PACK-Teen Treatment Protocol
Mary Nord Cook
In an era of ever-decreasing inpatient and partial hospitalization stays, coupled with shrinking community resources, increasing numbers of patients need intensive outpatient behavioral health services that are readily accessible, convenient, efficacious, and cost-effective. There is a significant need for clinic-ready, manualized treatments for diagnostically complex, treatment-refractory youngsters, who present with a range of emotional and behavioral disturbances. A manualized Intensive Outpatient Program (IOP) was developed at Children’s Hospital Colorado (CHCO) in January 2006, to serve a broad and diffuse patient population, aged 7–18 years old, referred on the basis of clinical acuity rather than primary diagnosis. To ensure standardization of service delivery and enable program dissemination, the written materials were deliberately evolved to be explicit and readily followed. To the best of our knowledge, no other published, manualized programs are available that target a broad and diverse patient population referred based on acuity, symptom severity, treatment refractoriness, and level of functional impairment, rather than diagnosis. Chapter 4 describes the parent training component of the adolescent or teen treatment protocols that served the families of patients 12–18 years old. The child treatment protocols, targeting 7–12 year olds, and their families, were previously published in 2012.
Keywords
Treatment refractory; comorbid; diagnostically diffuse; parents; families; children; adolescents; teens; Intensive Outpatient Program (IOP); cost effective; efficacious; manualized; evidence-based; standardized
Established Parent Introductions and Check-Ins
Each Parenting Approaches for Challenging Kids (PACK)-Teen session follows a similar pattern and routine. Ask established or returning parents to remind the group of their first name and the name of their adolescent, who is enrolled in the program. After their first week, ask parents to check-in briefly regarding the past week, or interim period, since the last session. Cue them to relate one example of a “victory” (required) during which they used a new skill during a parent–teen interaction, in support of their self-identified individual or family treatment goals. They may additionally relate an instance of a “challenge” (optional), describing an experience during which they or their teen attempted to use a new skill or complete the “family homework,” but struggled and felt their effort was only partially successful or had outright failed. The point should be repeatedly reiterated so that we can learn from victories or successes and challenges or failures. All efforts and experiences are fodder for personal and family growth, if appropriately examined, discussed, and understood.
Workshop Guidelines
Following introductions briefly go over the group guidelines, inviting established or returning parents to assist with the process. Use of the word “rules” is avoided because it tends to invite resistance—even among adults. Guidelines include the following: punctuality is required, pagers and cell phones must be turned off, and of course, confidentiality is required. During the discussion of confidentiality, point out the few exceptions to confidentiality, which relate to client safety (e.g., suicidality, homicidality, abuse). Make the point, that part of maintaining confidentiality means that while they are enrolled in the treatment program, they and their teens should refrain from developing personal relationships that transpire outside of group sessions. This point should be made explicitly and despite doing so, many adolescent patients may still covertly develop friendships and even romantic connections, while in program, that sometimes become inappropriate and distracting. Many teens referred to such programs struggle with maintaining balanced and healthy interpersonal boundaries and often rush relationships, in a desperate effort to make connections with peers and feel liked and accepted. Therapists can’t control whether or not this happens, but they certainly can and should make the point explicitly, to both parents and teens, that personal communications with group peers, outside of sessions, is contraindicated, at least while in treatment. The guidelines should be mentioned at the start of each group session. Without this practice of routinely reminding the group of expectations every visit, inevitably parents will violate group guidelines, which may take the form of forgetting to turn off electronics, coming late, or leaving early.
New Parent Introductions and Check-Ins
After established or returning parents have introduced themselves, and “checked in,” go around the room and ask new parents or caregivers to identify themselves by first name; mention their adolescent’s name, sex, and age; and then comment on first one strength, talent, or positive attribute of their teen, followed by one challenging trait or behavior pattern, for which they are seeking help and guidance. Parents of adolescents with histories of emotional and behavioral problems are often surprised and ill-prepared to be queried about and report upon their teen’s strengths. Many in our programs have endorsed that the inquiry during the check-in and introduction process is the first time they recall having been asked about positive qualities their teens possess, in a long line of involvement with behavioral health providers and services. They find it refreshing but are often taken aback.
Once all new parents have had an opportunity to share one strength and challenge pertaining to their teen, ask the returning parents whether or not the challenge mentioned resonates for them, in reference to their own families. Encourage at least one or two of the established group members to relate a commonality, tied to the challenges reported, with respect to their current or past experiences and concerns regarding their own teen. The terms “strength” and “challenge” are used as cues for new parent check-ins, inviting them to identify and comment on a more global attribute, quality, or trait of their teen. The terms “victory” and “challenge” are used to cue returning or established parents, thereby inviting them to relate specific instances of attempts to apply new skills or strategies.
By creating a highly structured format for the introductions and check-ins, as well as reminding parents at the start of each session of those explicit expectations, emphasizing the direction to share briefly, the stage is set to contain that phase, for the sake of ensuring adequate time for didactic discussion, skills training, and practice of skills. This predictable and structured format serves to proactively prevent inappropriate or excessively prolonged check-ins. Setting clear expectations and structuring the check-ins in advance, increases the odds that parents are mindful of time limits and follow specific workshop guidelines, rather than having to be interrupted or redirected, by group facilitators, after they’ve launched into potentially lengthy and counterproductive check-ins.
During the check-ins, it is important for the clinicians to refrain from problem solving immediately as parents share concerns; instead, it is better to simply note the concerns and tie them into later discussions and practice of skills. Nearly every issue or experience related by parents during check-ins may be used as an example during the didactic and skill-building portion of the workshops. In fact, using examples from check-ins for practice the same day or week increases the degree of relevance and engagement experienced by parents during skill-building exercises; therefore, if parents request immediate attention to concerns raised during check-ins, encourage them to remember their questions and use them for practice during the subsequent portion of the same session.
The separate weekly, individual therapy session provided to each family creates a forum for customized safety planning and problem solving around issues pertaining to specific youth, which may not have been adequately addressed during the group sessions. In addition, the third weekly session, which occurs if implementing the Intensive Outpatient Program (IOP) service delivery model, uses the media of art and music to reinforce concepts and rehearse skills, from the first two weekly, more structured, language-based sessions. This creative arts session additionally provides a forum for whole families to process their feelings and express themselves within a less structured intervention, using nonverbal modes of experience and learning.
New Parent Orientation
If using a “rolling” style of admission, new patients may be joining the workshop at any time, mixed together with “established” parents, who are returning after attending previous sessions. New parents should already have been oriented to the program content, format, and logistics, as part of a standard intake process that occurs prior to the first session, but inevitably they either claim to not have been oriented at all or to have forgotten some portions of their orientation. This has occurred frequently, at our site, despite the practice of routinely providing families with both verbal and written summaries detailing program components and expectations, during their intake.
Provide a brief orientation of the program to new parents at the start of their first session, recruiting established or returning parents to assist with this process. A PACK-Teen program syllabus, copies of which are available in the book’s companion website, can be handed out to each new parent during their first session and reviewed, as a way of orienting to all program topics or skill sets. Additionally, the program’s format, including its different components, times, days, and locations, can be reviewed briefly by the therapists, assisted by returning parents. Details regarding options for the program format are provided in a separate section, titled “Format and Operations.”
Managing Parental Resistance
When parents first enroll in PACK IOP-Teen, it is common for them to focus on trying to change their adolescents; they often are eager to quash their teen’s maladaptive behaviors and engender in them more respectful, compliant, and deferential attitudes. Parents often endorse a desire to rid their teens of angry or distressed feelings and effect change in their adolescent’s overall attitudes, behavior patterns, and styles of relating; however, they usually will acknowledge that the more they have attempted to change or control their teen’s behavior, attitudes, or feelings, the more their youngsters have resisted.
You may want to ask parents, “What can you control?” in reference to effecting changes to their adolescent’s difficult behaviors. The answer, of course, is that the parents can control how they approach and respond, to their teen as well as the behavior they model. However, because families can be understood as “closed systems,” in which changing one element inevitably reverberates and effects change throughout the system, the power to modify their end of an interaction is often enough to effect the changes they desire in their adolescents. Parents often have commented to us, “It took me a little while…but we finally figured out the intervention is actually targeting us—not our teen!” Such a reflection is partly true, although it is our experience that the most effective and powerful way to effect change in an adolescent is to intervene simultaneously and equivalently with both the parents and their teen. A phrase that captures a principal tenet of PACK IOP-Teen places emphasis on an aspect of the parent–adolescent relationship over which the parents have full control and is as follows: “Model the behavior you want to see.”
Parents who are newly admitted to a program like this are often, “at the end of their rope” and commonly lament, “We’ve tried everything! Nothing works!” Exhausted and stressed parents of teens often feel as though they have failed and are incompetent. They often feel guilty, embarrassed, and helpless, a mindset commonly associated with a psychological defensive posture which manifests in the form of devaluing or negating others. That is, because it is so uncomfortable to feel as though one is incompetent, especially at the highly valued role of parent, parents who are struggling might be inclined to devalue and criticize clinicians and programs attempting to help. The underlying assumption, which is probably mostly an unconscious one, is that “Look, if I’m feeling incompetent then everyone must be incompetent. There is no solution or effective method—otherwise, I would have identified it by now.”
However, typically, their past failed efforts were focused mostly or exclusively on the teen, without sufficient attention to the contexts and systems surrounding the teen, by far the most important of which is the family, particularly the parents. The critical shift of paradigms that must occur, for meaningful family system changes to occur is the notion that parents can be powerful change agents in relation to their teen’s attitudes and behaviors. However, that is only the case if parents focus their efforts on optimizing their own attitudes and behaviors, including that which they model, along with the patterns by which they approach and respond to their teen. You might point out that most families already have much of what they need to emotionally support one another—but those resources just need to be discovered and cultivated. Essentially, most families already possess a set of “ruby slippers.” They are often simply unaware or at a loss as to how to operate them.
The experience parents often relate of encountering increasing levels of resistance as they have escalated their efforts to change or control their teen’s behavior, feelings, or attitudes, can be understood by considering humanistic theory as formulated by Carl Rogers (1961), who espoused that humans are most able to change, once they feel unconditionally accepted by others, and ultimately themselves. He stated, “The curious paradox is that when I accept myself just as I am, then {and only then} I can change” (p. 17). Humanistic theory serves as a fundamental tenet for Parent Effectiveness Training, a parent training program focused on fostering a sense of unconditional positive regard through empathic communication between parents and children (Gordon, 2000). A similar philosophy or formula for psychological healing is encouraged in the PACK IOP-Teen program, aka, “If you accept teens as they are … then they will change.” Such a suggestion often feels counterintuitive to most parents, who might initially respond with skepticism or resistance. Established parents, who’ve already recently experienced the benefits of empathic communication, can often assist in helping overcome the resistance and skepticism that may be held and espoused by new parents.
Workshop Format, Past Topic Review, Family Homework
Once orientation, introductions, check-ins have been completed, write the current session’s overarching topic on a dry erase board, and delineate specific time allocations for each component. It is helpful to give a mini-review (no more than 10 minutes) of what was discussed in the previous session, prior to launching into new material. The clinicians should invite returning members to assist in this process as a way of engaging them, assessing their degree of retention and also reinforcing previously taught constructs. If using a rolling style of admission, newly joined members can be reassured by the therapists that they will receive exposure to the briefly reviewed topic, in much greater depth when their cycle through the program predictably rotates back to that particular module.
After briefly recapping the previous sessions’ topic or skill set, begin that day’s discussion, using an interactive, experiential, and psycho-educational style. The basic sequence of interventions, for each module includes psycho-education, using an interactive format, introduction of new topics and skills, modeling of new skills and then provision of an opportunity for parents to rehearse them. The parents and teens will later join, to rehearse skills together and then families are assigned additional practice exercises, to perform at home, in between sessions. All modules contain homework assignments for families; worksheets related to homework are given to parents (and teens) at the end of group sessions; these sometimes involve activities or parenting interventions and other times paper-and-pen exercises.
“What About My Teen?” Examples
After every major topic or skill set, it is advisable to pause and invite the group to share and discuss examples from their own lives that relate to the topic covered in the current module. Encourage the parents to share either relevant victories or challenges; either type of scenario can provide teachable moments.
Handouts and “Business Cards”
All of the sessions have corresponding handouts, available in the book’s companion website that can be given to the parents to review information covered during the group, either during the session, or at its close. Provide parents with these handouts as the related material is covered during the session, rather than in advance. In some cases, modules have associated worksheets that are intended for teens and parents to complete during the session. If workbooks have not been assembled by the clinicians in advance, advise the parents to keep their handouts together, in a safe place at home. Encourage them to maintain all handouts in a protective folder, or notebook, for future reference. Most modules also contain “business cards” reviewing material as well, which may be cut out, and provided to parents during the workshop to serve as a reminder. Laminating the cards elevates the level of preciousness of the cards and in our experience, increases the likelihood the cards will be kept and safeguarded for future reference. The parents may also be given copies of the “business cards” to keep, to tuck in their wallets and save for future reference.
Alternatively, all handouts and worksheets, except those required for homework in between sessions, can be preprinted and assembled into workbooks. These workbooks can be handed out to parents on their first day, but should be maintained by the clinicians, when not in use. They should be given out, when needed, during the workshop, but collected and held by the therapists in between groups. Otherwise, parents inevitably forget to bring them to sessions, or become distracted by them during group, sometimes flipping through them, even when they are not being referenced. The workbooks can be given to parents to keep, at the point of graduation. For convenience and to facilitate flexible use, all handouts are available digitally as separate documents, in the book’s companion website.
Introductions, Check-Ins, and Orientation Summary Outline
• Copies of parent handouts or workbooks
• Established Parent Introductions and Check-Ins
• Have the introduction and check-in format for new versus established parents written on the board.
• Go around the room and have each established parent take turns doing as follows:
– Ask each parent to identify themselves by first name.
– Ask each parent to mention their teen’s first name.
– Ask each new parent to mention one “victory” or success (required) and “challenge (optional),” from past week, related to their teen.
– Ask one or two returning or established parents to share commonalities pertaining to the teen challenges related by the new parents.
– If there are new parents, invite each established parent to help in orienting the new parents to the workshop format and guidelines.
– Established parents may check-in regarding their family progress, including approaches they tried which were effective thus far.
• Workshop consistently starts on time and finishes on time, punctuality required, leaving early or stepping out of workshop during session, not allowed.
• Confidentiality required, “What is said in here, stays in here,” playfully termed the “Vegas Rule.”
• Exceptions are safety issues (suicidality, homicidality, violence, abuse/neglect).
• Part of maintaining confidentiality includes refraining from communicating with group peers, outside of sessions, while enrolled in the program.
• All cell phones, pagers, electronics of any kind must be turned off during group.
• New Parent Introductions and Check-Ins
• Have the introduction and check-in format written on the board.
• Take turns having each parent introduce themselves and check-in as follows:
– Ask each parent to identify themselves by first name.
– Ask each new parent to mention one positive feature or strength of their adolescent and mention one “challenging behavior” they’d like to focus on.
• If new parents present, provide brief overview of what to expect from program, review PACK-Teen Syllabus, format for IOP program (three sessions weekly, describe how sessions vary from one another, etc.).
Handouts/Business Cards
Module 1-PACK-Teen Handout #1
PACK-Teen Module 1
Introductions and Guidelines
Begin Module 1 of the PACK-Teen program with a brief orientation if there are new members, introductions, “check-ins,” and a review of workshop guidelines, as detailed in the PACK-Teen Introductions, Check-Ins, and Orientation section. Follow the same basic routine at the start of each session. After introductions and “check-ins” are completed, mention the overarching topic of the current session, and write the schedule for the day on a dry erase board, with time allocations specified for each section. If there are new parents, provide them with copies of the program syllabus, and take a few minutes to review it, including briefly highlighting the topics or skill sets to be covered, throughout the program. For subsequent sessions, review these elements as needed for new members, including providing them with copies of the program syllabus, along with recruiting established parents to welcome and briefly orient new ones.
Review
Once introductions have been made, guidelines have been reviewed, and the current session’s topic mentioned, conduct a brief review of material from the previous session for no more than 10 minutes. Recruit returning parents to assist with this process.
Treatment Goals: Individual and Family
Throughout the program, there is an emphasis on clearly and concisely articulating primary treatment goals, for each individual, and their family. Likewise, both teens and parents are repeatedly encouraged to focus on their own role in improving family cohesion and functioning. Participants are routinely invited to contemplate goals they can realize and behavior changes they can personally implement. Parents are reminded to “Model the behavior you want to see” and that “If you accept teens as they are … then they will change.” It is common for both parents and teens to initially present with a defensive posture, in a blaming mode and the more the facilitators and their peers can shift them away from that position, the more open, flexible, and workable they become.
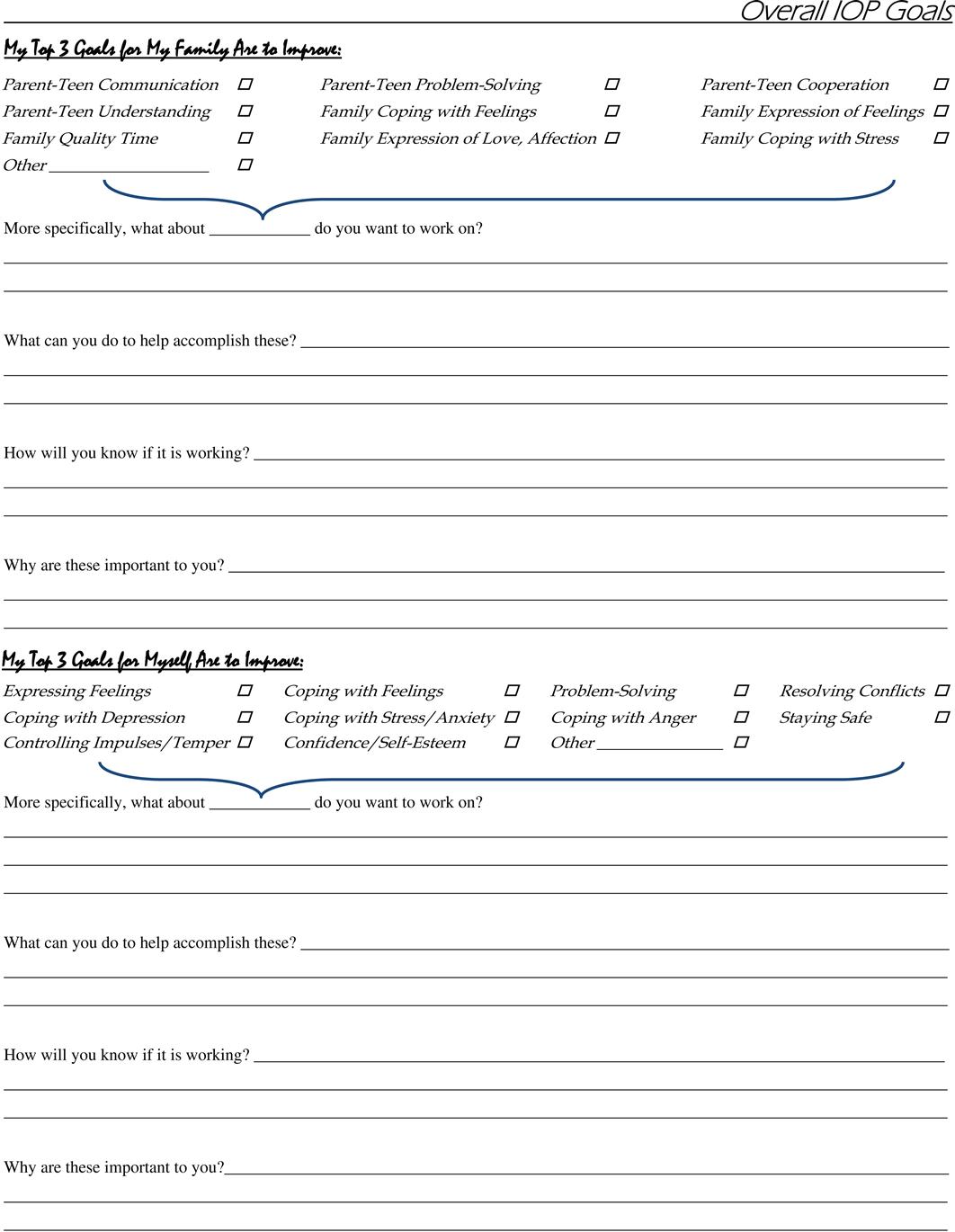
Ask parents to identify both an individual and family goal, during their first session, which is connected to the topics or skill sets covered in the program. When the expectation of formulating goals which are highly relevant and specific to the program is not made clear, it is very common for parents to identify treatment goals that are irrelevant, unrealistic, or vague, such as “I want to be a better parent,” or “I’d like my teen to move out.” A goals worksheet should be provided to new group members, at the end of their first session. They should be advised to further contemplate and write out their individual and family goals at home, prior to the next session. The worksheet contains several explicit directions and cues, which help parents focus on goals that are relevant, measurable, and realistic.
