In addition, the study from Seattle, Washington, had measured nighttime urinary melatonin levels over a period of three days in two different seasons of the year but found no strong or consistent relationship between residential exposure to EMF and melatonin levels. Since the melatonin hypothesis had been proposed in the late 1980s, most studies designed to address the question had provided little support for an effect of EMF on melatonin levels in humans.43 (Studies of exposure to light-at-night and shift work, which can depress the normal rise in melatonin during the night, in relation to breast cancer have yielded inconclusive results. However, there is intriguing evidence that blindness may reduce the risk of breast cancer.) Finally, eight studies that examined the association between use of electric blankets and breast cancer also failed to find evidence of increased risk. These studies contributed important information since electric blankets, especially older ones, entailed relatively high exposures. In publishing the eighth null report on the association of electric blanket use and breast cancer, the editor of the journal Epidemiology voiced the opinion that the issue was now dead.44
LESSONS OF THE EMF STORY
The evolution of the EMF controversy over a period of nearly twenty-five years is marked by a number of paradoxes and contradictions. By failing to present a balanced and critical view—such as that presented by Poole and Trichopoulos in 1991—epidemiologists and experimentalists engaged in research on EMF contributed to an exaggerated concern about health effects from power lines and other sources. Their work fed the journalistic and regulatory appetites for “evidence” of this hazard. At the same time, the high level of anxiety among the public, federal agencies, and industry was responsible for the allocation of research funds that would not otherwise have been forthcoming. As a result of intensive work by epidemiologists, however, a marked improvement in the quality of studies took place, and the later studies were able to either dispel concern about a hazard (in the case of female breast cancer) or put a very low upper limit on the possibility of a hazard (in the case of childhood leukemia). It is clear that these studies would not have been undertaken on such a large scale or as quickly as they were had it not been for the enormous societal anxiety and economic interests at stake. Work got done that otherwise would not have been done. So, one might reason that, in spite of the cost and the widespread and unnecessary public alarm, something positive came out of the process. But it is reasonable to ask, what is the value of that work? Not surprisingly, the answer to this question depends on whom you ask.
One response was given by Edward Campion, an editor at the New England Journal of Medicine, who wrote an editorial accompanying the 1997 National Cancer Institute childhood leukemia study. Under the title “Power lines, cancer, and fear,” Campion summed up the EMF issue in the bluntest possible terms.45 After enumerating the weaknesses of the epidemiologic studies, he wrote: “Moreover, all these epidemiologic studies have been conducted in pursuit of a cause of cancer for which there is no plausible biologic basis. There is no convincing evidence that exposure to electromagnetic fields causes cancer in animals, and electromagnetic fields have no reproducible biologic effects at all, except at strengths that are far beyond those ever found in people’s homes.” (It is noteworthy that, in addition to the National Research Council report, Campion cited the 1991 paper by Poole and Trichopoulos and the Oak Ridge report of 1992.) He went on to conclude that, owing to unfounded fears about EMF, hundreds of millions of dollars were wasted on investigating a hypothesis that never had any biological evidence to support it and that made no contribution to advancing our understanding of the causes of childhood leukemia.
A very different point of view is implicit in a commentary by Savitz entitled “Health effects of electric and magnetic fields: Are we done yet?” which appeared in the journal Epidemiology in 2003.46 Where Campion addressed the issue in the broadest terms and took an outspoken position, Savitz, writing for epidemiologists, confined himself to the question of what further research after the past twenty-five years was worth undertaking and publishing on this topic. Even allowing for the fact that Savitz’s commentary is directed at epidemiologists, the narrowness of his focus is striking. The whole implication of the piece is that epidemiologic research on EMF has basically accomplished what it can accomplish and that, barring a major improvement in methods or the emergence of solid “empirical” evidence that would justify the study of specific outcomes, new studies are unlikely to be productive. While stressing the need for empirical, as opposed to merely theoretical support for a hypothesized biological mechanism, Savitz does not see fit to comment on the fact that decades of empirical research on mechanisms whereby EMF could affect biology have failed to produce any replicable findings. In contrast to Campion, he does not refer to skeptics like Poole and Trichopoulos or the Oak Ridge report, to say nothing of physicists like Adair and Bennett. While drawing distinctions about what further epidemiologic work on EMF is warranted, Savitz chooses not to draw any lessons from the past twenty-five years or to even point out any problems that are visible in retrospect. His narrow focus allows him to avoid confronting questions concerning the value of the work that was done, why it essentially failed to uncover evidence of a hazard, and whether the issue could have been approached differently from the start.
While Campion’s editorial may have performed a useful function in questioning the value of research on EMF, in one respect his position is extreme. Even physicists like Adair and Bennett and skeptical epidemiologists like Poole and Trichopoulos do not go so far as to deny any value to research on this topic. Rather, they argue that the facts of the case did not justify a “crash program” and special “set-aside” funding for such studies. In their view, studies of health effects of ELF-EMF should have competed for funding in the general grant pool on an equal footing with other investigator-initiated proposals. Adair also concedes that some research may be justifiable, including studies of high exposures, such as those encountered by users of electric blankets.
There is no need to be quite as categorical as Campion is. One can take exception to the exploitation of poorly founded fears and still concede that useful knowledge has been gained through the epidemiologic studies. Some of those studies have been able to address other potential risk factors such as overcrowding and traffic congestion, and it is conceivable that these lines of work could lead to new insights in the future. The fact that high measured fields in the recent pooled analyses are associated with a slight increased risk of childhood leukemia points to something that still needs clarification.