Other parents in the group and therapists may assist new parents with formulating and potentially reframing, specific treatment goals, if needed. As new parents share their experiences and reasons for entering the program, they can usually be readily guided to formulate specific treatment goals, which tend to flow naturally from their past experiences, including both challenges and victories. Additionally, the parents are expected to formulate and relay to their group, their ideas and plans for achieving their self-identified individual and family treatment goals.
During subsequent sessions, as part of routine check-ins, invite parents to discuss their progress in relation to each of these goals. Returning parents should have completed a goals worksheet, that they may be cued to reference, throughout the program, during “check-ins.” The parents are repeatedly urged to identify and comment on their own strengths and challenges, as well as their teens’, throughout the program, which may impact goal attainment, positively or adversely. Treatment goals can be established during Module 1 or the parent’s first session if using a “rolling” style of admission, but are typically dynamic and evolve throughout the course of the program, as each family masters various skill sets and achieves behavioral and relationship targets.
Feelings: Good, Bad, and Ugly Ones
Feelings Overview
Remind the parents that a primary goal of the program is to arm them with knowledge and tools in support of modeling, teaching, and reinforcing the psychosocial skills, on which the teens are being coached, with a goal of skills mastery for entire families. To that end, they will be acquainted with similar kinds of materials and urged to perform practice exercises, in parallel to the domains covered by teens. To begin, the most fundamental and universally relevant topic that merits their attention is the exploration of feelings or emotions, followed by strategies for effectively managing and coping with difficult or uncomfortable feeling states.
Ask the group whether they think emotions are important, and then have them indicate whose feelings they consider important. Typically, they will conclude that yes, feelings are important and that everyone’s feelings are important, at least to the person having them and those who care about that individual. Make the point that youngsters who struggle to regulate their emotions and control their impulses often come to view emotions, especially forms of anger, as “bad”; likewise, they often come to view themselves as “bad” for frequently expressing their emotions in an ineffective or even destructive manner. Because many of the youngsters enrolled in the Mastery of Psychosocial Skills (MaPS) IOP-Teen program have histories of being extremely reactive to emotions, and additionally often live in households wherein family members, including parents, may have modeled ineffective expression of emotions, learning to regulate and express emotions appropriately, is often a focus of treatment for many families.
Using a psycho-educational and Socratic style of teaching, ask questions about emotions, with the goal of helping the group recognize and acknowledge that experiencing a full range of emotions is perfectly normal and, in fact, unavoidable. Generate discussion to help the parents recognize that feelings are not good or bad—they just are—and that it is normal to experience anger, along with a full range of emotions, on a regular basis. Assist the group in recognizing that all feelings are part of the human experience and serve important functions.
Facilitate discussion regarding how emotions, even uncomfortable or difficult emotions, are often expected or understandable. Have the parents provide examples of when this might be the case. The goal of this discussion is to guide the group to recognize that their emotions serve a purpose and can often fuel positive, appropriate change. An example the parents might suggest is becoming angry in response to a bully mistreating their teen, propelling them to inform a counselor or administrator, for the sake of protecting their youngster and eliminating the bullying. An additional example might include instances during which citizens become outraged enough about an injustice that they are energized and mobilized to try to make things right and effect positive change. Depending on the examples the parents themselves are able to generate, you may want to contribute examples from history such as the actions of Rosa Parks, Mahatma Gandhi, and Martin Luther King, Jr.
While acknowledging that all feelings are normal and acceptable, in and of themselves, ask the group to discuss whether or not behavioral responses or reactions to emotions should be managed or limited. It is important to reiterate and reinforce the point, however, that unmanaged or inappropriate expression of emotions can be destructive, hurtful, and wrong.
Help the parents realize the point, that if feelings can be proactively monitored, labeled with words, discussed and processed, they can be understood and managed in healthy, adaptive ways, rather than destructively acted out. Ask the group if any of them are in the habit of monitoring, labeling, and verbally communicating their feelings with others, on a frequent basis. Most parents will indicate they have no such habit and little to no experience with monitoring, labeling, or conveying their feelings (aside from anger, perhaps, which they may have experience expressing aggressively). Recommend that parents target a goal of becoming expert at monitoring their own feelings; appropriately identifying and labeling them; and then expressing them in safe, nondestructive, nonhurtful ways. If they can become masterful in their ability to monitor, label, and express feelings, and routinely model effective mood regulation and interpersonal processing of emotions, they can support their teen’s progress in powerful ways. Remind the parents, “Teens don’t do what we say. … They do what we do!”
Ambivalence or Mixed Feelings
Facilitate discussion regarding the potential for experiencing two or more different conflicting emotions at the same time, by asking the group, “Is it possible to feel happy and sad at the same time?” Or “Is it possible to feel angry and hurt at the same time?” “Is it possible to be mad at someone and love them at the same time?” Ask whether more than one emotion or even seemingly conflicting emotions can be experienced simultaneously. Guide the group, through Socratic discussion, to recognize that emotions, like people and relationships, are complicated and that often individuals experience a variety of overlapping or even conflicting emotions simultaneously.
Foster additional discussion among the group regarding the phenomenon of ambivalence in relationships. Ask the parents to define the term ambivalence, cueing them to formulate a simple and concise definition, such as “a mix of bad and good,” or “mixed feelings.” Help the parents recognize and accept that everyone feels anger occasionally, even toward people they love very much. Generate discussion regarding the fact that all relationships and all people are a mix of good and bad. Make the point that just because people sometimes feel angry, including toward people they love, does not mean that they are bad people or that they do not love those at whom they have been angry. Inform the group that while experiencing intense emotions, all human beings may sometimes experience fleeting thoughts or wishes to harm others; as individuals age and mature, however, they learn to control their impulses and refrain from acting out aggressive thoughts or fantasies.
Feelings Vocabulary
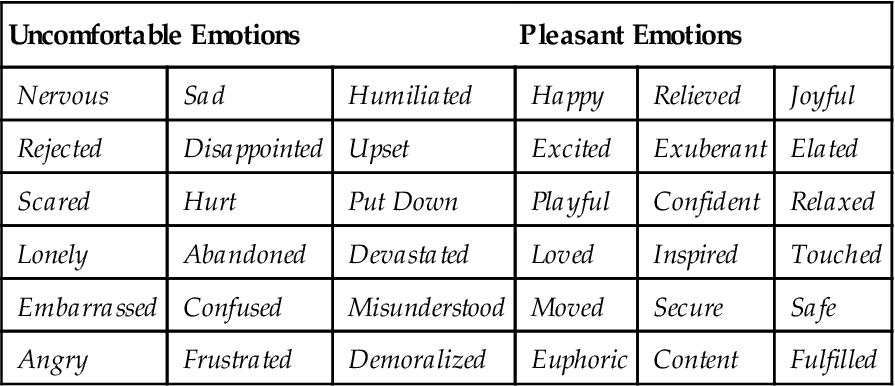
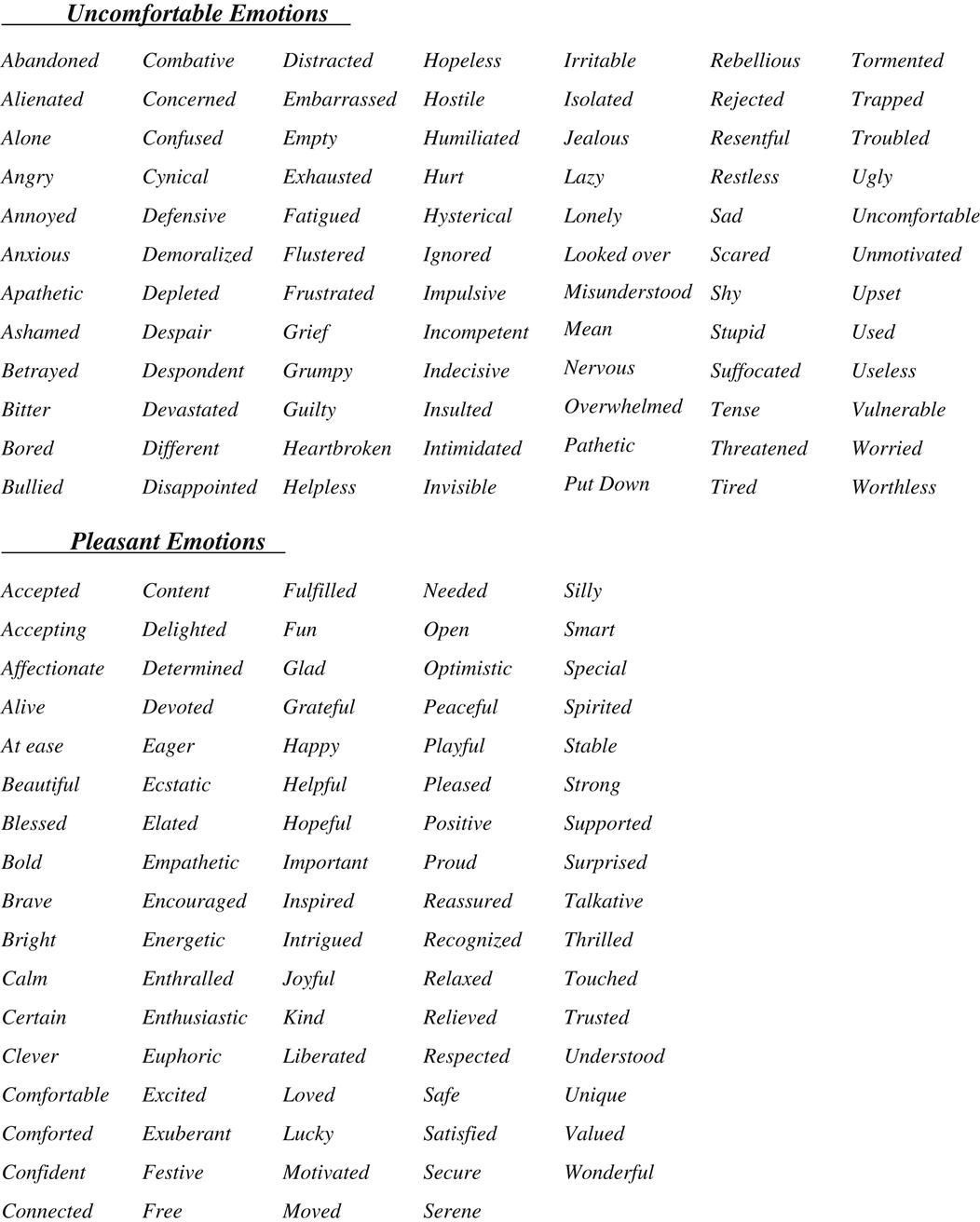
Reference the earlier point, that when feelings are aptly labeled and discussed, they can be understood and effectively managed, and then invite the group to brainstorm a list of feeling words, which can be written on a dry erase board. Point out that parents have an opportunity to support their teens, by modeling the appropriate labeling and verbal expression of feelings. Let them know that youth who are prone to act out feelings, in unproductive or even destructive ways, are likely to have impoverished feelings vocabularies and maybe inadequate words to describe emotions. Again, remind the parents to distinguish feelings from physical or physiological states, such as “hyper,” “tired,” or “sore.” Additionally, help them discern the difference between feelings and thoughts, perceptions or judgments. For example, parents might endorse feeling as though “my family situation is hopeless,” when asked to reflect upon their feelings, although that statement is more representative of a thought or viewpoint, rather than indicative of an emotion or feeling state. The term “hopeless” by itself could represent a feeling state, but not when used as a descriptor referencing a family situation. It is helpful to have the caregivers initially focus on more positive or pleasant emotions and then switch and instead brainstorm another list comprised of more uncomfortable or unpleasant ones. The lists generated, which can be subsequently augmented via input from the therapists, might resemble those that follow:
| Uncomfortable Emotions | Pleasant Emotions | ||||
| Nervous | Sad | Humiliated | Happy | Relieved | Joyful |
| Rejected | Disappointed | Upset | Excited | Exuberant | Elated |
| Scared | Hurt | Put Down | Playful | Confident | Relaxed |
| Lonely | Abandoned | Devastated | Loved | Inspired | Touched |
| Embarrassed | Confused | Misunderstood | Moved | Secure | Safe |
| Angry | Frustrated | Demoralized | Euphoric | Content | Fulfilled |
Feeling Intensities
Have the group define intensity of feelings, which can be summarized as how little or how much you feel a feeling. Introduce the group to a scale, 0–10, and invite them to begin routinely noting their feelings, as well as assigning an intensity percentile.
Feelings Identification and Somatic Monitoring
Ask the parents to take turns identifying and relating their top two or three most uncomfortable, difficult, or distressing feelings and why they tend to cause problems in their lives. Encourage parents to identify warning signs for their emotions to include physiologic or bodily sensations as well as behavior changes or signs observable by others that indicate they are experiencing that particular emotion. Questions such as the following may be posed, to generate fruitful discussion:
How do you know you are experiencing that particular emotion?
How do you differentiate between feeling anxious versus feeling excited? (This is an example of a question used because the two feelings can physically be similar.)
Where in your body do you feel sadness (hurt, anger, etc.)?
How do you know you are becoming sad (hurt, angry, etc.)?
How would you describe the sensation of feeling sad (hurt, angry, etc.)?
What changes do you notice in your body, when you begin to feel sad (hurt, angry, etc.)?
Some examples of physical sensations or bodily effects noted, in association with various feelings include the following list:
Differentiate between physiological changes, such as the list above, versus behavioral warning signs which might include:
Facilitate discussion regarding the mind–body connection and help the group recognize regarding that there are physiological and bodily reactions that typically accompany all emotions, which can vary between individuals. Help the parents appreciate the value of identifying and attending to their bodily and behavioral warning signals, as early as possible, related to impending and escalating feeling states. Guide them to recognize the window of opportunity for self-soothing and coping that can be leveraged, before impulsive or harmful responses take over. Stimulate discussion with the group regarding the fact that many people find it difficult to deescalate their feelings and emotional reactions before they act out in some manner (again, the normalizing thing works really well). The goal is to learn to be proactive in identifying their own triggers and bodily signals and attenuate them early. As youngsters, along with their family members, become more tuned into their body signals, they can become better at taking care of themselves and dealing with their difficult emotions and the precipitants before they react impulsively in a manner they might regret. Again reiterate the point, that role-modeling healthy, pro-social behaviors, is often the powerful intervention parents can offer, in support of promoting emotional and behavioral health in their teens.
“Fight-or-Flight” Responsea
Generate discussion regarding the phenomenon of fight or flight. Encourage the parents to discuss what they know about the phenomenon of the fight-or-flight response and its origins.
The response consists of elevated arousal; increased heart rate, pulse, and breathing; increased strength in large skeletal muscles; and shifting into a highly instinctive, primitive state of mind (residing in the amgdala) that is bent on survival. Blood rushes to the major vital organs including the heart and lungs and to large skeletal muscles but notably away from the frontal lobes and rational decision-making parts of the brain (prefrontal cortex). The body is deliberately routing all resources, that is, blood flow to only the most vital, life-sustaining areas, of which the frontal lobes is not one.
Thus, a person experiencing a fight-or-flight response might feel dizzy, lightheaded, or confused. This response is a vestige of cavemen times, when early man had to be on guard and have the capacity to launch instantly into a physical state in which he was prepared to run away or fight when faced by that saber-toothed tiger or wooly mammoth. Ask the caregivers “What happens to people when they feel threatened or experience the fight-or-flight response?” and write down the ideas they generate on the dry erase board. The list may ultimately resemble the following:
Increased blood flow to large organs
Increased blood flow to large skeletal muscles
Facilitate discussion with the parents regarding the fact that arousal states (along with most emotional states)—as most people know and have experienced—are usually contagious. That, too, probably conferred early evolutionary advantage and so has been preserved in the species. It is rare, however, that the fight-or-flight response is apropos in modern society. People no longer face saber-toothed tigers or their modern-day equivalent. Discuss with parents, that, unfortunately, many youngsters are sensitized to enter this high-arousal state with minimal provocation. Their central nervous system wiring is functioning as though “short-circuited” and vulnerable to misfiring out of cue. In fact, there is a burgeoning body of literature, growing out of functional brain imaging studies, that is amassing evidence demonstrating a pattern of amygdala hyperactivation (emotion) coupled with prefrontal cortex and anterior cingulate (rational decision-making) hypoactivation, in adults and youngsters with anxiety and mood disorders (Wegbreit, Cushman, Puzia, et al., 2014). This robust scientific finding can help answer parental inquiry as to “Why is my child/teen struggling with emotional regulation?” Caregivers can likewise become sensitized to activation of their own threat or “fight-or-flight” response; especially if they have a long history of managing frequent escalations in their teens. In short, both their teens’ and their own arousal system can become “twitchy” and prone to firing and misfiring, akin to a “hair-pin” trigger.
Greene (2001) suggests that youth lose at least 30 IQ points when they become hyperaroused. They become more primitive and less capable of rational, logical, reasonable thought and conversation. If their parents likewise become hyperaroused, it as though gasoline has been poured on a fire, with both parties operating in a primitive, low-intellect, aggressive state. Ask the parents to reflect on an instance during which they entered this high-adrenaline state themselves. Encourage them to recollect the event in vivid detail and to share highlights with the workshop. Ask, “When highly aroused, what becomes of one’s ability to think clearly, to reason, to negotiate, or to problem-solve?” A hyperaroused person loses much of his or her capacity for rational thought along with 30 IQ points and instead becomes braced for action, either defending against or evading danger, a primitive being. Their higher-level brain functions shut down, leaving only the most primitive part of the brain engaged and functional. You might orient the group to reference the psychological mindset of a threatened individual as being controlled by their “savage” brain (amygdala) which is more powerful but much dumber than their “civilized” brain (frontal lobes or prefrontal cortex). The former is comprised purely of brute force, but lacking intellect and capacity for reason. The latter brain regions are admittedly less powerful, but much more intelligent, effective, sophisticated, and mature.
Threat in Eye of Beholder
The point should be made that often adolescents who are becoming increasingly agitated genuinely feel threatened, even when others do not perceive an obvious or significant threat. Nonetheless, youth who are dysregulated tend to adopt a defensive or aggressive posture and behave as though they are under attack. Often, their brains inadvertently extrude large amounts of adrenaline, which heightens physiological arousal and in turn activates a mindset of defensiveness or aggression. Parents and other adults who are attempting to deescalate such a teen or prevent an escalation can behave in a manner that makes them unlikely to be perceived as a threat. Essentially, parents can present themselves as soft, vulnerable, and allied with the teen, causing the teen to deescalate more readily and become increasingly open, flexible, and cooperative. “Business cards” summarizing the steps for lowering arousal can be handed out now or at sessions’ end. These are available at the end of the bulleted outline for this module, as well as in the Therapist’s Toolbox on the book’s companion website.
Lowering Arousal
Contagiousness of Feelings
Suggest to parents that the plan for the remainder of the session is to focus on exploring techniques for coping with heightened arousal states in youngsters. However, prior to learning to cope with their teen’s heightened states of arousal, parents must become skilled at lowering and controlling their own arousal and behavioral responses to distress. Facilitate a discussion regarding the contagious nature of arousal and of feelings in general. It is easy and natural to laugh and joke when in the midst of playful, jovial company. Likewise, when in the presence of individuals who are agitated, irritable, angry, furious, or out of control, it is hard not to be affected and to avoid reacting in concert. This natural tendency is amplified in instances of parents witnessing their children experiencing and expressing intense feelings. Furthermore, if parents have teens who have been impulsive, dysregulated, and prone to explosive and aggressive outbursts, they may have become highly “sensitized” to their youngster’s emotional reactivity. Essentially, they may have heightened “anticipatory” anxiety in response to their teen’s upset and both parent and teen may be wired to escalate especially rapidly, with minimal triggers, as a programmed reaction to one another’s cues and provocative behaviors or remarks.
Cue discussion around the typical sequence of events and interactional patterns that occur between any two people, who are at odds, when one or both of them is upset, angry, frustrated, anxious, or experiencing some other negative emotion or mix of feelings. Inevitably, the communication degenerates and becomes not only unproductive, but often hurtful or even menacing. No conflict or problem can be addressed in a creative, collaborative and productive manner unless both parties are totally or at least mostly calm, open, and receptive. The rule of thumb needs to be that one should only confront a conflict when calm. There is a vast body of literature, encompassing a broad range of patient populations and treatment options that demonstrates that “Expressed Emotion,” or aggressive, critical, and hostile communication, negatively correlated with outcomes. In other words, emotionally charged relational patterns make patients do worse and confer increased risk of poor outcomes, whereas the absence of expressed negative emotions promotes treatment progress and protects against relapse (Han & Shaffer, 2014; Miklowitz et al., 2009).
Enmeshment
Highlight the fact that some parents are overly emotionally connected to their own adolescents, sometimes even to an unhealthy, extreme degree. This dynamic, termed enmeshment, results in a tendency for the identities and feelings of parents and their teens to fuse. Short of being enmeshed, many parents are naturally extremely tuned in to their youngster’s affective states. Some parents note each facial grimace, frown, furrowed brow, evil eye, and fist of fury. Because of this strong emotional attunement parents have with their teens, parents often assume and begin directly experiencing similar feeling states when in their midst. This applies especially when youngsters are distressed or highly agitated. It is hard for parents to tolerate witnessing their adolescents in distress because they, too, feel it deeply and feel obligated to do whatever they can to assuage their teen’s painful feelings.
Interrupting Cycles of Arousal Escalation
Ask parents to reflect upon and share specific experiences along these lines. They may recall how unbearable it was to observe their adolescents in psychic pain. If a youngster is angry, especially if his or her anger is directed toward the parent, the feelings between the two tend to fuse. The parent–teen dyad of the reciprocal cycle of anger tends to fuel itself like gasoline poured on a flame. The teen’s escalation leads to the parent’s escalation, which leads to further teen escalation, which leads to further parent escalation, and so on and so forth. Ask the group, “How can parents interrupt the cycle? How can you resist these natural, instinctual tendencies for your feelings to fuse with those of your teens?” This reaction is hard-wired, a vestige of early man; clearly, it once conferred evolutionary advantage to have been preserved all these years. Educate parents that they can actually resist this tendency and reverse nature, at least within themselves.
Share with the group that mental health providers routinely train themselves to step back, disconnect, and safeguard against assuming the emotional states of their patients. When a client becomes agitated or despondent, it is not that the therapist becomes cold and does not care; however, to be empathic and helpful to their clients, therapists must retain a reasonable level of affective control within themselves. If clients shout or cry, therapists know better than to follow suit. It would be ridiculous and also render the therapist incapable of helping and stabilizing the client.
Through didactic discussion, help parents recognize the counterintuitive reality that a person is best able to understand, validate another’s feelings, and be supportive, if he or she can remain somewhat objective, rational, and calm. Encourage parents to try to understand and validate their adolescent’s feelings but to avoid taking them on as their own. Teach parents to emotionally disconnect a bit if their teens are overwhelmed so that they can adopt a reasonable approach that will be helpful and supportive.
Nonverbal Calming Techniques
At this point, move to fostering a discussion of nonverbal techniques or behaviors for lowering arousal. Have the parents brainstorm and see whether they can identify the following actions that are typically useful in this regard:
Controlling breathing (slow, deep, abdominal breaths)
Assuming a nonthreatening body posture (facing the person with palms showing and open).
In addition, parents can depict themselves as nonthreatening by crouching down and attempting to minimize their size while speaking softly and slowly. Sometimes whispering will distract and disarm youth who are becoming distressed. Whispering and calm behavior tend to be contagious in the same way that agitation can be contagious. Parents often admit that they struggle to control their own arousal when facing off with their distressed or agitated teen. They are encouraged to “fake it until they make it,” that is, to pretend to be calm and strive to act accordingly until they are genuinely able to remain relaxed, even if their teen is distressed. Parents will discover that if they master the ability to at least present outwardly as calm, they will ultimately achieve a state of genuine calmness. In other words, acting calmly lowers arousal within a person behaving as such and leads to actual calmness in self and others.
“Taming Bambi” Metaphor
Share with the group that forging trusting and empathic connections with adolescents is akin to “Taming Bambi.” Adolescents tend to be defensive and mistrustful in their baseline posture toward the world, especially adults and most particularly in reference to their parents. The level of reactivity and mistrust teen’s harbor often increases exponentially relative to the extent of a legacy of escalating parent–teen conflict and acting out behaviors, which tends to proceed and precipitate entry into treatment. Encourage parents to consider the steps necessary to build trust with a wild animal, especially one prone to flightiness, and exaggerated startle response, such as a deer. Bambi is unlikely to initiate a connection with a human, and initially unlikely to accept attempts by a human to encroach. Humans must find ways to entice Bambi to venture closely and he will do so, only at his own pace, on his own terms. One false or sudden move by the human will send Bambi running rapidly for the hills, and if the breach in trust is too great, he might never return.
Parents must tread ever so delicately and ensure they are offering something that is especially incentivizing to their teens, to facilitate overcoming their natural instinct to flee. If parents attempt to forge relations and communications with teens in an overly aggressive or abrupt fashion, they may burn bridges beyond repair. They must outreach teens gingerly, mindful of the reactivity and flightiness to which they are prone, putting out crumbs delicately and then backing off sufficiently, such that their easily triggered teens can slowly but surely accrue comfort and trust, at a pace they control. In the likely event, in the case of a teen presenting for psychiatric treatment, that there has been intense and chronic parent–teen conflict and patterns of hostile communication, the parent is at an even greater disadvantage, where they are essentially starting from a deficit position, in building trust with their teen. This situation would be akin to a human attempting to encroach upon and make contact with a Bambi who had been treated aggressively by a human in the past, or specifically that very person now attempting to mend the bond between parent and deer (or teen).
“What About My Teen?” Examples
After covering each major topic, it is worthwhile for the facilitators to pause and invite some brief discussion regarding specific examples or applications of the material or skills covered as they relate to the teen for who they are attending treatment. Invite parents and caregivers to share examples of actual experiences with their youngsters and take turns role-playing instances of conflict while attempting to lower their own arousal as well as their teens’.
Feelings Triggers
Invite the group to recall examples of past experiences involving uncomfortable feelings and elaborate upon the circumstances under which those emotions were elicited. As individual parents share examples, inevitably their peers will identify and point out parallels from their own lives. Encourage the caregivers to especially reflect on what kinds of events set them off. Through didactic discussion, make the point that every individual will perceive the same situation differently and that different things make different people angry. It is very common for adolescents to identify interpersonal stressors as their most common and intense trigger for intense distress. Teens especially are prone to becoming overly dependent upon validation from peers for self-worth, as well as prone to failing to preserve their own definition of self as separate and distinct from others. Hence loss of friends or romantic break ups can trigger catastrophic reactions in adolescents who are left feeling empty, worthless, and devastated. Similarly, teens with ill-defined identities are likewise vulnerable to disintegrating emotionally in the face of intense conflict and verbal assaults, laden with derogatory labels and put downs, from family members, including parents and siblings. That finding is often associated with difficulties in maintaining healthy and balanced interpersonal boundaries, as detailed in the next section.
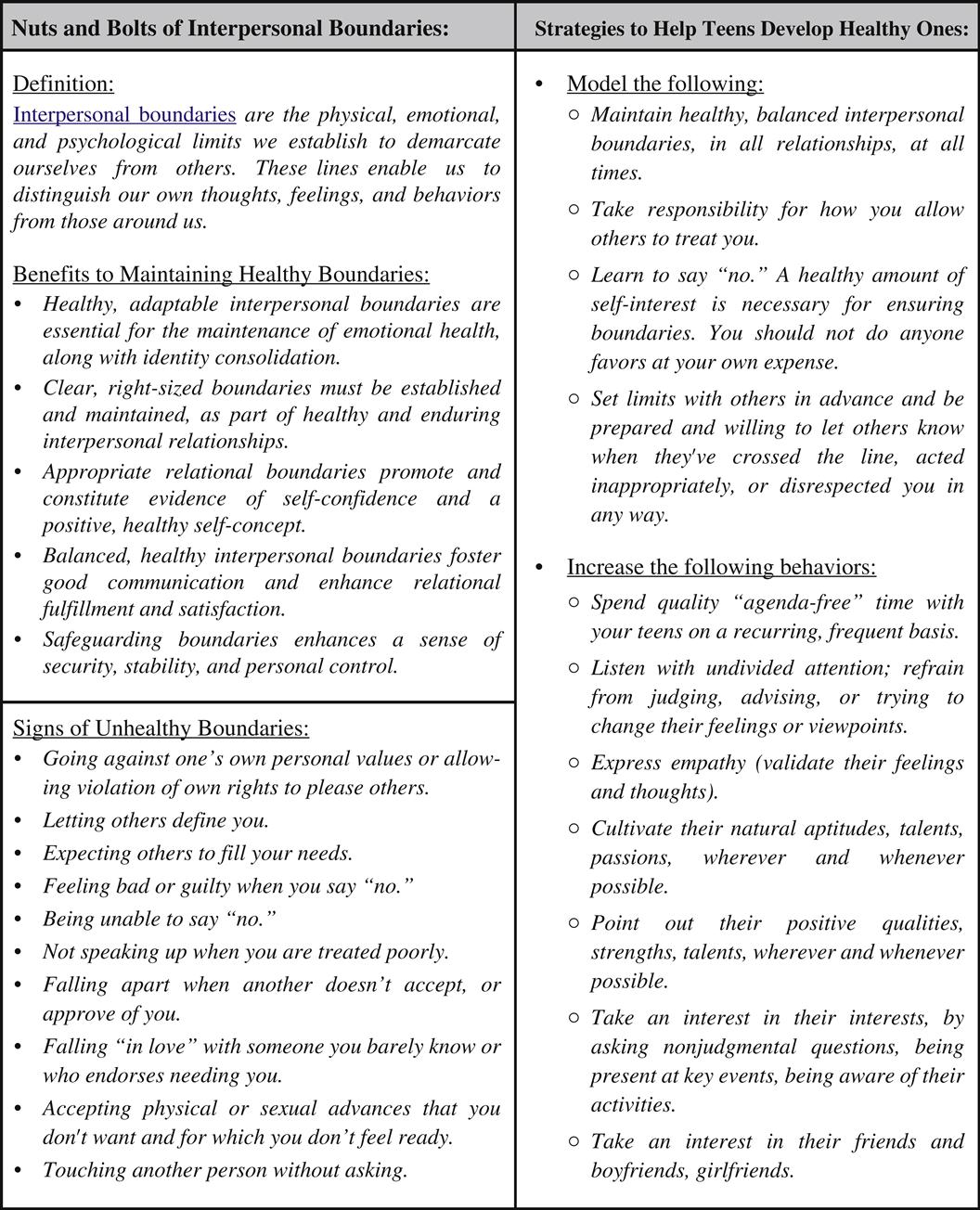
Interpersonal Boundaries
It is well established, that the most salient and critical developmental task of normal adolescence is identity consolidation, most especially in regards to defining oneself, in relation to others (Stiles & Raney, 2004). Typically developing teens shift their focus and prioritization of interpersonal relationships from parent–child to peer–peer (Flannery, Torquati, & Lindemeier, 1994). Within this context of heavy reliance upon peer acceptance and relationships, a fundamental interpersonal skill must be honed, pertaining to the capacity to healthily balance forging positive connections with peers with psychological autonomy (Scott & Dumas, 1995). The case has been made, via a significant body of literature that interpersonal boundaries that fall toward the extreme ends of the spectrum, ranging from extremely open to totally closed, are problematic and contribute to maladaptive social and psychological development, as well as fuel emotional and behavioral struggles (Peck, 1997).
Many teens, who have had difficulty making and keeping friends and/or have been embroiled in intense and chronic family conflicts, are relatively inept at managing interpersonal boundaries. They often exhibit patterns of rushing hastily into relationships at mock speed, in an intense, forceful, and emotionally dependent manner, characteristically revealing their whole life story at a first meeting, or instead refuse to open themselves up to engaging even superficially with peers.
Stimulate a discussion with the group about interpersonal boundaries. Invite them to define that term, as well as define the terms “identity formation” and “sense of self.” Ask them to ponder extremes of interpersonal styles, ranging from extreme openness, on the one hand, contrasted with extreme withdrawal and impenetrability, on the other. Ask them for examples of experiences wherein they observed interpersonal boundaries that were too loose, or fluid. Guide them to recognize the pitfalls and dangers inherent in maintaining relationship boundaries that are too diffuse, whereby one individual loses their distinct identity or sense of self and instead merges or becomes “enmeshed” with another individual. Diffuse boundaries can be seen in any relationship including inside professional situations, families, friendships, and romances. Ask them to reflect upon experiences wherein they observed an unhealthy degree of interpersonal walling off or impenetrability and invite them to consider and discuss potential risks inherent to that extreme style of relating.
Facilitate discussion around the value of striking a balance between remaining separate and distinct, psychologically, from others, versus allowing one’s definition of self and self-worth to be utterly dependent on feedback from others. Provide psycho-education regarding what is known in reference to optimal adolescent psychological development and social success, that is, that flexible and balanced interpersonal boundaries promote well-being and healthy relationships. Make the point that the capacity to define oneself is in part contingent upon one’s capacity to form relationships with others, wherein a connection develops, but at the same time, both individuals retain their distinct and separate identities. Invite parents to share specific examples regarding interpersonal struggles they’ve witnessed in their adolescents and brainstorm options for promoting healthy and flexible interpersonal boundaries. Examples of parenting strategies for promoting appropriate interpersonal boundaries and consolidation of identity or sense of self in their teens include the following:
• Modeling flexible, healthy, and balanced interpersonal boundaries, in all relationships, at all times.
• Spending quality time with your teens on a recurring, frequent basis.
• Listening with undivided attention and refraining from judging, advising or trying to change their feelings or viewpoints.
• Expressing empathy (validating their feelings and thoughts).
• Cultivating their natural aptitudes, talents, passions, wherever and whenever possible.
• Pointing out their positive qualities, strengths, talents, wherever and whenever possible.
• Taking an interest in their interests, by asking questions, being present at key events, being aware of activities.
• Taking an interest in their friends and boyfriends/girlfriends.
“What About My Teen?”
After covering each major topic, it is worthwhile to pause and invite some brief discussion regarding specific examples or applications of the material or skills covered as related to the adolescent for whom the parents are attending treatment. The parents and caregivers might be asked to provide an example or two of instances during which they understood their teen’s unhealthy behavior to be the function of a mismatch between developmental level or capabilities and environmental demands.
Family Homework
As a homework assignment, ask the group to pay attention to their bodily signals of emotions and take note of their triggers and warning signs during the subsequent week. They should also be provided with the treatment goal and family crisis plan worksheets and directed to complete them, prior to the next session. Additionally, encourage the parents to schedule family meals, at least once weekly, where all members gather at a table and each person takes a turn, sharing the best and worst parts of their day to model and facilitate practice of conversation and listening skills.
Joint Session for Module 1
As described in detail, in the format and operations section, parents and teens are brought together, once a week, in reference to each Module set, for the sake of discussing and practicing the skill sets that were initially introduced and rehearsed separately. At the start of the “Joint” session for PACK-Teen and MaPS-Teen Module 1, hand out the “Family Strengths and Goals” interview worksheets, which were designed to promote further contemplation and discussion of each family’s strengths and goals. Teens are invited to “swap” parents with another teen and partner with parents, who are not their own. Teens take turns with parents; alternately interviewing one another, using the interview questions outlined in the “family strengths and goals” interviews, with slightly different versions available for parents versus teens. Handouts are available containing the interviews to cue the participants, as well as provide a mechanism for writing down answers, to serve as later reminders while reporting results. A slightly different version of the handout is available for teens to interview parents than the one intended for parents to interview teens.
Advise the teens and parents to jot down answers, as they move through the interview. Cue them to demonstrate exceptional listening skills, by maintaining consistent eye contact, staying focused, and tracking their partners’ responses closely. They are encouraged to demonstrate that they are interested in hearing what the speaker has to say by using facial expressions, body language, tone of voice, and responding empathically. After all parties have completed their interviews, cue the larger group to come back together and have the teens and parents take turns presenting the information gleaned from their interviews.
As the reporting wraps up, ask the group to reflect upon their thoughts, feelings, and observations related to the exercise and information shared. Facilitate discussion regarding common themes that emerged and invite comments regarding any insights that were derived or experienced as surprising. Also reflect upon the purpose of the exercise, including explaining the importance of identifying individual and family strengths. Often, individuals tend to focus on aspects of a relationship or situation that are not going the way they would like. Ironically, it is often more difficult and counterintuitive to consider and point out aspects that are going well. As they progress through treatment and beyond, encourage families to focus just as much on strengths and victories, as they do on challenges. Also explain the importance of setting individual and family goals, that are realistic and relevant, as well as formulating plans to achieve them. Encourage families to set aside some time periodically to discuss how they are doing with the fulfillment of their family goals. If they find that they aren’t progressing as they would like, encourage them to identify a different plan.
Read the excerpt from Michael Riera’s book aloud, as it appears on the parent handout during the final 5 minutes of the joint group session, before adjourning and dismissing the group.
PACK-Teen Module 1 Summary Outline
Materials needed
Established Parent Introductions and Check-Ins
• Have the introduction and check-in format for new versus established parents written on the board.
• Go around the room and have each established parent take turns doing the following:
• Ask each parent to identify themselves by first name.
• Ask each parent to mention their teen’s first name.
• Ask each new parent to mention one “victory” or success (required) and “challenge” (optional), from the past week, related to their teen.
• If there are new parents, invite each established parent to help in orienting the new parents to the workshop format and guidelines.
• Established parents may check in regarding their family progress, including approaches they tried which were effective thus far.
Workshop Guidelines
• Workshop consistently starts on time and finishes on time, punctuality required, leaving early or stepping out of workshop during session, not allowed.
• Confidentiality required, “What is said in here, stays in here,” playfully termed the “Vegas Rule.”
• Refrain from developing personal relationships with other patients while in program.
• Exceptions are safety issues (suicidality, homicidality, violence, abuse/neglect).
• All cell phones, pagers, electronics of any kind must be turned off during group.
New Parent Introductions and Check-Ins
• Have the introduction and check-in format written on the board.
• Take turns having each parent introduce themselves and check in as follows:
• Ask each parent to identify themselves by first name.
• Ask each new parent to mention one positive feature or strength of their adolescent and mention one “challenging behavior” they’d like to focus on.
• Ask established parents to relate commonalities noted during new parent check-ins.
New Parent Orientation
Review
Treatment Goals: Individual and Family
Feelings: Good, Bad, and Ugly
Feelings Overview
• Generate broad discussion of feelings.
• What are feelings? Are they important? Whose are important?
• What feelings “get them in trouble?”
• What is the purpose of feelings?
• Encourage the parents not to ignore their feelings, and remind them that emotions serve a purpose. Share that it does not make you a bad person if you have anger; it’s what you do with the feeling that counts.
• Ask the parents, “Is it ever a good thing to be angry about something?” May also provide the group with examples of anger that is put to good use. For example, a parent getting angry over how a bully is treating someone and deciding to tell the administrator so that it stops is a positive result of anger.
Ambivalence or Mixed Feelings
Feelings Vocabulary and Intensities
• Invite discussion and brainstorm regarding negative or uncomfortable feelings. Generate list on whiteboard such as the one that follows:
| Nervous | Sad | Humiliated | Rejected | Disappointed | Upset |
| Scared | Hurt | Put Down | Lonely | Abandoned | Devastated |
| Embarrassed | Confused | Misunderstood | Angry | Frustrated | Demoralized |

• Assist parents in distinguishing feelings from thoughts or perceptions/judgments.
• Have the group define intensity of feelings, which can be summarized as how little or how much you feel a feeling, introduce a rating scale, based on percentage 0–100.
• Ask, “Are emotions good or bad?”
• Help parents realize that emotions are not “good” or “bad,” they are natural and serve important functions.
• Discuss if behavioral responses to emotions can be “good” or “bad.”
• Ask, “Can more than one emotion or even seemingly conflicting emotions be experienced at the same time?”
• Discuss ambivalence and reiterate that this mixture of emotions is often the case.
Feeling Identification and Somatic Monitoring
• Invite the group to reflect upon and discuss the various bodily signals and sensations they have experienced, associated with various feelings.
• Where in your body do you feel sadness (hurt, anger, etc.)?
• How do you know you are becoming sad (hurt, angry, etc.)?
• How would you describe the sensation of feeling sad (hurt, angry, etc.)?
• What changes do you notice in your body, when you begin to feel sad (hurt, angry, etc.)?
• Choose two or three feelings as examples and generate lists on the whiteboard, as the parents share examples.
• Some examples of physical sensations noted, in association with various feelings include the following list:
• “I feel sick to my stomach.”
• Discuss mind–body connection and guide group to recognize the value of attending to early bodily signals, especially for anger.
“Fight-or-Flight” Response
• Generate discussion about the “fight-or-flight” response. Discuss its origin and purpose as well as the physiological or physical changes associated with it (turn off frontal lobes).
• Make a point about contagiousness of feelings and discuss the phenomenon of “sensitization” whereby escalation can become more automated, and more rapid, if hostile exchanges have become a pattern.
• Orient group to terms “Savage” brain (amygdala, brainstem) versus “Civilized” brain (prefrontal cortex, frontal lobes)—one all brute force, no intellect or reason—the other less powerful, but much, much more intelligent, effective, and mature!
Discuss Contagiousness of Feelings and Enmeshment
Discuss Cycles of Arousal Escalation
• When a defiant, defensive adolescent (or a teen with psychosocial impairments or difficult temperament) hears “No,” “You can’t,” or “You must” or feels boxed in or controlled, a power struggle or meltdown is imminent.
• Recognize that fear is usually under or behind anger. Anger and anxiety go together. Essentially, one might react with hostility when he or she feels threatened. The threat does not have to be rational or realistic; it’s the perception of threat that matters.