A further justification for conducting such studies, given by Savitz and others, is that this research can allay serious public concerns about novel exposures. As Savitz pointed out to me, epidemiological studies cannot rule out the existence of a very weak effect, but if they are well designed and large enough, they can put an upper limit on a potential hazard. They can allow us to say, “Look, we know that there are no dire effects from everyday exposure to EMF. This is not some catastrophe.”
Thus, one benefit of continued study of EMF is that epidemiologists were able to put a potential hazard into a sharper perspective. In a review article published in 1995, the Swedish epidemiologists Feychting and Ahlbom calculated that if residence near high-voltage transmission lines in Sweden was in fact associated with a doubling of the risk of childhood leukemia (as indicated by three high-quality studies from Scandinavia), this would translate to less than one case per year out of a total of 70 being due to this exposure.47 Given the many methodological issues surrounding the epidemiology and the considerations raised by the critics, this estimate of 1/70 can be looked at as the sort of upper bound referred to by Savitz. However, in response to a question posed to Adair by Louis Slesin, the editor of Microwave News, Adair put his own estimate of the probability of any contribution of ELF-fields of less than 10 milligauss to cancer at one in a million.
In looking back at the trajectory of the EMF controversy over a period of twenty-five years, it is significant that epidemiologists involved in studying the effects of EMF rarely made use of the criteria for judging the causality of an association, first proposed by Austin Bradford Hill and discussed in chapter 2.48 How does the available evidence fit the four most important of Hill’s criteria? First, regarding the magnitude of the association, the Wertheimer and Leeper study reported risk estimates of 2–3, but most subsequent studies reported risk estimates between 1 and 2. Risk estimates in this range are sufficiently weak that the effects of bias are difficult to rule out. Second, as we have seen, there were numerous inconsistencies when the results of the studies were examined in detail. Third, there was also a striking absence of a dose-response relationship with increasing strength of measured fields. Finally, the criterion of “biological plausibility” was never satisfactorily addressed by those making the case for adverse health effects of EMF. This criterion requires epidemiologists to take account of what is known from other disciplines. In the case of EMF, this would have meant a rigorous assessment of the laboratory and mechanistic studies and an understanding of the relevant physics.
If physicists like Adair and Bennett were right, there were compelling reasons, based on the biophysics of the interaction of ELF-EMF with human tissues, to think that no mechanism was likely to be discovered in the future. Their arguments shed light on why many intriguing experimental results—seized on by Brodeur and highlighted in the newsletter Microwave News—had never been convincingly reproduced. The case put forward by the physicists was directly relevant to addressing biological plausibility. Allowing for a time lag of several years (since the articles of Adair and Bennett were not published in epidemiology journals), one might have expected that by the mid or late 1990s their work would have been cited by epidemiologists working on EMF. However, this was not the case. The careful arguments made by Adair and Bennett concerning the possibility of adverse—or beneficial—health effects from weak ELF-EMF encountered in everyday life went without mention in the epidemiologic literature. This is even more surprising given that Adair had attended meetings of the Bioelectromagnetics Society and published in the society’s journal Bioelectromagnetics, as did many epidemiologists working on EMF. One cannot escape the impression that epidemiologists caught up in the methods and data from their own discipline had no time or interest to enlarge their field of vision to incorporate the highly relevant point of view of the physicists. In epidemiology papers published in the years 2000 to 2004, I was able to find only one reference to a paper of Adair’s49 and no references to his most wide-ranging and provocative paper from 1991, “Constraints on biological effects of weak extremely-low-frequency electromagnetic fields” or to Bennett’s 1994 paper in Physics Today. Furthermore, in no article on the epidemiology of EMF that I am aware of has there been any discussion of the viewpoint put forward by the physicists.
In his interview with me, Adair, who, at nearly eighty, is mild mannered and laughs easily, expressed the view that the epidemiologists were arrogant, that they felt that their discipline was paramount because they were engaged in measuring actual exposure and linking it to the occurrence of disease in humans. What is clear is that the epidemiologists’ “tunnel vision” kept them focused narrowly on the results of their studies to the exclusion of fundamental insights about the phenomenon whose effects they were investigating. After all, nature does not recognize the distinctions between academic disciplines.
Box 4.1 Major Take-Home Points
The question of possible adverse health effects of exposure to ambient electromagnetic fields (EMF) from power lines, home appliances, and other sources became an issue of interest to scientists and of concern to the public with the publication of an epidemiologic study in 1979. Although relying on a crude assessment of exposure, this study seemed to point to an association between childhood cancer and proximity to power distribution lines.
Further epidemiologic studies were carried out, and, by the late 1980s, the topic of EMF had become the focus of intense regulatory and media attention and enormous public concern. The quality of the epidemiologic and laboratory studies, however, was poor, and the results were weak and inconsistent. Nevertheless, the apparent indications of links to a growing number of diseases created the widespread perception of a hazard.
There was a split among scientists, with those engaged directly in research on EMF feeling that there was justification for further study of this question, and “outsiders” arguing that decades of research had produced no evidence of reproducible biological effects of the weak electromagnetic fields encountered in daily life. Furthermore, a number of physicists argued a priori that these fields were highly unlikely to have any effects because they were many orders of magnitude smaller than the energy levels within the body.
Owing to the publication in the late 1990s, and after, of a number of large epidemiologic studies showing no association of EMF exposure with either childhood leukemia or female breast cancer, as well as the acknowledgment by regulators of the failure of experimental studies to yield reproducible results, fears of EMF began to wane and to be put in perspective.