• When a teen or parent becomes “aroused” or feels threatened in some way, he or she experiences an adrenaline response “fight or flight”—accompanied by physical symptoms of arousal and/or anxiety, including increased heart rate, increased respiratory rate, dizziness, and lightheadedness. This is because blood rushes away from the brain to the large skeletal muscles, heart, and lungs.
• One’s capacity for rational thought disappears when one is furious and/or upset.
• When aroused, humans are evolutionally programmed to fight or run away. We tune out the sound of the human voice and instead tune in to the frequency of large predators or other threats. When angry, your teen literally cannot hear you.
• As a parent becomes aroused in response to the teen’s arousal (parent is emotionally connected to teen, and the teen knows how to push the parent’s buttons), the parent’s arousal only further fuels the teen’s arousal, resulting in a vicious cycle of escalating emotions. Because of this long-standing cycle, the parent and teen essentially are both sensitized or programmed to react automatically when faced with certain cues (e.g., “No,” “You can’t,” “You must”).
Discuss Nonverbal Techniques for Lowering Arousal
• Lower your own arousal—quiet your voice, control your breathing, use a gentle tone of voice, and assume a nonthreatening body posture (same techniques psychiatrists use with agitated patients).
• In other words, when you child goes up, you go down. Model the regulation of affect and appropriate expression of anger.
• Use relaxation training (hand out and discuss relaxation training scripts, located on the book’s companion website as PACK-Teen, Module 1, Handout 1).
Summary of Calming Steps
• The steps for calming down a distressed child can be summarized as follows:
• Calm yourself (“fake it until you make it”).
• Lower your voice (speak slowly and softly; whisper).
• Crouch down (make body appear small).
• Display empathy (use formulas).
• Use mirroring (covered in next module).
• “Business cards” outlining these calming steps are available digitally in the PACK-Teen Therapist’s Toolbox on the book’s companion website. These cards can be cut out and handed to parents to serve as reminders during the workshop as well as at home.
Review “Threat” (i.e., “Fight or Flight”) Response
“Taming Bambi” Metaphor
• Introduce the idea that empathically connecting with teens is akin to “Taming Bambi.”
• Teens must feel as though they control pace and manner.
• Parents should be mindful on offering incentives “crumbs” that are powerful, such that teens are compelled to approach.
• One false or sudden move experienced as threatening to teens, can send them running for the hills, so gentle and delicate approach, alternating with sufficient backing off, is key.
Feeling Triggers
Interpersonal Boundaries
• Facilitate discussion around the notion of interpersonal boundaries including inviting a definition of the term.
• Cue the group to reflect upon the value of striking a balance between remaining separate and distinct, psychologically, from others, versus allowing one’s definition of self and self-worth to be utterly dependent on feedback from others.
• Provide psycho-education regarding what is known in reference to optimal adolescent psychological development and social success, that is, that flexible and balanced interpersonal boundaries promote well-being and healthy relationships.
• Invite the group to share specific examples of interpersonal struggles they’ve witnessed in their adolescents.
• Brainstorm with the group options for promoting healthy and flexible interpersonal boundaries in their teens.
• Modeling flexible, healthy, and balanced interpersonal boundaries, in all relationships, at all times.
• Spending quality time, with your teens on a recurring, frequent basis.
• Listening with undivided attention and refraining from judging, advising or trying to change their feelings or viewpoints
• Expressing empathy (validating their feelings and thoughts)
• Cultivating their natural aptitudes, talents, passions, wherever and whenever possible
• Pointing out their positive qualities, strengths, talents, wherever and whenever possible
• Taking an interest in their interests, by asking questions, being present at key events, and aware of their activities
• Taking an interest in their friends and boyfriends, or girlfriends.
PACK-Teen Mantras
What About My Teen?” Examples
Family Homework
• As a homework assignment, ask the group to pay attention to their bodily signals of anger and take note of their anger triggers, during the subsequent week.
• The parents are encouraged to schedule family meals, at least weekly, where all members gather at a table and each person takes a turn, sharing the best and worst parts of their day, to model and facilitate practice, of conversation and listening skills.
Wrap Up and Answer Questions
Joint Session Ideas for Module 1
• Complete Family Strengths and Goals Interview:
• Teens “swap” parents and join with parents who are not their own.
• Both parties interview each other using the attached interview questions.
• Parents and teens report back to the group about what they learned about one another. Ask about thoughts and observations from the group.
• Facilitate discussion regarding common themes. Also discuss the purpose of the exercise. Explain the importance of being able to identify strengths.
• Encourage families to focus just as much on strengths as they do on challenges. Also explain importance of setting goals as well as having a plan to carry them out.
• Encourage families to set aside some time periodically in order to discuss how they are doing with fulfilling their family goals.
• Read excerpt from Michael Riera’s book aloud, as it appears in the parent handout, during last 5 minutes of session, before adjourning and dismissing the group.
Handouts/Business Cards
Module 1-PACK Parent Workbook Cover
Module 1-PACK-Teen Handout #1
Module 1-PACK-Teen Handout #2
Module 1-PACK-Teen Parent Handout #3
Module 1-PACK-Teen Parent Handout #4
Module 1-PACK-Teen Mantra Cards Therapist Tool #1

Module1-PACK-Teen Parent Handout #5
Family Strengths and Goals Interview: Parent Version
Directions: Pair with a teen from another family and alternate asking and answering questions with them, until the interviews have been completed. Write down answers as you go, and prepare to share the responses, with the group, when the interviews are done.
Parents Ask Teens (paired with teen from another family):
1. What is your favorite feature of your family?
2. What is something your parent does really well?
3. What works really well in your family?
4. What is something you wish you could change about your family?
5. What is something you wish you could change about yourself?
6. Describe a favorite memory of a time with your family.
7. Share three activities (you think your family would be willing to do), that you would like to do with your family.
8. What would you be willing to do, to improve your family relationships or help in achieving your family goals?
Module 1-PACK-Teen Parent Handout #6
Parenting Adolescents:
The following passage by author Michael Riera (2012) was excerpted with permission from Uncommon Sense for Parents with Teenagers, Third Edition:
Until this point, you have acted as a “manager” in your child’s life: arranging rides and doctor appointments, planning outside or weekend activities, helping with and checking on homework. You stay closely informed about school life and you are usually the first person your child seeks out with big questions. Suddenly, none of this is applicable. Without notification, and without consensus, you are fired from the role of manager. Now you must scramble and re-strategize; if you are to have meaningful influence in your teenager’s life through adolescence and beyond, then you must work your tail off to get rehired as a consultant.… As a consultant, you offer advice and give input about decisions when you are asked. Otherwise, you’ll lose your client. You don’t garner the automatic praise and admiration that you did earlier. And, when your client asks for advice, you need to make sure that she really wants it. Sometimes, more than anything else, she simply wants your reassurances that she’ll figure it out herself. Sometimes she will temporarily lose belief in herself and ask to borrow your belief in her for a short while. Offering advice is not helpful when the real problem is the teenager’s lost belief in herself. A rule of thumb is not to take your teenager’s request for advice too literally until the third time. Nobody wants a consultant who tries to take over the business. What you are doing is not doing—you are waiting, but not abandoning. As a consultant, you must also save your “power plays” for health and safety issues; everything else is negotiable on some level. Skipping a biology class is definitely not on a par with driving a car after drinking alcohol. Finally, at this stage in your relationship, you are no longer the focus of your child’s praise and admiration; rather, you are often the scapegoat for the confusion about what it is to be an adolescent. As a manager, you were quite content to take their feedback personally, as a reflection of you; as a consultant, you must learn to not take most of their feedback personally, since it is often more about them than about you.
PACK-Teen Module 2
Introductions, Check-Ins, Guidelines, and New Parent Orientation
Module 2 begins with introductions, and a review of group guidelines, as detailed above. Returning parents are invited to relate a “victory” (required) and “challenge” (optional) regarding an experience connected to their recent attempts with practicing skills covered in group. Parents are asked, on their first day, to share one strength and one challenge, related to their adolescent, rather than specific instances of experiences. Parents may receive a workbook, containing a complete set of parent worksheets and informational handouts, except for those related to homework, unless the facilitators have elected to handout worksheets individually, by module. Parents are provided a brief overview and orientation to the program, on their first day, to include discussion of the modular format, along with a brief overview of the syllabus. The schedule and topics for the day should be written on the dry erase board and a brief review of the latest topic is conducted, before new material is introduced.
Effective Coping Skills
Remind the parents of how powerfully they can influence their teens’ behavior, by modeling what they want to see. Reiterate the point that if teens (and they) can learn to recognize their distressing emotions early and identify patterns in the development of their emotions, then they can learn to manage their reactions and behave in a manner that leaves them feeling competent and empowered. Facilitate discussion regarding potential “effective coping skills” that are additionally healthy. Clarify what is meant by “effective.” Make the point that teens often mistakenly consider a coping skill effective only when the skill completely or greatly diminishes their current uncomfortable emotion. Explain to parents that a coping skill is considered “effective” if it decreases the intensity of the uncomfortable emotion by even a small degree (e.g., decreases anger from a “10” to an “8.5”). Reiterate that individuals don’t “think well” when their emotions are very intense and any factor that can reduce the intensity of an emotion is considered effective. Further explain that if anger is at an “8.5” versus a “10,” an individual is much more likely to manage their anger effectively than if it were a “10.”
Encourage the parents to share their current most effective, preferred, healthy coping skills with the group. Go around the circle and have each group member mention a healthy and potentially effective coping skill they have tried or would like to try. Organize the discussion by listing a series of categories of coping strategies on a dry erase board and cue the group to brainstorm ideas, one category at a time. Examples of broad categories of coping skills include, “Coping Using Your Senses,” “Coping Using Your Creativity,” “Coping Using Relaxation Exercises,” “Coping with Help from Others,” and “Coping Using Healthy Habits.”
The parents will typically indicate having tried an array of healthy, and unhealthy, as well as effective and ineffective coping strategies. Cue them to focus on approaches that were both healthy and effective, while jotting them down on the dry erase board, under the appropriate category heading. Examples might include working out, journaling, listening to music, emailing or talking to friends or family members, walking or performing yoga. Go around the circle a few times and conclude the discussion by presenting a comprehensive list of coping skills to the group, available as a handout on the book’s companion website. Pause for a few minutes for the group to look over the list and then hand out the worksheet titled, “Effective Coping Plan.” Provide pens or pencils and allow the parents to take a few minutes to complete the worksheet. Invite the group to share “popcorn” and style their ideas generated via the worksheet completion exercise and any plans for implementing coping strategies.
Encourage the group members to practice several of these skills, at home, and then rate their effectiveness (scale of 1–10) during the subsequent week. Explain to the parents that it is important to set aside time each day to “practice” their most effective coping skills or to try new ones. You can inform them that the teens too, are being encouraged to develop similar habits. This habit of daily rehearsal of coping exercises, not only serves as a preventative measure (e.g., their emotions are less likely to reach their peak intensity if they listen to relaxing music three times per day), but also increases the likelihood that they will be able and inclined to utilize the skills when they actually need them. If an individual practices some form of relaxation or healthy coping skills daily, even for only 10–15 minutes, over the course of a few weeks, they can achieve something called the “generalization response” (Bournes, 2005) whereby they reset their baseline level of arousal at a lower level, hence increasing the threshold for triggering agitation, a temper outburst, or a threat response.
If they (or their teens) don’t rehearse relaxation and coping skills, while they are “cool-headed” and experiencing low levels of arousal, they won’t master the techniques to the degree necessary, to deploy them during episodes of intense distress or heightened arousal. A useful metaphor to share is the idea of trying to teach someone to tie their shoes, when the building is on fire. To effectively tie one’s shoes, in the context of attempting to evacuate a building on fire, one must have mastered the skill to the point that no thinking is required and the task can be done automatically and reflexively. The primitive, survival portion of the brain is taking over, fueling physiological arousal and the skills needed in the heat of the moment must be hard-wired and second nature. The same principle is at play with being able to call up relaxation and coping skills, when in the midst of heightened arousal or intense distress. The parents must know the techniques “cold” and be adept at performing them effortlessly, as if on “auto-pilot.”
Also, encourage them to initially keep a list of potential healthy and effective coping skills handy (on their phone, in their journal, etc.), so they can reference the list when they are having a difficult time. This practice should continue until they are very experienced in utilizing a solid set of healthy, effective coping skills. Again, remind them that when emotions are intense, it becomes significantly more difficult to think clearly and control behavioral impulses. The best approach for parents, if interested in increasing the level of healthy and effective coping, is to model daily, healthy, and effective coping.
Healthy Habits
Remind the parent group again regarding the most promising strategy at their disposal, in influencing their teen’s attitudes and behaviors, for the good, aka modeling, modeling, modeling … the attitudes and behaviors they’d like to see adopted by their youngsters. Orient the group again to the phenomenon that “Kids (teens) don’t do what we (parents) say … they do what we do!”
Facilitate a discussion around the basic elements of healthy living, cuing the group to reflect upon the roles of sufficient and regular sleep, exercise, nutrition, along with socialization with family and friends and a balance between time and energy devoted to work, school, and fun. Most teens who’ve been suffering a mood or anxiety disorder have compromised sleep and nutrition. They may have lost a balance to their lives and often have neglected their health in fundamental ways, such as failing to meet basic dietary, rest, and exercise requirements. Because families are interdigitated, interdependent systems, with each member’s habits and health affecting the health and well-being of all others, parents of youth who are struggling emotionally, nearly always report similar levels of life imbalance and compromised sleep, diet, and other basic elements of healthy living, for themselves.
Inadequate sleep severely compromises all aspects of cognition, and impedes learning and memory (Louca & Short, 2014). Inadequate nutrition can slow growth, lower energy, impair focus, and even contribute to the onset and persistence of depression and other emotional problems (Gauthier et al., 2014). Daily aerobic exercise, in moderate doses, protects against eating disorders and improves sleep, energy, concentration, and mood, while relieving stress and reducing anxiety (Rosenbaum, Tiedemann, Sherrington, Curtis, & Ward, 2014).
The point should be made that healthy living is all about balance—too much or too little sleep, calories, exercise, work, play, etc. can severely compromise overall health, potentially impairing all domains of functioning—academic, social, emotional, and physical, to name a few. Stimulate discussion with the group by cueing them to set a goal (if they haven’t already) of modifying their overall lifestyle, as a family, such that they are very deliberate in forming habits and scheduling and engaging in recurring activities that rejuvenate them physically and emotionally. Using a method of didactic discussion, with content prompts from facilitators, guide the group to recognize that to optimize health and functioning, families must commit to living a balanced life, with a sufficient degree of energizing and restorative habits, targeting both individual and relationship health, that occur no matter what. Such health-promoting activities function akin to preventative immunizations against rare but devastating diseases such as polio or rubella.
A healthy and balanced lifestyle is made, not born, and it requires continual and painstaking maintenance through conscious and willful effort. A family and each individual within a family must prioritize health promotion to the degree that those activities and habits are pursued, routinely and consistently, despite competing agendas. Sufficient time and energy must be specifically allocated in a proactive manner to promoting and preserving overall and fundamental individual and relationship well-being. In no place does the old adage, “An ounce of prevention is worth a pound of cure,” ring more true than in the field of stress management.
Conclude this section by handing out the “Healthy Habits Inventory,” and pause for a few minutes for the parents to complete this worksheet. Then pull the groups’ attention back together and invite the parents to share their findings about their lifestyle habits and overall health score. Also encourage group members to reflect up and share their plans for improving their own overall health and cue teens to offer one another feedback and support around their deficit areas and ideas for self-care.
Relaxation Training
Remind the parents that one of the most basic sets of skills offered to adolescents and adults with problems regulating their feelings, including controlling anger and anxiety, is relaxation training, which is covered in depth, in the teen workshop, as part of Module 2. Draw the anxiety versus performance curve (Diamond, Campbell, Park, Halonen, & Zoladz, 2007), as it appears below, on the board and facilitate discussion regarding the role of stress or anxiety, on functioning.
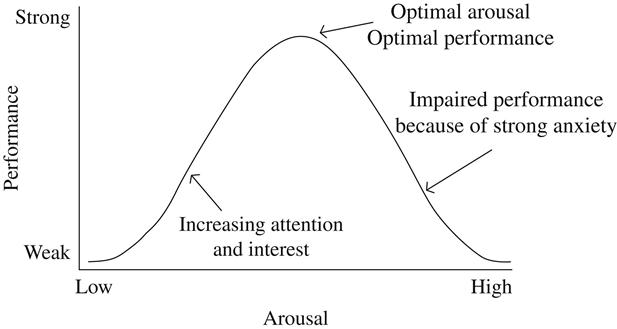
Ensure the group appreciates the “take home” point made by the curve, that is, that some anxiety is normal and healthy. Too little or too much anxiety can markedly impair performance and functioning (Diamond et al., 2007).
A variety of relaxation techniques are available, such as imagery or visualization, deep breathing exercises, progressive muscle relaxation, self-hypnosis, meditation, and yoga, samples of which were previously discussed, rehearsed, and assigned as homework. Youngsters tend to respond well to these exercises—especially imagery, deep breathing, and yoga. Numerous commercially available books, tapes, and CDs—some geared toward youth in particular—present such exercises. MaPS-Teen Module 2 provides some sample scripts for relaxation designed for teens, although they could be readily used by parents, as well.
Point out to the group that the best way to help adolescents hone their relaxation skills is to have them practice every day, building the practice into their daily routine, perhaps at bedtime each night. Practicing relaxation daily for several weeks leads to a generalization response in which a person’s baseline level of arousal is set at a lower level; thus, it takes a greater stimulus than before to cause an individual to become agitated and out of control. In addition, as adolescents master these skills, they can move more readily into a relaxed state when facing an environmental stressor. It becomes easier to calm themselves once they have escalated or, ideally, to stay calm without escalating. Without frequent and ongoing practice of relaxation or arousal-lowering techniques, once a teen begins escalating or a crisis occurs, they will not be able to make use of those tools. The exercises must be rehearsed to the point that they are “second nature” and can be done almost automatically, akin to one’s ability to tie ones shoes.
Parental Empathy Part I
Empathy Definition
The next topic considered by the group is fundamentally and monumentally important—empathy. Responding empathically is the key to “Listening So Kids Will Talk” (Faber & Mazlish, 1980). Encourage the group to generate a definition of empathy, and write their answers on a dry erase board. Most parents are able to come up with a reasonable definition of empathy. They typically seem to know what it is, at least in theory, and tend to understand it intellectually. The problem often emerges later when they are invited to role-play the expression of empathy. Following the brainstorming session, summarize the definition of empathy as follows:
Empathy is a two-step process:
Step 1: Identify what the other person is experiencing (feeling, thinking).
Step 2: Convey to that person what you believe he or she is experiencing (feeling, thinking).
Take a moment to disavow the old adage that describes empathy as “Putting yourself in someone else’s shoes,” which is actually a misnomer. Imagining YOURSELF in someone else’s shoes implies viewing a particular situation from one’s own perspective, rather than that of the other person. Empathy refers instead to the notion of “Imagining YOU ARE SOMEONE ELSE, in someone else’s shoes.” To add to the challenge inherent in empathic listening is the fact that especially in cases of parents relating to their teens, the “someone else” is someone usually very different from themselves. You can cue the group to reflect upon the types of events that might trigger intense distress in their teens, versus those that they might experience as upsetting. Usually the nature of triggers for teens is quite discrepant from those common to parents.
This concept of mentally trying to leave one’s own self behind, for the sake of entering the mind’s eye of another person, is elusive and difficult for most individuals to fully digest and grasp. What typically derails the process of achieving genuine, empathic understanding and communication, is a natural tendency for a person to project their own thoughts, feelings, temperament, etc., onto another person’s experience, which results in the first person imagining only how THEY would feel, facing that situation, rather than appreciating how the OTHER PERSON would feel, given their unique qualities, skills, and thoughts. To experience and express genuine empathy, one must develop the capacity to suspend one’s own agenda and sense of self temporarily.
Discuss with the group that the real secret to empathy lies in recognizing the fact that, because everyone has experienced the full range of human emotions at one time or another, anyone can connect with anyone else around feelings. Every human knows how it is to feel devastated, frustrated, overwhelmed, scared, rejected, or furious. This connection is what one person can offer to another person who is in distress. This is how parents can connect with their teens—by letting them know that they do, in fact, “get” what their teens are feeling. The bottom line or “take home” message for parents is that listening purely for the sake of understanding, while expressing empathy constitutes the essence of “listening in a way that others (teens) will talk.” Furthermore, teens will not be open to hearing feedback from parents, until they have felt as though they’ve been heard and validated sufficiently, that is, “They (teens) don’t care what you (parents) know, until they know that you care.”
A number of social psychology researchers have attempted to explicitly define empathy, operationalize its measurement, as well as evolve curricula for training in empathic communication techniques (Goldstein & Michaels, 1985; Gordon, 2000; Keefe, 1982; Rogers, 1957). Rogers (1957) identified empathy as a “necessary and sufficient” ingredient, in psychotherapy, a catalyst for positive changes in patients. Keefe (1982) described empathy as comprised of a series of stages, beginning with neutral observation of thoughts and feelings of another, followed by “taking in,” and mentally “holding” those constructs. However, the observer must refrain from stereotyping, judging or hypothesizing, to enable genuine empathy to transpire.
Advantages of Empathy
Empathy for Conflict Resolution
Facilitate further group discussion about empathy by fostering a dialogue regarding relationships in general. Pose the following question to the group: “What makes or breaks any relationship?” Many ideas may be suggested and discussed, but, ultimately, what determines whether any relationship will endure and remain healthy and strong is the method by which the two parties resolve conflict. To ensure that conflict is resolved in a mutually satisfactory way, each person must feel as if he or she has been heard and understood. To achieve this end, it is usually necessary for one person to temporarily suspend his or her feelings, viewpoint, and agenda for the sake of understanding the other person. In other words, one person must take the initiative in being the first to express empathy, which typically sets the stage for the other person to, in turn, listen and understand his or her partner. To suspend one’s feelings during a conflict usually requires a person to have enough trust and self-confidence, to be willing to put him- or herself into an emotionally vulnerable position.
Ask the group to reflect on the sequence of events that typically transpire when two people experience a disagreement. What is usually described is a series of efforts of increasing intensity by both individuals to push their own agenda and attempt to convince the other person that he or she is wrong. The obvious flaw with this tactic is that both parties may have markedly different and widely discrepant perspectives on the same situation. When both parties are only interested in passionately promoting their own viewpoints, a mutually satisfactory solution is untenable. Pose questions to the group that lead to recognition of the fact that feelings and perspectives cannot be judged as right or wrong. They just are.
Ask parents to think about a parent–teen relationship during which a conflict develops, then pose the following question: “Who will have the wherewithal and sophistication to initiate the exchange of empathy and taking of the other person’s perspective?” Obviously, an adolescent, especially one with a history of defiant, defensive and dysregulated behavior, is an unlikely candidate; however, parents often find, to their astonishment, that as they increasingly express empathy to their teens, the teens naturally and readily become increasingly empathic themselves, including toward their parents.
Empathy Begets Empathy
Parents often lament that their adolescents seem to lack empathy for others and refuse to take responsibility for their actions, even when their actions have hurt others. Parents typically have adopted the tact of attempting to talk their teens into having empathy and accepting accountability for their behavior, including escalating their efforts as their teen reacts with increasing defensiveness and resistance. The best chance parents have of improving the odds that their adolescents will develop empathy for others—especially others with whom they have been angry or are experiencing conflict (e.g., siblings, peers, parents)—is for parents to first give them empathy. Youth with patterns of defiant, defensive, and dysregulated behavior tend to be psychologically defensive at their baseline, exquisitely sensitive to rejection, and easily agitated. They often present as though primed for battle, awaiting the next accusation or negative consequence.
Empathy to Disarm and Lower Arousal
If the parents’ goal is to see their teen own his or her misbehavior and empathize with others, they would be better off disarming their adolescent first by empathizing with him or her. Although parents would not be advised or expected to condone, inappropriate, hurtful or unsafe behavior, nonetheless, they can at least listen to and convey a sense of understanding and validation related to the “acting out” teen’s perspective and feelings. The youngster who has egressed will no doubt, have his or her own take on the sibling conflict and usually will verbalize their sense of having been victimized or provoked. After separating the siblings, it is useful for parents to begin by appreciating each teen’s viewpoint and feelings, before reacting or attempting to facilitate problem-solving or conflict resolution. The goal is not to imply approval of inappropriate behavior; only understanding and validation of feelings and perspectives. Once the adolescent who is perceived to have acted out feels heard and validated, they usually experience an immediate, sometimes dramatic, lowering of defenses, along with a significantly increased capacity for empathy for others.
Empathy for Bolstering Self-Esteem
Educate parents that expressing empathy is a powerful verbal strategy for lowering arousal and relieving another’s distress. Empathy, inclusive of the validation of feelings and viewpoints, is also the most reliable and powerful way parents and other significant adults can bolster a child’s self-esteem. A youngster routinely getting the message “Your thoughts and feelings matter and are valid” is routinely getting the message, “You matter.” Human beings are comprised of feelings, thoughts, and behaviors; it is the feelings and thoughts that drive the behavior. It is impossible to separate thoughts, feelings, and behavior from who a person is because those elements essentially define a person.
Empathy for Relationship Building
Parental empathy is advocated by a number of authors of parenting books and developers of parenting programs including Greene (2001), Brooks and Goldstein (2001), Gordon (2000), and Faber and Mazlish (1980). It is a very effective tool to connect emotionally with and support another person, especially one who is upset. Competent therapists are experts at expressing empathy and routinely do so a great deal. Parents also may acquire expertise in this arena, and the reality is that parental empathy is infinitely more powerful in building parent–teen bonds, relieving distress, and bolstering self-esteem, than empathy delivered by a trained therapist.
Empathy to Promote Accountability
It is fairly typical for youth with histories of disrespectful behavior and impaired social relatedness to adopt a defensive posture toward others and the world. They are accustomed to being accused of wrongdoing and blamed for conflicts and negative consequences at every turn. Of course, they often do contribute to conflict and negative outcomes, but their defensive posture and tendency to be scapegoated generally leads to unwillingness and even an inability to accept responsibility for any wrongdoing on their part. In fact, one of the chief complaints among parents and teachers who interact and manage such youth is that they will not take accountability for their actions and/or show no remorse after hurting others. Adults must understand, however, that such youth cannot be convinced they are to blame for conflicts or negative outcomes when they are in a mode of defensiveness.
What works best for these youngsters is for adults to first listen to and empathize with them before trying to talk sense into them. This approach often promotes a lowering of arousal and defenses in the teen, which facilitates a broadening of his or her perspective to one inclusive of others. The teen who has behaved in a hurtful or destructive manner must first feel as though his or her feelings and viewpoint have been heard and validated before he or she is rendered capable of modifying his or her position or agenda. With a lowering of defenses, the adolescent becomes more willing and able to own his or her contribution to the conflict or negative outcome. Such a strategy often is the opposite of what adults instinctively feel inclined to do, which typically is to use coercive communication to instill a sense of blame in the teen who has acted out.
Empathy Different from Agreement
Make the point that parents should not necessarily expect to agree with their teens or to experience the same feeling in response to the same stressor. For instance, if a teen fumes “I hate my little brother, Joey!” should the parent respond, “Me too?” Of course not. When a youngster chooses a strong word, such as hate, he or she simply is trying to convey very intense feelings. The youth may have a limited feelings vocabulary and limited insight into his or her own feelings and may need the parents’ help to sort things out. What is helpful is for parents to do their best to translate their adolescent’s feelings for them—that is, to give the feelings a suitable name. What is the adolescent really saying? Usually, there is intense anger behind the word hate. Underneath the intense anger, which, again, tends to be easier and safer for teens to express than more vulnerable feelings, often lies deep hurt. Therefore, the parent might respond by saying, “It sounds like you are very angry with your brother,” or, “It sounds like Joey did something that upset you.” This type of approach stands the best chance of opening up dialogue around what really happened and what is really fueling the teen’s intense distress.
The conversation is over the minute a parent says, “How dare you say you hate Joey? He loves you. I never want to hear that kind of talk again!” The adolescent will feel ashamed and wrong and will respond by shutting down or blowing up. Instead, if parents repeatedly translate comments such as “I hate Joey” back to the teen as “you sound angry,” then eventually the adolescent will open the dialogue with “I’m so mad at Joey!” rather than “I hate…” Parents can teach their adolescents to monitor, understand, and ascribe an appropriate word to their feelings. This pattern of interacting will go a long way toward helping youngsters to identify, discuss, and deal with their feelings. In addition, this approach lowers arousal, facilitates productive dialogue, and strengthens the parent–teen bond.
Ask parents to reflect on the fact that what upsets them likely differs from what upsets their spouse and what upsets their adolescent. The specific stressor that precipitated the distress becomes almost irrelevant. The point is, in that moment, whatever the stressor, the adolescent truly is distressed. Feelings are not right or wrong. They just are. The same point can be made regarding perspectives or viewpoints. Perspectives are not right or wrong. They just are. The most powerful thing parents can do to bolster their teen’s self-esteem is to routinely validate that teen’s feelings and viewpoints. The idea is for parents to give their youngsters permission to have their own feelings and to sit with those feelings, even negative ones, as long as needed. Parents are encouraged to refrain from reacting to their adolescent’s feelings or trying to change or quash them. Youngsters have a right to hang on to their feelings. Everyone does. Suggest that parents learn to allow teens to ride out their feelings until the feelings have run their course.
Facilitate discussion with the group regarding how rare it is even for adults to express genuine empathy to one another. This probably explains, at least partially, why so many people are willing and eager to pay for prolonged, intensive psychotherapy. Their therapist’s office might be the only place where they receive consistent and genuine empathy.
Empiric Evidence Base for Empathy
If additional information is needed, to facilitate buy in from parents regarding the value of empathy training, some findings from social psychology research can be cited. This information is also cited for the sake of providing an empiric foundation and background information to the group facilitators. For instance, it has been widely shown that a number of pro-social behaviors, including cooperation, socializability, altruism, and social competence, covary with an individual’s empathic ability (Batson, Fultz, Schoenrade, 1987; Davis, 1996). In addition, it is well established that capacity for empathy is inversely related to aggressive behavior (Davis, 1996; Richardson, 1996). Finally, a vast literature has demonstrated that heightened empathic communication from therapists, teachers, and parents is positively correlated with relatively higher levels of treatment progress and academic success, along with increased cooperation and self-esteem, respectively (Goldstein & Michaels, 1985; Rogers, 1983).
Empathy Imagery Exercise
Have the parents perform the following imagery or visualization exercise, as a way of solidifying and concretizing the concept of empathy. You can read the script below aloud.
Empathy Clay Basketball Metaphor
For a moment, imagine that you have two basketballs, made of clay, stored in a refrigerator, which are therefore cold and unyielding. One of those clay basketballs represents your teen’s viewpoint and feelings about an issue or situation, and the other represents your perceptive and feelings about the same topic. Your initial challenge is to find a way to warm both basketballs of clay, while preserving their exact shape. How could you ensure both clay balls precisely maintain their original shape? (Pause for answers and discussion) The only solution, of course, is that one of the clay balls must remain “on ice,” temporarily, and remain stored in the refrigerator.
To build an alliance with your teen and enhance chances for a reasonable and cooperative response, you must start by carefully cradling their clay basketball, ever so gently, without manipulating it, using both hands. That exercise would equate to the mindset one must adopt to fully and deeply experience empathy—this process can only occur if you are simply HOLDING another’s thoughts and feelings, initially seeking only to UNDERSTAND your teen’s vantage point about a situation, without any attempt to change, influence, or insert your own agenda (as represented by the other clay basketball). In fact, if one has their own agenda in mind, or is contemplating a reaction, they are rendered incapable of listening empathically.
What happens as you carefully hold that cold, initially unyielding, clay basketball, with both hands, as a few moments pass? (Pause for an answer) Right—the clay warms and becomes malleable, as every kindergartener knows. In fact, it may spontaneously begin to change shape, simply by virtue of the warmth from your hands, without any active manipulation, as you continue to hold it carefully, for an extended period time. To have attempted to mold the clay ball before it had sufficiently warmed, while it was still cold and fixed, would have been foolish and ineffectual.
This exercise is analogous to the process of empathy—whereby, as we effectively convey to our teens that we are genuinely listening, that is, “holding,” and “getting” their viewpoints and feelings, they inevitably “soften” and often spontaneously experience a shift in their perspective (and feelings). Their feelings generally tend to fade in intensity and their take on any given situation tends to broaden in its scope, rendering them more capable of creative and collaborative problem solving, as well as more amenable to listening empathically to others. Once their clay basketball has been warmed and becomes malleable (analogous to the teen calming and becoming softer and more cognitively flexible), then you can take your clay basketball (representing your concerns) off “ice” and hand it off to your teen to hold, examine, and contemplate, in the same fashion as you just modeled. Teens tend to only be rendered capable of hearing a parent’s side of a conflict, after they have felt genuinely and sufficiently heard and validated.
Egg Catching Metaphor
Another useful metaphor that could be alternatively presented involves the classic picnic game of catching raw eggs. Ask the group whether any of them have experience with such a game? Invite them to recall their experience or imagine such a game transpiring and facilitate discussion about strategies for preserving the raw egg’s integrity. Of course, the secret to success in this game is “soft hands” and gentle catching and holding of the egg. The egg metaphor is especially salient for teens, as they tend to be quite interpersonally and rejection sensitive. They often attempt to portray a hard outer shell, especially in interactions with their parents, yet the shell is very thin and fragile, with the egg’s interior comprised of the critical substance, which is readily infiltrated and disrupted. Gently catching and holding the raw egg is analogous to experiencing and expressing empathy with a teen. One must focus on preserving the egg’s integrity, while carefully refraining from actions that could disrupt and penetrate the frail outer shell, so as to protect the precious interior substance (which of course represents the teen’s thoughts and feelings about an issue).
Temporary Tattoo Metaphor
Another metaphor that conveys the principles inherent in empathic listening is the image and steps involved to successfully apply a temporary tattoo. You could invite the group to reflect upon the steps and technique required. One must of course soften it with water and gently hold it onto an area of skin. The tattoo must be held precisely in one spot, for a sufficient period of time, for it to remain intact and adhere to skin. You can ask the group, “What happens if the tattoo is too dry?” Also, you might ask, “What if it is removed to quickly?” or “What happens if you slide the tattoo across an area of skin, during the application?” Of course this process is surprisingly delicate and requires some practice and specific technique. It is analogous to mastering the expression of empathy with teens. One must be methodical and patient, following specific steps in a particular order, with great care, softening first, holding still without movement, and then finally paving the way for an intact tattoo, or workable teen.
Parental Resistance
Many parents struggle a great deal with the suggestion that they take the time to understand and validate their adolescent’s feelings, especially in the midst of an episode of disrespectful behavior and especially if they never received empathy from their own parents. It is very common, as you offer suggestions regarding empathy and other approaches, for parents to respond, “I’ve already tried that and it didn’t work!” It is useful to recognize that some parents seem to automatically devalue and reject anything you recommend, even before you have an opportunity to outline a particular strategy fully.
Parents who have youngsters with significant emotional and behavioral problems usually have tried a myriad of approaches, often unsuccessfully. They usually are experiencing varying degrees of defeatism and demoralization, often feeling as though they are failures as parents. It is an understandable albeit frustrating pattern for parents who feel defeated to devalue therapists as part of a psychologically defensive reaction. You would do well to expect some resistance and challenge from parents and avoid falling into the trap of entering debates or becoming defensive.
What works better is for therapists simply to listen and empathize with parents about their struggles and recognize and validate their efforts and perspectives. In addition, bear in mind that although many parents are quick to react “We tried that and it didn’t work,” on closer examination it often is revealed that they haven’t tried exactly what is being recommended. In other words, “The devil is in the details.” For example, parents may have made attempts to implement behavioral contracts but used behavioral targets such as “Be good” instead of more specific goals or provided rewards that were only delivered at the end of a month instead of more regularly, both characteristics which would have doomed the contract to fail. Parents may have tried a series of approaches, but if they lacked a sophisticated understanding of the factors inducing and perpetuating their teen’s disrespectful, defensive, and dysregulated behaviors as well as the philosophy underlying effective strategies, they were unlikely to have experienced robust and consistent success.
In addition to or as an alternative to using empathy with parents who are resistant to your suggestions, you might respond to parents by gently encouraging them to consider keeping an open mind and staying tuned in. It might be helpful to acknowledge that although many of the tools discussed might already be familiar to parents, inevitably some approaches and information will be new. It is useful to acknowledge that none of the tools taught in PACK-Teen are guaranteed to work every time with every adolescent; however, traditional, authoritarian approaches to parenting that are heavy on threats and punishments are nearly always guaranteed to fail, especially when deployed with youth who are chronically disrespectful, defiant, defensive, and dysregulated.
Family Homework
Encourage families to post a comprehensive feelings’ vocabulary on their refrigerator or in another obvious, highly trafficked area. Ask that each family member identify his or her current feeling while checking-in during family meals, regarding his or her day. In addition, encourage parents and teens to reflect upon and name their emotions throughout the day, every day.
Joint Session for Module 2
As detailed earlier, in the Format and Operations section, the second session of IOP each week begins with the teens and parents initially meeting separately for the sake of “checking-in” and preparing them for the subsequent “Joint” session. The “Joint” session that coincides with Module 2 is focused on grouping teens with their own parents, for the sake of facilitating creative thinking and collaborative discussion regarding healthy, effective coping approaches for each family member. First, invite the group members to reference their “Coping Lists,” and ensure each person has a copy of the “Effective Coping Plan” worksheet. Provide extra copies of either handout if necessary.
Provide pens or pencils and have each person fill out the coping plan handout (or revise it), in reference to their own triggers, difficult feelings, and ideas of healthy and effective coping. Remind the group that when describing “triggers,” it is essential to avoid “blame, shame, put downs” and instead frame the triggers using “I statements,” or in a neutral fashion, that is devoid of judgment or derogatory language or inferences. Specific individuals should not be mentioned in the “trigger” descriptions and instead, examples of general types of situations or behaviors, can be offered, without pinpointing a particular person.
After a few minutes of individual, paper-and-pencil work, have each family join in a small circle, facing one another and take turns presenting their “Effective Coping Plan.” Encourage each person to inform their family members about their distress warning signs and the ways that they would like their family to respond and support them, when they are upset. The group facilitators can divide up and coach individual families, as indicated. After each family member has had an opportunity to present and discuss their thoughts about coping, then have the larger group come back together. Encourage the group to share their experiences with this exercise, including what they learned about themselves and other family members. Invite individuals to share specific examples of their triggers, and plans to cope in healthy and effective ways, on their own and with support and encouragement from family members.
PACK-Teen Module 2 Summary Outline
Materials Needed
Established Parent Introductions and Check-Ins
• Have the introduction and check-in format for new versus established parents written on the board.
• Go around the room and have each established parent take turns doing as follows:
• Ask each parent to identify themselves by first name.
• Ask each parent to mention their teen’s first name.
• Ask each new parent to mention one “victory” or success (required) and “challenge” (optional), from the past week, related to their teen.
• If there are new parents, invite each established parent to help in orienting the new parents to the workshop format and guidelines.
• Established parents may check-in regarding their family progress, including approaches they tried which were effective thus far.
Workshop Guidelines
• Workshop consistently starts on time and finishes on time, punctuality required, leaving early or stepping out of workshop during session, not allowed.
• Confidentiality required, “What is said in here, stays in here,” playfully termed the “Vegas Rule.”
• Refrain from developing personal relationships with other patients while in the program.
• Exceptions are safety issues (suicidality, homicidality, violence, abuse/neglect).
• All cell phones, pagers, electronics of any kind must be turned off during group.
New Parent Introductions and Check-Ins
• Have the introduction and check-in format written on the board.
• Take turns having each parent introduce themselves and check-in as follows:
• Ask each parent to identify themselves by first name.
• Ask each new parent to mention one positive feature or strength of their adolescent and mention one “challenging behavior” they’d like to focus on.
• Ask established parents to relate commonalities identified during new parent check-ins.
New Parent Orientation
Review
Effective Coping Skills
• Discuss how most people have both “healthy” and “unhealthy” mechanisms for coping.
• Ask about their responses and coping mechanisms to uncomfortable feelings and discuss if these are helpful or hurtful to themselves and others.
• Discuss and introduce “effective coping skills” to group.
• Encourage parents to develop/keep a solid set of effective copings skills handy to reference for difficult times they will experience.
Coping Skill Lists
Healthy Habits
• Encourage discussion regarding value and crucial role of healthy habits.
• Cue group to recognize need for commitment to engaging in sufficient degree of health-promoting and stress-reducing activities.
• Optimization of individual and family health requires constant attention, deliberate performance of restorative, rejuvenating individual and relationship habits.
• Provide handout titled “Healthy Habits Inventory,” have parents complete and discuss.
Discuss Relaxation Training
• Examples include deep breathing, progressive muscle relaxation, imagery, or visualization.
• Daily practice, “away from the heat of the moment” essential for mastery.
• “Generalization Response” occurs if daily practice for a few weeks.
• Practice to point of mastery, when calm or else attempting while upset is akin to trying to teach someone to tie their shoes when the building is on fire.
Discuss Parental Empathy
• Ask the group for their ideas and to provide a brief definition of empathy.
• Take a moment to disavow the old adage that describes empathy as “Putting yourself in someone else’s shoes,” which is actually a misnomer. Imagining YOURSELF in someone else’s shoes implies viewing a particular situation from one’s own perspective, rather than that of the other person.
• Empathy refers instead to the notion of “Imagining YOU ARE SOMEONE ELSE, in someone else’s shoes.”
• In the case of parent–teen communication exchanges, parents are having to imagine what it is like to be someone very different than themselves (i.e., their teen), which even further adds to the challenge of empathic listening.
• Define Empathy as a two-step process
• Step 1: Identify the teen’s experience (feelings, thoughts).
• Step 2: Communicate you understand the teen’s experience (feelings, thoughts).
• Review the Advantages of Empathy
• The key to “Listening So Kids Will Talk.”
• Fundamental for conflict resolution.
• Defuses upset so a person can become rational and able to reason again.
• Invites a discussion of the feelings and situation surrounding the upset.
• Brings the parent and teen closer because the teen feels validated and understood.
• “They (teens) don’t care what you know, until they know that you care.”
• Teaches the teen how to identify and express feelings in an appropriate, more mature way (also helps if parents consistently model appropriate expression of anger and other emotions).
• Builds healthy self-esteem (i.e., “My feelings matter so I matter!”) and strengthens identity.
• Empathy does not equal agreement.
• Conduct Empathy Imagery Exercise as Follows:
• Empathy Clay Basketball Metaphor:
For a moment, imagine that you have two basketballs, made of clay, stored in a refrigerator, which are therefore cold and unyielding. One of those clay basketballs represents your teen’s viewpoint and feelings about an issue or situation, and the other represents your perceptive and feelings about the same topic. Your initial challenge is to find a way to warm both basketballs of clay, while preserving their exact shape. How could you ensure both clay balls precisely maintain their original shape? (Pause for answers and discussion) The only solution, of course, is that one of the clay balls must remain “on ice,” temporarily, and remain stored in the refrigerator.
To build an alliance with your teen and enhance chances for a reasonable and cooperative response, you must start by carefully cradling their clay basketball, ever so gently, without manipulating it, using both hands. That exercise would equate to the mindset one must adopt to fully and deeply experience empathy—this process can only occur if you are simply HOLDING another’s thoughts and feelings, initially seeking only to UNDERSTAND your teen’s vantage point about a situation, without any attempt to change, influence, or insert your own agenda (as represented by the other clay basketball). In fact, if one has their own agenda in mind, or is contemplating a reaction, they are rendered incapable of listening empathically.
What happens as you carefully hold that cold, initially unyielding, clay basketball, with both hands, as a few moments pass? (Pause for an answer). Right—the clay warms and becomes malleable, as every kindergartener knows. In fact, it may spontaneously begin to change shape, simply by virtue of the warmth from your hands, without any active manipulation as you continue to hold it carefully, for an extended period of time. To have attempted to mold the clay ball before it had warmed sufficiently, while it was still cold and fixed, would have been foolish and ineffectual.
This exercise is analogous to the process of empathy—whereby, as we effectively convey to our teens that we are genuinely listening, that is, “holding,” and “getting” their viewpoints and feelings, they inevitably “soften” and often spontaneously experience a shift in their perspective (and feelings). Their feelings generally tend to fade in intensity and their take on any given situation tends to broaden in its scope, rendering them more capable of creative and collaborative problem solving, as well as being more amenable to listening empathically to others. Once their clay basketball has been warmed and becomes malleable (analogous to the teen calming and becoming softer and more cognitively flexible), then you can take your clay basketball (representing your concerns) off “ice” and hand it off to your teen to hold, examine, and contemplate, in the same fashion as you just modeled. Teens tend to only be rendered capable of hearing a parent’s side of a conflict, after they have felt genuinely and sufficiently heard and validated.
• Egg Catching Game Metaphor (Another Option for Conveying Essence of Empathy)
• Temporary Tattoo Metaphor (Additional Option for Explaining Empathy)
• Review the PACK-Teen Mantras
• “If you accept children as they are … then they will change!”
• “Model the behavior you want to see.”
• Review, Answer Questions, and Wrap Up
• Encourage families to post a comprehensive vocabulary of feeling words (provide handouts from book’s companion website on their refrigerator or in another obvious, highly trafficked area). Ask each family member to identify his or her current feeling while checking-in during family meals regarding their day. In addition, encourage parents and teens to reflect upon and name their emotions throughout the day every day.
• The parents are encouraged to schedule family meals, at least weekly, where all members gather at a table and each person takes a turn, sharing the best and worst parts of their day, to model and facilitate practice of conversation and listening skills.
• Recommend that each family continue discussions and rehearse skills for healthy and effective coping, including using some of the ideas they generated during the joint session for Module 2.
• Pair teens with their own parents and provide each person with a list of coping ideas (available in book’s companion website).
• Provide each group member with an “Effective Coping Plan” hand-out and pen or pencil. Have them fill out (or update) the hand-out for a few minutes.
• Have teens work with their own parents, taking turns presenting their triggers, difficult feelings, and ideas for healthy and effective coping (including plans for self-care along with preferences for responses from family when distressed).
• Invite teens and parents to report to larger group, regarding their experiences, ideas, and plans.
Handouts/Business Cards
Module 2-PACK-Teen Calming Steps Summary Cards Therapist Tool #2
Module 2-PACK-Teen Coping Skills List Parent Handout #7
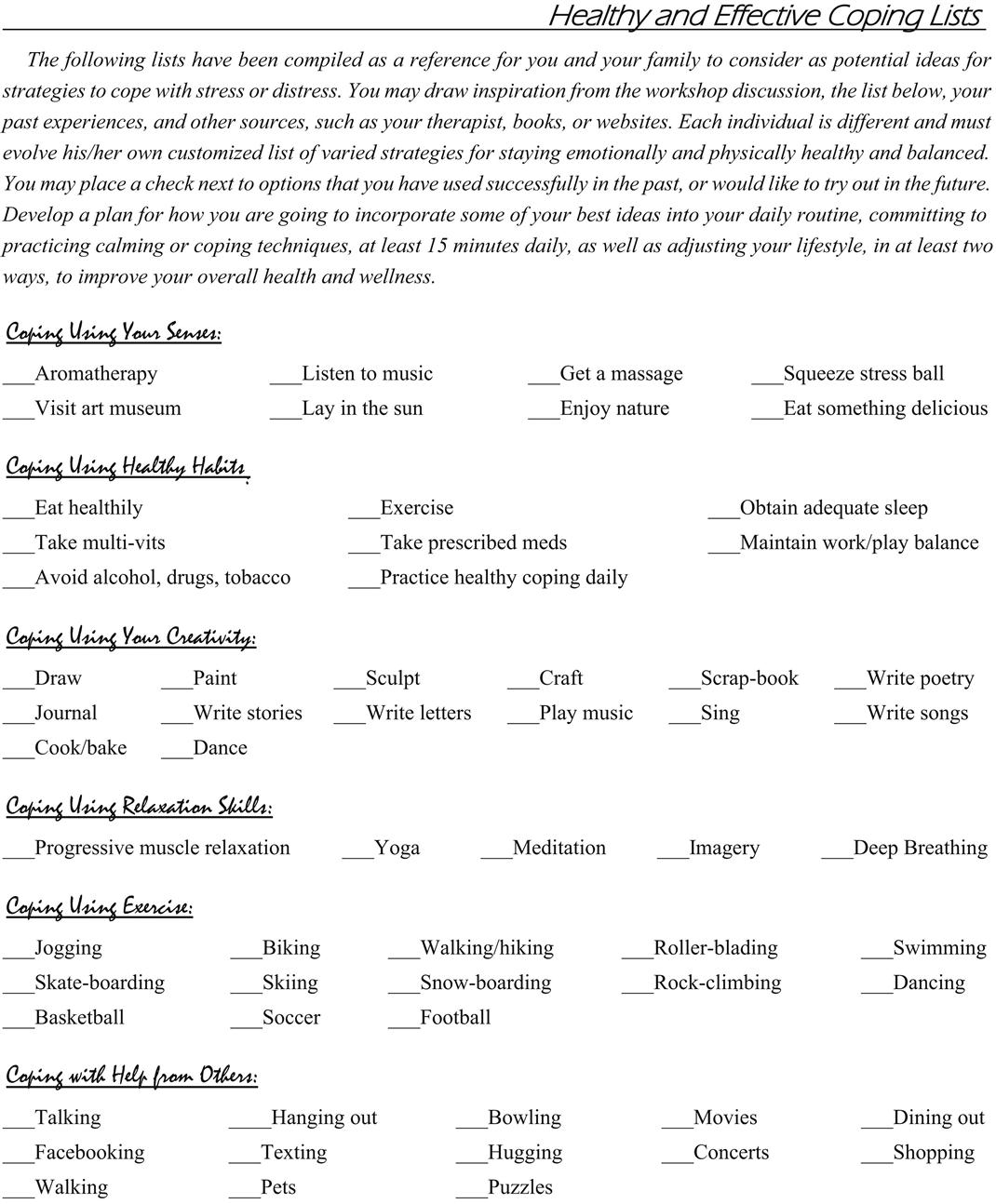
Module 2-PACK-Teen Healthy Habits Inventory Parent Handout #8
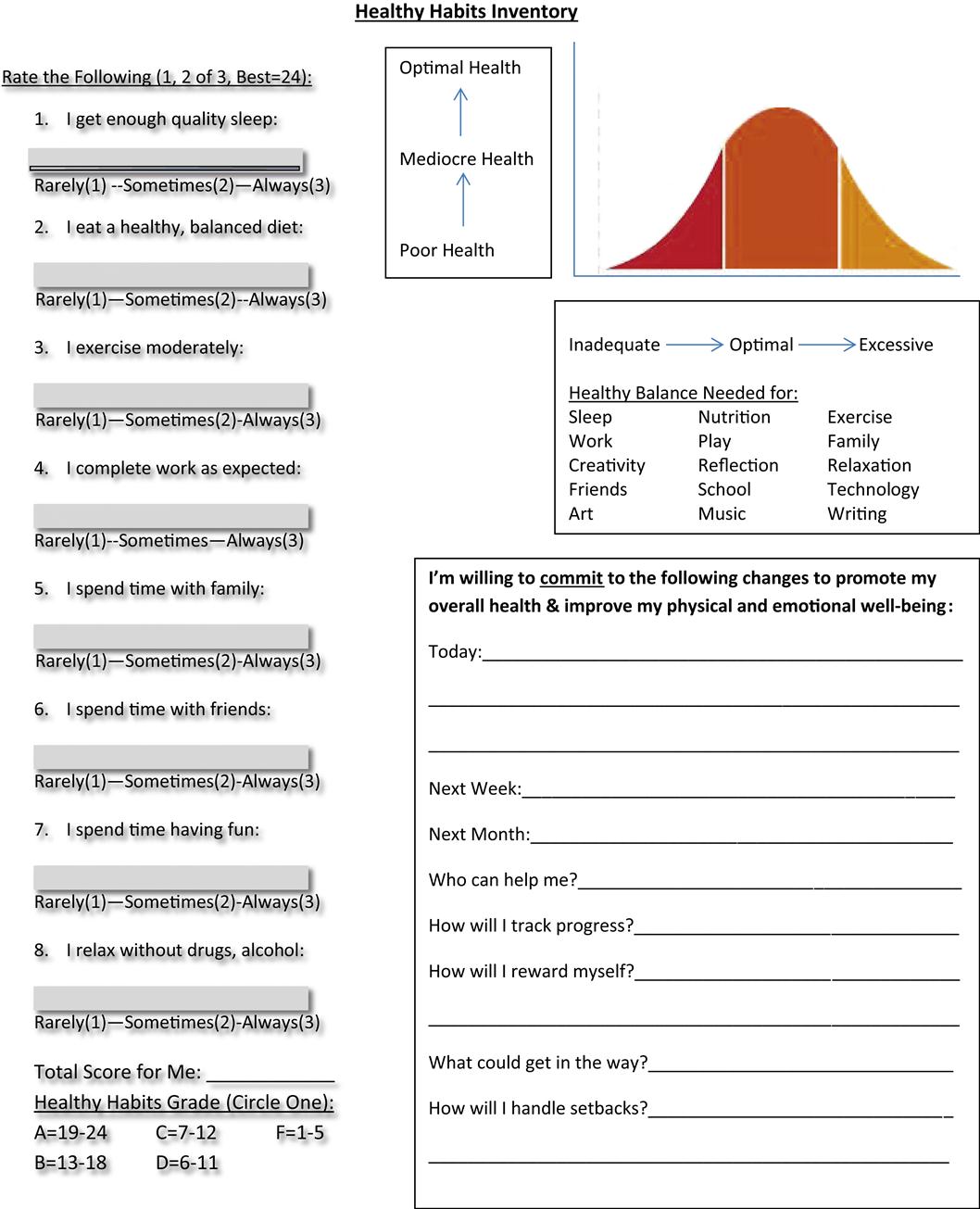
Module 2-PACK-Teen Effective Coping Plan Parent Handout #9
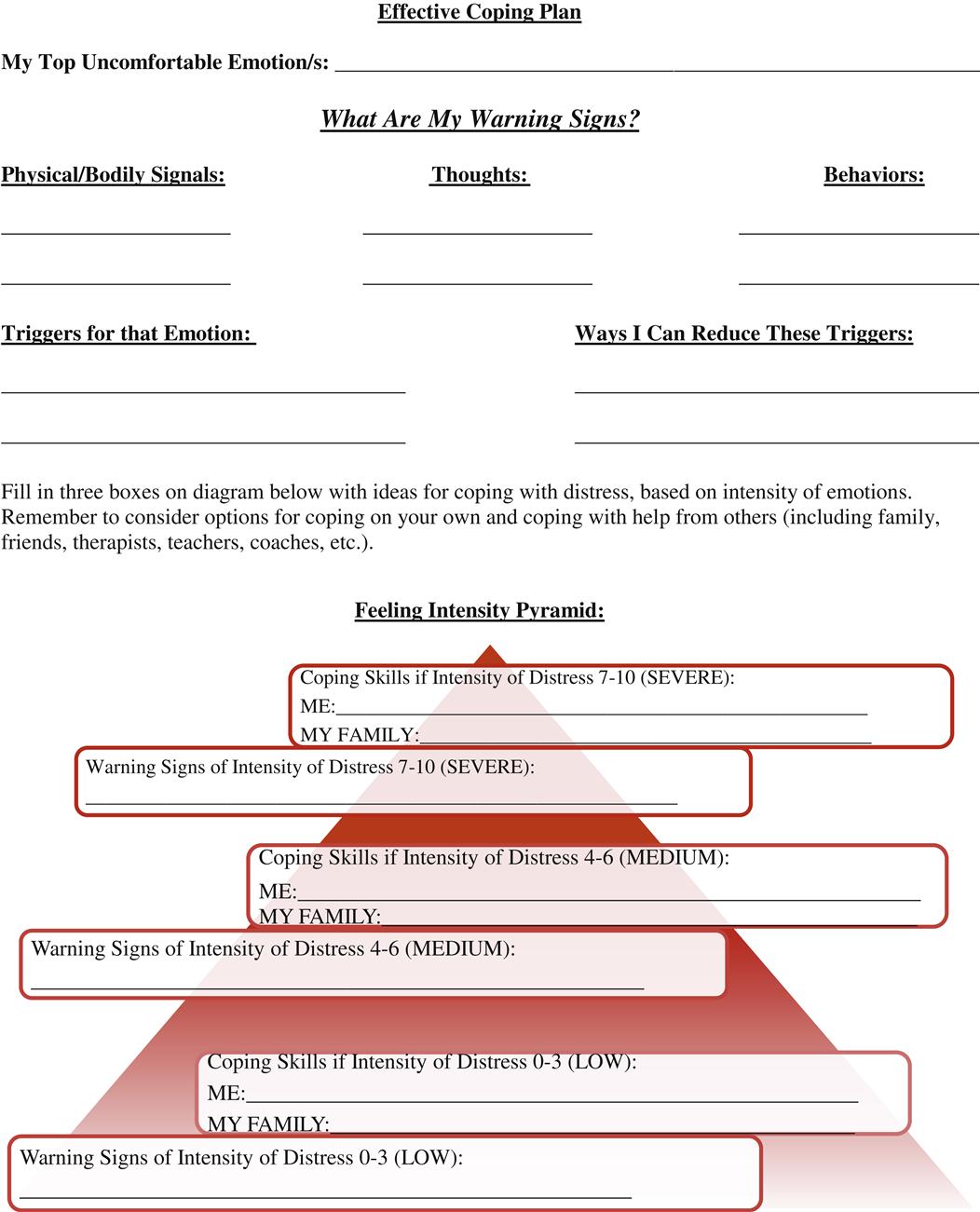
PACK-Teen Module 3
Introductions, Check-Ins, Guidelines, and New Parent Orientation
Module 3 begins with introductions, and a review of group guidelines, as detailed above. Returning parents are invited to relate a “victory” (required) and “challenge” (optional) regarding an experience connected to their recent attempts with practicing skills covered in group. Parents are asked, on their first day, to share one strength and one challenge, related to their adolescent, rather than specific instances of experiences. Parents may receive a workbook, containing a complete set of parent worksheets and informational handouts, except for those related to homework between sessions, unless the facilitators have elected to handout worksheets individually, by module. Parents are provided a brief overview and orientation to the program, on their first day to include a discussion of the modular format, along with a brief overview of the syllabus. The schedule and topics for the day should be written on the dry erase board and a brief review of the latest topic is conducted, before new material is introduced.
Empathy Test
Before embarking on additional training and practice of the expression of parental empathy, administer the Multiple Choice Test on Parental Empathy that appears at the end of the bulleted outline section of this module as well as on the book’s companion website as PACK-Teen, Module 3, Handout #10. Instruct parents to answer the questions as they typically would respond to their adolescents. Mention that parents will correct their own tests and that no one will be graded or criticized for getting the “wrong” answers. The test is simply an exercise to get parents thinking (as well as to get them interested in the psycho-education that follows). The test will be discussed at a later point. Once parents have completed their empathy tests, have them turn them over and set them aside for later review and discussion.
Empathy Bustersb
In this module, a menu of response types called empathy busters is introduced. These are common, if not typical, responses that most people frequently heard from their own presumably well-intentioned parents while growing up. Parents often find themselves employing these same types of responses fairly automatically in response to common scenarios they face with their own children every day.
Write a list of these response types on the dry erase board, and then generate a series of randomly ordered examples, inviting the group to guess which type of response is being illustrated with each new example. At the end of this exercise, encourage parents to come up with their own examples or experiences that might further illustrate the concepts. The typical list of busters follows; they can be remembered using the acronym S.S.S.S.S.L.U.R.P.P.E.D.D.
Solving the problem: “I’ll get you a new one.” “I’ll call her mother right now.” “I’ll fix it.” “I’ll call your principal.”
Sympathy: “You poor thing.” “How horrible that is.” “My poor baby.”
Sarcasm: “I’ll give you something to cry about.” “Oh, it’s just the end of the world.” “Boo hoo, whah, whah, what a crying shame.”
Shame, blame, and put downs: “Sounds like you deserved it.” “You should have known better.” “Why did you provoke him?” “You are so selfish.”
Scolding: “You should have known better.” “You should have studied harder.” “You should have practiced more.” “How dare you say that?”
Lecturing: “You really need to work harder. If you don’t get your act together, you’re going to fail, and if you fail now, then you’ll grow up a failure. You should really take things more seriously.”
Unsolicited advice: “Well if I were you….” “I think you should….” “Why don’t you just…?”
Reassurance: “Your hair will grow back.” “There are other fish in the sea.” “Nobody will notice.” “There will be other games (or tests, friends, dances, and so forth).”
Philosophy lesson: “Life is like that.” “Everything happens for a reason.” “This setback will make you stronger.” “It was God’s will.” “Big boys don’t cry.”
Psychoanalysis: “Did it ever occur to you that the real reason…?” “You’re only saying that because….” “You’re just upset because….”
Enemy (Defending the…): “What did you do to invite that?” “The teacher was just trying to….” “No wonder Johnny did that.” “You probably asked for it.” “I’m sure she didn’t mean it.”
Dismissing feelings: “It’s not that big a deal.” “You shouldn’t feel that way.” “I’ll give you something to cry about.” “Get over it.”
Detective: “So what happened?” “Why are you so mad (upset, sad, frustrated)?” “So what are you going to do?” “Why didn’t you study harder?”
Parents usually will acknowledge that the empathy busters outlined above are actually common responses that they routinely employ with their teens and others. Some of these types of busters actually sound reasonable and even supportive at first blush. For example, parents typically will ask, “What’s wrong with giving advice, solving the problem, offering reassurance, or asking questions? What’s so wrong with offering your teen a little advice or offering to solve their problem?”
Invite parents to think of and share with the group their own experiences of being in distress and having a spouse or friend respond in one of these traditional ways. For example, you might ask, “If your spouse were ill or dying, would it comfort you or relieve your distress if someone said ‘It’s God’s will?’ What if you were sobbing inconsolably and your spouse asked, ‘Why are you so upset? What’s the big deal?’ Or, if you really felt like a failure and genuinely had performed poorly, would it help if your friend said, ‘You did great! Better than I would have.’”
Discuss with the group the fact that everyone, including youngsters, can detect false praise or false reassurance a mile away. In general, people know when they have done well and are usually well acquainted with their own strengths. Likewise, most people know when they have done poorly and know their own weaknesses. Thus, for a teen who is lamenting about his failure or poor performance, reassurance and empty praise usually will feel patronizing and even demeaning. What feels better to most everyone, especially teens, is allowing them to vent their feelings while showing them empathy. It is helpful for parents to respond in such a way that they leave their adolescents feeling understood and heard.
Facilitate discussion regarding the fact that the basic problem with the empathy busters is that they leave a teen who is distressed feeling as though his or her feelings are wrong. The implication is that the teen also is somehow wrong for having the feeling. Youngsters, confronted with some of the empathy busters, often will work harder and harder to convince parents that they do, in fact, have a valid reason for feeling whatever it is they are feeling. Questions often make teens feel defensive, as though they have to defend themselves and their feelings. Lectures feel denigrating and shaming at a time when adolescents already are feeling hurt and vulnerable. Teens usually react to parental dismissal of their feelings by becoming increasingly upset and agitated. In addition, teens are made to feel defensive and once defensive, their primitive threat response is activated, which results in them experiencing anything subsequently said as static or the garble that represented the teacher or parent’s voice from Charlie Brown’s cartoon series.
If adolescents’ feelings are dismissed and negated repeatedly, the result will be low self-esteem and an inability to trust or openly express their feelings. Repeated dismissal or invalidation of feelings may interfere with the development of assertiveness. Plus, this pattern of interaction creates and perpetuates a chasm between parent and teen. The teen will bemoan, “My parents never understand me” or “My parents never listen.” In addition, ask parents, “What is implied to a youngster if when he or she presents a problem we respond by giving advice or solving the problem for him or her?” The downside to the two empathy busters of solving the problem and unsolicited advice is that the adolescent likely will become more distressed at feeling as though their feelings are not being validated; in addition, use of these two empathy busters robs teens of the opportunity to practice solving their own problems, including gaining a sense of mastery and accomplishment that comes with successful, independent problem solving. The parental role, therefore, is not to tackle a specific problem presented by a teen but instead to help him or her label, discuss, and process his or her feelings, thus paving the way for a calm discussion related to creatively solving the problem at hand. This paradigm shift is a major struggle for most parents, who feel compelled to fix things and give advice rather than facilitate the identification and processing of upset feelings.
Generate discussion regarding the fact that it is useful for parents to resist their natural urge to rush to their adolescent’s rescue and try to “make it all better.” Ironically, riding out the distress ultimately is what relieves it. What goes up must come down. Parents rushing in to quash feelings or rescue their children from upset tend to fan instead of extinguish the fire. This notion, though counterintuitive, is a reality. This phenomenon resonates with another that often is seen with parents who are dealing with adolescents: The harder parents hold on, the more their teens push them away. Parental utilization of empathy busters is likely to activate defensiveness, increase defiance, and heighten arousal.
“Business cards” on which are printed the list of empathy busters above are available in the PACK-Teen Module 3 Therapist’s Toolbox on the book’s companion website. These cards can be cut apart and distributed to parents to use during the session and at home.
Review of Multiple Choice Test on Empathy
Once the group has finished their discussion of empathy busters, have them turn back their completed “empathy tests.” Go around the circle, having them take turns reading the statements and possible answers, while identifying which responses sound like empathy and which do not. Ask the parents to identify which empathy buster is being illustrated in the responses they recognize as not being empathic.
Identifying Feelings in Others
Invite the group to brainstorm ideas or clues, starting with nonverbal ones, for determining what someone else is feeling. Write the responses on the dry erase board. Encourage parents to reflect upon all the senses to which they should attend, as they attempt to understand the perspective and emotional experiences of another person. Help them appreciate that to increase their odds of accurate interpretation of signals, they should deploy their eyes, ears, brains, hearts, and intuition. The following four “Feeling Clues” should be included in the final list:
Feelings Vocabulary
Note to the group that many youngsters who act out feelings have an impoverished or even nonexistent feelings vocabulary. These youth often have alexithymia—an inability to express their feelings in words. Suggest that parents begin to role model habitually expressing their own feelings in words. This process starts with self-monitoring, whereby parents check in with themselves and identify what it is that they are feeling at any given moment. By putting words to their own feelings, parents show their teens that it is possible to express strong feelings (e.g., anger, despair) in a safe manner while maintaining control over one’s behavior. Parents also demonstrate that it is possible to use talking as a way of relieving distress and uncomfortable feelings.
Invite parents to brainstorm a list of feeling words, which may also be jotted on the dry erase board. First cue them to shout out examples of positive, pleasant feelings and then invite them to focus on generating a list of unpleasant or negative ones. Write this list on a dry erase board. A comprehensive list of feelings words is available on the book’s companion website as PACK-Teen Module 2, Handout #3. This list also is included for your reference following the bulleted outline at the end of this module.
Encourage parents to post a list of feelings words in an obvious place, such as on the refrigerator, and to model identifying and stating their own feelings aloud as often as possible. Parents can encourage all family members to do likewise. Many of the feelings words that appear on the list are sophisticated words, which parents might need to define or explain. The broader and more sophisticated teen’s feelings vocabularies become, however, the less likely they will resort to acting out feelings in a destructive manner.
Mirroring
Before performing some empathy role-plays introduce and discuss the skill of mirroring, which has also been termed “active” or “reflective” listening. Typically, at least some of the parents are acquainted with this type of response. Mirroring refers to the idea of simply paraphrasing or repeating back parts of what another has said. This style of response demonstrates that the listener is interested in the other person and is tracking what he or she says. This technique is useful for maintaining conversations, processing upset feelings, and building relationships with others. Use didactic discussion to teach the parents how to perform mirroring—that is, repeating back portions of or paraphrasing what the other person has said.
A subtle but important point to impart is that mirroring is experienced as most genuine, when the listener paraphrases what is being said, using completely or at least primarily new verbiage, different than what was stated by the speaker. In other words, when the mirroring is comprised of primarily repeating, verbatim, like a parrot, exactly what was said or portions thereof, the speaker may be put off and reject the listener’s attempts to express empathy, which may have been experienced as awkward and ingenuine by the speaker. However, another important but subtle point, that must be understood, is that the listener must refrain from introducing new ideas or pushing their own agenda, during this exercise. As the listener focuses on restating, using fresh language, a point made by the speaker, he or she should strive to capture the essence of the speaker’s point, as accurately as possible, using original words, but at the same time, resist introducing novel ideas that were not contained in the speaker’s statements.
Much rehearsal of this sophisticated and challenging skill is required, before a listener can be adept at empathizing and mirroring, especially if processing an area of disagreement or conflict, with the speaker. The following “mirroring stems” are suggested to the group, as a way of guiding the listener to reflect and validate the speaker and may be written on the dry erase board:
“So it sounds like you feel as though … (paraphrase speaker’s message)”
“So what I’m hearing is that … (paraphrase speaker’s message).” “So what you’re saying is that … (paraphrase speaker’s message).”
These phrases should be written on the dry erase board and handed out to parents by way of the empathy “business cards” found in the PACK-Teen Therapist’s Toolbox, Module 3 on the book’s companion website. Mirroring reassures the speaker that he or she has been understood and heard by the listener and allows the listener to demonstrate a willingness to track and understand what is being said without critiquing or offering unsolicited feedback. While expressing empathy and mirroring, the listener should not be entertaining or projecting any other agenda or goal other than to understand the experience of the person who is distressed and relaying his or her story.
Another potential advantage of the mirroring process is that it can lead the adolescent to essentially hear him- or herself through the parents’ reflections. This can be a powerful tool and help the teen gain insight and come to appreciate some of the distortions in his or her thinking or the exaggerated nature of his or her emotional response to a relatively minor stressor. For instance, an adolescent might accuse his or her parent of “never helping me, ever!” If the parent echoes back “So you feel as though I’ve never, ever helped you,” then the teen might begin to recognize that his or her position is unreasonable.
Encourage parents to reflect on the fact that during a typical conversation, most people are preoccupied with contemplating their next response and not completing attending to what the other person is saying. The process of mirroring demands that a person pay careful attention to the speaker and shifts the focus on them, over the listener. It is an effective tool when one person, such as a parent, is trying to support, understand, and be truly present with another person, such as a youngster. Reiterate the notion that empathic listening is about understanding, not responding or reacting. In fact if the listener is experiencing their own reaction (feelings, thoughts) or mentally contemplating a response, they are incapable of fully hearing and understanding the message being shared by the speaker. Sometimes with youth, especially adolescents, it helps for parents to just stay quiet and perhaps nod occasionally. Simply saying “Oh,” “Hmmm…,” “I hear ya’” or “Tell me more” often works well.
As parents “dial in” and contemplate the overt messages being transmitted by their teens, both verbally and nonverbally, they might also come to recognize and appreciate the “metamessages” inherent within their youngsters’ communication. Consider the following examples:
14-year-old Joey complains, “I hate my stupid teacher … she yelled at me in front of the whole class!” The metamessage might be comprised of a concern about feeling humiliated in front of peers and a girl on whom Joey had a crush.
16-year-old Stacey laments, “You always take Megan’s side!” The metamessage might be comprised of concerns about favoritism of a younger sibling or even a sense of being less loved.
17-year-old Doug decries, “You don’t care if I never come home!” The metamessage is that he is very concerned that perhaps parents would prefer life after he’s gone and won’t miss him.
As an alternative to mirroring, using the “mirroring stems,” a statement made by one person can be repeated by the other person in the form of a question. For example, if Susie says “I want to switch schools,” then the parent could respond, “You want to go to a new school?” It also helps to demonstrate good listening if the listener responds relevantly to the speaking individual or expands on what has just been said. The listener, if they feel confident to do so, can make an inference, about a deeper message, underlying the speaker’s concern, or convey a stronger sentiment that is sensed. For example, if Susie says “I can’t stand Joey (little brother) and feel like punching him!” then the parent could say “So Joey’s been driving you nuts, and you just can’t stand him anymore.” However, this approach is more risky than simple empathy and mirroring, as the listener could miss the mark and inadvertently convey misunderstanding or a sense of presumptiveness.
Overcoming Barriers to Empathy
Review the following list of the “Top 10” Parent–Teen Empathy Barriers and using a method of Socratic discussion, spur the group to generate ideas of strategies for averting and overcoming these barriers. As the discussion of the common barriers and potential means for overcoming them comes to a close, you may refer parents to the corresponding hand-out on this topic in their workbooks or alternatively hand out copies, if no preassembled workbooks are available. The list is comprised of the following:
#1-Parental Hidden Agenda
It is instinctual for parents to concurrently contemplate their own agendas while listening to their teens, such as a desire to change, correct, teach, advise, problem-solve, or contract with their teen.
Solution: Parents must learn to temporarily, but genuinely and wholly, suspend their concerns and agendas, while listening empathically.
#2-Parental Blame/Judgment
When teens present their version of a situation, especially one in which they experienced negative consequences, it is natural for parents to look for and comment upon sources of error or flawed thinking or behavior in teens.
Solution: Parents must learn to suspend formulating judgments, identifying short-comings or assigning blame, while listening empathically.
#3-Parental Distress
When teens present their version of a situation, especially one that involved conflict with another family member, including a parent or sibling, parents naturally begin having their own emotional reaction and may inherently experience increasing levels of defensiveness and distress.
Solution: Parents must learn to refrain from interpreting teen reports personally and avoid “taking the bait” that teens may confer in the form of provocative or “snarky” remarks.
#4-Parental Insincerity
Teens often exhaust and overwhelm their parents. As teens relay their sense of injustice, entitlement or seemingly distorted perspective, it is often difficult for parents to listen openly and remain focused solely on genuine understanding and acceptance.
Solution: Parents should only engage in empathic listening when they feel physically and emotionally refreshed and capable of genuine understanding and acceptance. The genuineness of the parent’s intent is the most pivotal ingredient to the teen’s receptivity.
#5-Insufficient Time
Families are busy, with most days packed with “to dos” and rare “down time” for simply relating and sharing, especially feelings.
Solution: Parents should request a scheduled, at least weekly, appointment with their teen, on a recurring basis, as well as whenever needed, during which parent and teen agree to give one another their undivided attention.
#6-Insufficient Energy
Families are busy and often energy-depleted.
Solution: Parents should attempt to approach their teens and communicate with them around difficult topics, when and only when all parties are rested, fed, and receptive.
#7-Teen Escalation
Particularly with chronically contentious topics, teens may become rapidly and intensely agitated, when the subject is broached by parents, even in an ideal manner.
Solution: Despite doing everything possible to set the stage optimally and use ideal approaches, teens might become too reactive to have productive exchanges. When parents sense teens are ramping up, approaching the “point of no return,” they should abort their intervention and look for a more workable moment in the future.
#8-Teen Resistance
Particularly with chronically contentious topics, teens may refuse to engage with parents, and either remain mute or walk away.
Solution: Despite doing everything possible to set the stage optimally and use ideal approaches, teens might refuse to engage in productive exchanges. When parents sense teens digging in their heels or when they withdraw or walk away, parents should avoid the urge to continue a pursuit. Instead, parents should abort their intervention and look for a more workable moment in the future.
#9-Distractions
Siblings, pets, electronics, phone calls, and friends can disrupt and derail empathic conversations and productive conflict resolution efforts.
Solution: Parents should attempt to meet with their teen “one on one,” ideally away from the house. There should be an agreement that all electronics are turned off and neither parent nor teen is permitted to answer emails, calls, or texts, during empathic communications.
#10-Parental Projection
It is instinctual for parents to project their own inferences or biases onto their teen. So, too, parents are prone to make assumptions about their teen, based on past experiences.
Solution: Parents must train themselves to refrain from making inferences or interpreting their teen’s motives, while listening empathically. They must actively will themselves to avoid making assumptions or “reading into” their teen’s report of an experience, but instead just understand and accept it, “as is.”
The “3-Minute Rule”
As a useful guideline, suggest that parents should spend at least 3 minutes empathizing and listening to their teen before they react or even begin to communicate their own feelings, and viewpoint. During this 3-minute process, parents should refrain from adding any new or original ideas or feedback of their own to the discussion with their teen. Advise them simply to listen with undivided attention or use only empathy statements or mirroring techniques. Their only mission is to focus completely on developing a deeper understanding of their teen’s feelings and perspective regarding the situation at hand. Many parents struggle and feel befuddled while practicing empathy and mirroring and report, “I just can’t think of what to say!” If this is their complaint, then it is likely they are not listening carefully to their teen and “aren’t doing it right.” If their teen is talking and they are truly listening, the parents will always have something to say; they can use the empathy formulas or paraphrase or summarize what they think they have heard and gleaned from the adolescent’s dialogue.
This exercise is next to impossible for some parents, especially fathers, in our experience, because of several factors. First, many parents become anxious at this suggestion and worry that suspending their agenda temporarily might jeopardize their agenda ever being met at all. Through hands-on practice of these techniques, parents increasingly are reassured that suspending their agendas temporarily for the sake of first aligning with their teen actually increases their teen’s capacity to consider and even cooperate with the parent’s agenda. Second, many parents cannot resist the urge to analyze what their adolescent is saying and tend to react, formulate ideas, or jump to conclusions before the teen has even said his or her piece. To overcome these patterns, it is helpful to have parents repeatedly role-play empathy and mirroring exercises until a degree of mastery has been attained.
What tends to trip up most individuals, when they first attempt to listen empathically, is a powerful instinct to mentally analyze the information being shared and engage in formulating a response. That typical and instinctual mental activity consumes the focus of the listener and therefore precludes them from wholly listening and understanding the speaker. Here is a sample dialogue that you can invite two parents to read and act out aloud for the group:
Scenario: You have recently informed your 15-year-old daughter of the need to move out of state.
Parent A (15-year-old girl): “I just can’t leave my friends. I’m never moving. You’ll have to go on without me.”
Parent B (mother): “You sound really upset.”
Parent A: “Yeah I’m upset. Wouldn’t you be? I’m so mad. You and Dad are ruining my life.”
Parent B: “Your friends mean the world to you, and you can’t bear to leave them.”
Parent A: “That’s right. My friends are the most important thing—more important than my family.”
Parent B: “No one can take the place of your friends.”
Parent A: “Especially Jean. She’s been my best friend since kindergarten. I could never find another friend like her. I’ll be lost without her.”
Parent B: “Jean is a really special friend—the kind that only comes along once in a lifetime.”
Parent A: “I can’t leave her. I won’t have anyone to talk to or hang out with.”
Parent B: “Not seeing Jean every day is going to be hard on you. I wonder if there’s anything you could do to make it easier on both of you?”
Parent A: “Nothing will help. Not moving is the only thing.”
Parent B: “You seem heartbroken. Maybe you and Jean can put your heads together and figure out a way to make this move a little less hard on both of you.”
Parent A: “Can I come back and stay with her all summer?”
Parent B: “Visiting each other may be an option.”
Parent A: “I’m going to call her right now. Maybe we could make scrapbooks for each other.”
Parent B: “Or get cell phones with unlimited long distance.”
Parent A: “Really? That would help … a little.”
The point that the sample role-play attempts to illustrate is that reassurance will not work in situations such as this. It only will exacerbate the 15-year-old daughter’s distress and solidify her perception that the parent is a dope who understands nothing. It is better for parents just to focus on understanding their teen’s perception and feelings and follow her lead. It is therapeutic and alliance-building for parents to allow their youngster to say strong things, even outrageous and provocative things. This is not to say that parents should not set limits and prohibit the use of foul language, insults, or threats; these things should not be tolerated. Outrageous and provocative remarks, however, often are intended by youth as bait to agitate their parents and invite an altercation. These comments also are used by youth to convey strong feelings. Teens are eager to be heard, validated, and impress upon their parents just how strongly they feel.
Reassure parents that, usually, it is not truly the case that the teen in the example is entertaining the idea of staying behind while the family moves. She simply is experiencing intense despair and feels overwhelmed by her painful feelings. She uses strong language and says extreme things because she’s bent on making the parent aware of just how powerful her feelings are. Encourage parents to validate her feelings and reflect back what they heard. Parents do not need to say, “Okay, you can stay here while the rest of the family moves.” That kind of unreasonable response will not help and will feel sarcastic and dismissive to her. They can, however, give her what she wants in fantasy—“I wish you and Jean could stay neighbors”—or simply identify her wish: “You wish you could stay here forever.”
Note that in the sample scenario, the girl made many provocative remarks (e.g., “I’m not moving,” “My friends are more important than my family”). It would be easy and natural for parents to become agitated and launch into a lecture at such points (e.g., “Don’t be ridiculous; of course you’re moving”). This kind of comment likely would shut the daughter down and exacerbate her distress.
Trivializing feelings and offering reassurance are two examples of other natural and common parental reactions. Parents often are tempted to say things such as, “Don’t worry, you’ll make new friends” or “It’s not the end of the world!” Remind parents that during empathic dialogues, their job is to avoid trying to convince their child of anything. The parent should have no other agenda than to listen, understand, and validate the child’s feelings and perspective.
As parents practice and increasingly master putting themselves wholly in their teen’s shoes, that is, envisioning the teen’s feelings and perceptions, they will increasingly hone natural instincts in knowing just what to say to defuse the teen’s upset. However, to truly be empathic with their adolescents, parents must learn to clear their minds and suspend their own feelings and agendas, at least temporarily. To deeply and completely understand the experience of another person, one must learn to refrain from reacting, and temporarily suspend their sense of self. Parents must practice presenting as open and neutral, devoid of judgment or response, to truly and fully appreciate their teen’s perspective.
Caution parents that they must be in a good emotional space to have this type of empathic dialogue in which they allow their child to take the lead and ventilate. This kind of discourse can be intense, and parents might not always have the emotional reserve and degree of psychological centeredness, that is required to make it work. Parents need to know themselves well and recognize whether they are truly up for an empathic conversation, especially in delving into a highly contentious or emotionally charged topic. In the past, if emotional reactivity and an aggressive style commonly characterized parent–teen dialog, both parent and teen will likely have become “sensitized” to one another’s verbal and nonverbal cues, hence apt to experience a “hair-pin” trigger and speedy escalation of arousal and hostility.
Remind parents of the “Taming Bambi” metaphor. Invite them to recall the steps necessary to gradually build trust with Bambi (or their teen), such that, slowly but surely, they demonstrate a level of acceptance and understanding that is deep and genuine. Remind them also, that they may be attempting to build a connection, from a point of a relationship deficit. It will likely take a great deal of persistence and patience, for parents to be accepted by their teens as trustworthy and safe, nonjudgmental confidantes. The teens are prone to doubt and test parents’ sincerity as they initially endeavor to transform the nature of parent–teen communication. The connection will not come quickly or readily and must be built slowly but surely, with steadfast effort and tenacious optimism, harbored by parents.
Once parents begin practicing empathy and Problem Solving Together (PST; covered in Module 4) with their youngsters, they often are amazed by the degree of cooperation and goodwill achieved; these strategies become inherently reinforcing. Encourage the group to recall being 15 years old, when friends and romantic interests were of utmost importance. At age 15, one often feels as though the world would end if anything compromised one’s relationships with peers. The parents’ goal is to help teens in distress feel as though their thoughts and feelings are respected, understood, and validated by someone who cares a great deal about them. This is a very cathartic experience for someone in psychic pain and a very powerful strategy for bolstering self-esteem in youth.
Empathy Role-Plays
Conclude the Module 3 PACK-Teen workshop with empathy role-plays. Refer back to the empathy formulas, feelings vocabulary, and mirroring stems, written earlier on the dry erase board. You may additionally invite parents to open their workbooks or hand them business cards from this module, to reference, during the empathy exercises. During their empathy role-plays, encourage parents initially to stick only to the empathy formulas and “mirroring,” in formulating empathic responses. Advise them to respond to the emotional reactions of their role-play partner (imaginary teens played by other parents), by “dancing” back and forth, between the two strategies. They can and should also listen with undivided attention, using their facial expressions and body language to convey their genuine interest and sustained focus. Remind them that what is most important is that they are genuine in their desire to understand and that their teen must feel convinced they have been first heard and understood, before they are capable to taking on the parents’ perspective. At the same time, parents must train themselves to inhibit their instinct to react and mentally formulate a response, during their attempt to deeply “get” their teen.
Even when directions for the role-plays are delivered clearly, concretely, and explicitly, and most parents report readily understanding the concept of empathy, on an intellectual basis, nearly all, even very sophisticated, highly educated parents, in our experience, struggle with these exercises. Even when using hypothetical scenarios, they often experience their own reaction and begin analyzing the situation presented by their role-play partner, who is playing the role of teen. To assist in overcoming the powerful instinct to view any given situation first and only from one’s own perspective the following suggestions can be made:
1. Empathic listening and mirroring requires intense, single-minded focus that never leaves the speaker and the message the speaker is conveying.
2. The listener might strive to “get it right,” “get it all,” and “get it deeply,” and approach these exercises as though they were intent in learning well, the lesson relayed by the speaker. The listener’s job is to astutely ascertain the overt, and covert messages contained within the statements made by the speaker.
3. Advanced empathic listening involves inferring what is behind or underneath the stated message. Consider the following examples:
A teen states, “You ALWAYS take little Johnny’s side!”
A parent infers, “Sounds like you feel as though you have not been treated fairly.”
A teen states, “No one asked me to the dance! I’m an ugly troll!”
A parent infers, “You’re feeling unwanted, as though no boys are interested in you.”
A teen states, “I’m never going to get in to any college!”
A parent infers, “Sounds like you are really doubting yourself and worried about your future.”
A teen states, “All my friends have turned against me!”
A parent infers, “Sounds like you feel all alone, with no friend to turn to.”
Some of the challenges, risks, potential solutions, and outcomes inherent to empathic exchanges can be understood by contemplating the following scenario, which operates in accordance with comparable principles:
A Toyota Prius and a Dodge Ram Truck are both merging onto a freeway at the exact same moment, when the on ramp unexpectedly and abruptly narrows to a single lane. That situation approximates, in principle, what typically happens during interpersonal dyadic exchanges, around disagreements. Both drivers are in a hurry and consider their mission and destination as a priority over all others. Their missions and destinations are as discrepant as their modes of transportation. However, it is impossible to determine, whose mission and destination are more worthy, more noble, more important. That decision would constitute a value judgment that can only be made through the eye of the beholder. The same premise applies in assigning value to viewpoints or feelings—there is no right or wrong—everyone is entitled to a unique perspective and no one else is qualified to judge its worthiness. All viewpoints and feelings must be considered valid and worthwhile (unless of course they violate universal moral, ethical principles). For both drivers to arrive safely at their destinations and successfully complete their missions, one must defer, temporarily, to the other. With the vast discrepancy in size and power between the two vehicles, it is intuitively obvious that the safest option would be for the Ram truck to slow itself, and its driver to suspend his agenda momentarily, for the sake of allowing the Prius to pass and merge safely. If both drivers remained hell bent on being first, on being right, on “winning,” both would surely lose … big time—one perhaps more than the other. Both would risk getting hurt, perhaps seriously and neither would arrive safely, unscathed, at their destinations or be able to fulfill their missions. For both to win, they must take turns, and such is the case in empathic exchanges, especially around interpersonal conflicts. One end of the dyad, must temporarily “press the brakes,” that is, suspend their agenda and defer to the individual on the other end, the side with less power, the person who is inherently in the “one down” position. The person with more power should then have an opportunity to say their peace and be heard and understood, safely “merge,” arrive at their destination and complete their mission. It is then and only then, that both parties can “win,” remain unharmed, and capable of realizing their goals. Turn taking must occur, and both parties must wholly commit to continuing the empathic exchange and engagement in a collaborative, creative, negotiation process, until both sides feel satisfied with the outcome. Remind the group that anything other than a “win–win” is a “lose,” in any relationship.
An example of an especially poignant and relevant role-play occurs when parents are able to identify examples of social conflicts or recent distressing events from their own lives. Initially, have two parents role-play with one relating an experience that they found distressing, while the other parent first responds with answers demonstrating “every empathy buster in the book.” Parents invariably become agitated during this exercise even though it is only a role-play. Once it has been demonstrated to parents how not to interact with their teen, have the same pair role-play the same scenario but this time with the listener expressing empathy and using mirroring.
The book’s companion website contains sample scenarios for role-play in the Module 3 PACK Therapist’s Toolbox section that can be cut out, placed in a basket, and used during this exercise. Some cards on the sheet were deliberately left blank; parents can use these cards to write down their own scenarios derived from actual experiences with their teens. Parents may be cued, to consider situations from the previous week, during which their teen became distressed or angry. It is best to start practice with “low stakes” scenarios that do not directly involve parent–teen conflict, in which it is relatively easy for the parent to be empathic.
Parents are again reminded that the goal of empathy is NOT to “put yourself in your teen’s shoes” but rather to “imagine you are your teen, in your teen’s shoes.” To this end, it is useful, prior to the beginning of each empathy role-play, to have the parent whose turn it is, to share three qualities or traits, that describe their adolescent, along with reminding the group of their youngster’s age and gender. It is also possible to have the parent don an item of clothing, accessory, body posture, or mannerism, reminiscent of their teen, to facilitate the role-plays and mastery of genuine perspective taking.
Ask parents to take turns selecting a sample scenario, pairing up with another parent, and role-playing their scenario in front of the group. While the parents role-play, you can subtly coach them in the art of expressing empathy and the use of mirroring. Encourage all of the parents to take at least one turn expressing empathy and practicing mirroring. The group members not involved in the role-play can be asked to raise their hands if they hear empathy busters. Following each role-play, which typically lasts 2–3 minutes, ask the person receiving empathy to comment on their experience, and then invite the person expressing empathy to do the same. You can additionally invite the parents who did not participate in that specific role-play to provide feedback to the role-players. If time allows, following the large group practice, it is also useful for parents to split up into small groups or pairs to rehearse empathy and mirroring.
Parents typically struggle a great deal during these exercises and often comment that the dialogue “feels awkward,” and that they “don’t know what to say.” Remind them that their assignment is just to listen and empathize. Initially, parents should rely on the empathy formulas and mirroring stems available on the board, on their handout, and on their empathy “business cards.” Remind them that if their teen is talking, they should always have something to say because their job is to listen and mirror, summarize, or paraphrase what the teen is saying. If they feel stuck, they can always simply listen with undivided attention, which they can demonstrate via maintaining eye contact, nodding, eliminating distractions, and making utterances such as “Uh-huh” or “I hear ya’.”
Before sending them out to practice with their teens over the week, remind them that an essential prerequisite for a parent to have capacity to render empathy to a youngster is that the parent be in a reasonable emotional space. If the parent’s emotional “tank” is depleted and/or he or she is in the midst of experiencing significant emotional distress him- or herself, then he or she is unlikely to be successful in efforts to emotionally support his or her adolescent. The more distressed a person is, the less able he or she is to set aside his or her own viewpoint and feelings in the service of expressing empathy and listening to the perspective and feelings of another person. The parent is wise to first check in with him- or herself regarding his or her own frame of mind and emotional well-being before embarking on a mission of empathic understanding of the teen.
Parental Resistance
Many parents struggle a great deal with the suggestion that they take the time to understand and validate their adolescent’s feelings, especially in the midst of an episode of disrespectful behavior and especially if they never received empathy from their own parents. It is very common, as you offer suggestions regarding empathy and other approaches, for parents to respond, “I’ve already tried that and it didn’t work!” It is useful to recognize that some parents seem to automatically devalue and reject anything you recommend, even before you have an opportunity to outline a particular strategy fully.
Parents who have youngsters with significant emotional and behavioral problems usually have tried a myriad of approaches, often unsuccessfully. They usually are experiencing varying degrees of defeatism and demoralization, often feeling as though they are failures as parents. It is an understandable albeit frustrating pattern for parents who feel defeated to devalue therapists as part of a psychologically defensive reaction. You would do well to expect some resistance and challenge from parents and avoid falling into the trap of entering debates or becoming defensive.
What works better is for therapists simply to listen and empathize with parents about their struggles and recognize and validate their efforts and perspectives. In addition, bear in mind that although many parents are quick to react “We tried that and it didn’t work,” on closer examination it often is revealed that they haven’t tried exactly what is being recommended. In other words, “The devil is in the details.” For example, parents may have made attempts to implement behavioral contracts but used behavioral targets such as “Be good” instead of more specific goals or provided rewards that were only delivered at the end of a month instead of more regularly, both characteristics which would have doomed the contract to fail. Parents may have tried a series of approaches, but if they lacked a sophisticated understanding of the factors inducing and perpetuating their teen’s disrespectful, defensive, and dysregulated behaviors as well as the philosophy underlying effective strategies, they were unlikely to have experienced robust and consistent success.
In addition to or as an alternative to using empathy with parents who are resistant to your suggestions, you might respond to parents by gently encouraging them to consider keeping an open mind and staying tuned in. It might be helpful to acknowledge that although many of the tools discussed might already be familiar to parents, inevitably some approaches and information will be new. It is useful to acknowledge that none of the tools taught in PACK-Teen are guaranteed to work every time with every adolescent; however, traditional, authoritarian approaches to parenting that are heavy on threats and punishments are nearly always guaranteed to fail, especially when deployed with youth who are chronically disrespectful, defiant, defensive, and dysregulated.
Family Homework
Ask that families continue a routine of identifying feelings, including as a routine check-in during family meals. In addition, encourage parents and teens to continue reflecting upon and verbalizing their emotions throughout the day, every day. Advise teens and parents to express empathy at least once daily, to one another, during the ensuing week.
Joint Session for Module 3
As detailed earlier, in the Format and Operations section, the second session of IOP each week begins with the teens and parents initially meeting separately for the sake of “checking-in” and preparing them for the subsequent “Joint” session. The “Joint” session that coincides with Module 3 is comprised of an exercise, termed “Empathy Interviews,” followed by empathy role-plays. For the first portion of the “Joint” session, pair parents from one family with a teen from a different family. It has been our experience, that conflict within families often running high and exercises requiring teens and their parents to discuss issues that are potentially inflammatory, early in treatment, can be counterproductive and experienced as too threatening. However, as families become more masterful in the emotional regulation and communication skills, they are encouraged to practice expressing empathy and resolving conflict directly with one another.
Invite the group to conduct “empathy interviews,” using the handouts provided in the book’s companion website for this module. The parent–teen pairs should take turns asking questions and jotting down the answers of their partner. The group can then be cued to come back together and each question can be read aloud and answered. What works best is to go around the circle, taking one question at a time and alternating between having a teen and then a parent (from another family), relate the answers provided to them by their partner.
The later portion of the “Joint” session for Module 3 involves empathy role-plays. Parents from one family should be initially paired with teens from a different family. Before launching the role-play exercises, remind participants of the “Empathy Formulas” and “Mirroring Stems” and encourage them to use their business cards as a reminder, should they become “stuck.” Remind the group to demonstrate exceptional listening skills, maintain consistent eye contact, stay focused, and actively track the speaker’s comments. Encourage them to use facial expressions, body language, and tone of voice to demonstrate that they are interested in hearing what the speaker has to say and are empathic regarding that person’s feelings and viewpoints.
Invite the parents and teens to take turns role-playing the expression of empathy and use of mirroring as the clinicians coach them through the exercise. The clinicians can offer to demonstrate an empathy role-play, before the group practices, to model an ideal exchange. Hand out a plastic toy microphone to each pair and instruct the group that only the holder of the microphone is allowed to speak, while their partner listens carefully for the sake of understanding, only. The “speaker” relating a story of a distressing event should share a sentence or two, then hand over the mic’ to the “listener” who should either label the “speaker’s” feelings, using empathy formulas, and/or “mirror” or paraphrase what they heard. The mic’ should be passed back and forth, serving as a concrete cue for the group, to ensure only one person speaking in each pair, at a time, and to help focus the listener on their role of empathizing and recapping the story being shared. If no mic’ is available, another alternative is to invite the speaker to signal the listener with a “thumbs up” once they feel as though they’ve been completely heard and fully understood. If the listener immediately responds to the speaker by defending themselves, or pushing their own agenda, rather than summarizing and mirroring the message shared, neither individual will feel heard and understood. It’s a process comparable to pushing together the positive poles of two magnets—they will repel no matter how much force is exerted.
Encourage the pairs to exchange feedback and “coach” one another during and at the end of each role-play. The participants can generate their own scenarios to use as examples in their rehearsals, but are cued to begin with relatively low-conflict, low-stakes scenarios, before tackling situations that have generated intense feelings and heated debates. It is only as families develop reasonable facility with empathic communication and the collaborative problem-solving approach that follows, that they should be encouraged to delve into more deeply rooted and affect-laden topics. Parents and teens can take turns expressing empathy to one another using real or hypothetical scenarios, and should be repeatedly cued to use the empathy formulas and mirroring stems, to guide their responses. Hypothetical scenarios, typical for adolescents and families with adolescents, are provided in the book’s companion website, within the therapist’s toolbox for PACK-Teen Module 3.
After individual pairs of parents and teens have role-played giving and receiving empathy independently, the group can come back together and be cued to process their experiences. In addition, one or more pairs of parent–teens can be invited to volunteer to role-play an empathy exchange, before the larger group. Ideally, families use real examples of recent conflicts that arose between them. As the final exercise for this module, have teens return to their real parents. Using the same scenario that was just rehearsed and coached with an “adopted” parent, have the teens relay their stories, while their own parents demonstrate empathic listening skills and mirroring. Once done, then have the families rehearse their roles such that parents become the speakers, while teens serve as empathic listeners. Despite how straightforward empathy might be to comprehend on an intellectual level, parents (and teens) quickly discover how incredibly difficult it can be to express empathy on the spot, in the heat of the moment. It really is hard for many parents and teens to master and worth practicing in group (and at home) again and again.
PACK-Teen Module 3 Summary Outline
Materials Needed
Established Parent Introductions and Check-Ins
• Have the introduction and check-in format for new versus established parents written on the board.
• Go around the room and have each established parent take turns doing as follows:
• Ask each parent to identify themselves by first name.
• Ask each parent to mention their teen’s first name.
• Ask each new parent to mention one “victory” or success (required) and “challenge” (optional), from the past week, related to their teen.
• If there are new parents, invite each established parent to help in orienting the new parents to the workshop format and guidelines.
• Established parents may check-in regarding their family progress, including approaches they tried which were effective thus far.
Workshop Guidelines
• Workshop consistently starts on time and finishes on time, punctuality required, leaving early or stepping out of workshop during session, not allowed.
• Confidentiality required, “What is said in here, stays in here,” playfully termed the “Vegas Rule.”
• Exceptions are safety issues (suicidality, homicidality, violence, abuse/neglect).
• Refrain from developing personal relationships with other patients while in program.
• All cell phones, pagers, electronics of any kind must be turned off during group.
New Parent Introductions and Check-Ins
• Have the introduction and check-in format written on the board.
• Take turns having each parent introduce themselves and check-in as follows:
• Ask each parent to identify themselves by first name.
• Ask each new parent to mention one positive feature or strength of their adolescent and mention one “challenging behavior” they’d like to focus on.
• Ask established parents to comment on commonalities noted during new parent check-ins.
New Parent Orientation
Parental Empathy Part II
Introduce and Discuss “Empathy Busters”
• Which behaviors are NOT empathy? (Write the list of empathy busters on the dry erase board.) Empathy busters increase frustration, lower self-esteem, erode parent–teen relationships, and block a teen’s feelings. Empathy busters include the following (use the acronym SSSSSLURPPEDD to remember):
• Solving the problem: “I’ll get you a new one.” “I’ll call her mother right now.” “I’ll fix it.” “I’ll call your principal.”
• Sympathy: “You poor thing.” “How horrible that is.” “My poor baby.”
• Sarcasm: “I’ll give you something to cry about.” “Oh, it’s just the end of the world.” “Boo hoo, whah, whah, what a crying shame.”
• Shame, blame, and put downs: “Sounds like you deserved it.” “You should have known better.” “Why did you provoke him?” “You are so selfish.”
• Scolding: “You should have known better.” “You should have studied harder.” “You should have practiced more.” “How dare you say that?”
• Lecturing: “You really need to work harder. If you don’t get your act together, you’re going to fail, and if you fail now, then you’ll grow up a failure. You should really take things more seriously.”
• Unsolicited advice: “Well if I were you….” “I think you should….” “Why don’t you just…?”
• Reassurance: “Your hair will grow back.” “There are other fish in the sea.” “Nobody will notice.” “There will be other games (or tests, friends, dances, and so forth).”
• Philosophy lesson: “Life is like that.” “Everything happens for a reason.” “This setback will make you stronger.” “It was God’s will.” “Big boys don’t cry.”
• Psychoanalysis: “Did it ever occur to you that the real reason…?” “You’re only saying that because….” “You’re just upset because….”
• Enemy (Defending the…): “What did you do to invite that?” “The teacher was just trying to….” “No wonder Johnny did that.” “You probably asked for it.” “I’m sure she didn’t mean it.”
• Dismissing feelings: “It’s not that big a deal.” “You shouldn’t feel that way.” “I’ll give you something to cry about.” “Get over it.”
• Detective: “So what happened?” “Why are you so mad (upset, sad, frustrated)?” “So what are you going to do?” “Why didn’t you study harder?”
• Important note: Feelings are not right or wrong; they just are. If the teen detects you are not validating his or her feelings, he or she will become more upset and simply work harder to convince you that he or she has a good reason to be upset (i.e., up the ante).
• “Business cards” outlining these empathy busters are available digitally in the PACK-Teen Therapist’s Toolbox on the book’s companion website. These cards can be cut out and handed to parents to serve as reminders during the workshop as well as at home.
Review the Empathy Test
• Go around the circle and have parents take turns reading the question and each answer.
• As they read the potential answers out loud, have them indicate whether the answer represents parental empathy or an “empathy buster.”
• If they indicate the answer is an “empathy buster,” have them specify which one(s).
• Some answers might sound like examples of more than one “empathy buster.”
Identifying Feelings in Others
Review the Empathy Formulas
Feelings Vocabulary
• Discuss how parents can help their teen build his or her feelings vocabulary.
• Brainstorm a list of feelings words. These might include mad, sad, happy, frustrated, or disappointed.
• What if you get the feeling wrong? No harm done. The teen will quickly correct you and will still appreciate that you are trying to understand and validate his or her feelings.
• If needed, provide parents with the feelings handout located on the book’s companion website as PACK-Teen, Module 1, Hand-out #3 or have them reference it, if already provided a copy at a previous session.
• Discuss how using the word “No” or the phrases “You can’t…” or “You must…” increase arousal and generate defiance.
• Discuss how parents need to demonstrate a willingness to put their teen’s concerns on the table.
• The best way to get someone to listen to your concern is to first demonstrate you hear and are willing to consider their concern.
Review Adolescent Responses to Empathy Busters
Define and Discuss Mirroring
• Repeating back parts of something someone has said or paraphrasing.
• Allows teens to hear their own words.
• Defuses upset and demonstrates the parent’s full attention and listening.
• Shows that parents have no agenda except to follow and understand what has been said (parents should not argue, reassure, lecture, or so forth—just listen).
Introduce and Discuss “Mirroring Stems”
Discuss “Metamessages” (Implied or Underlying Fears/Concerns)
Discuss the “Top 10” Barriers to Parent–Teen Empathy and Strategies to Overcome
Discuss the “3-Minute Rule”
Sample Empathic Communication Script
Here is a sample dialogue that you can invite two parents to read and act out aloud for the group:
Scenario: You have recently informed your 15-year-old daughter of the need to move out of state.
Parent A (15-year-old girl): “I just can’t leave my friends. I’m never moving. You’ll have to go on without me.”
Parent B (mother): “You sound really upset.”
Parent A: “Yeah I’m upset. Wouldn’t you be? I’m so mad. You and Dad are ruining my life.”
Parent B: “Your friends mean the world to you, and you can’t bear to leave them.”
Parent A: “That’s right. My friends are the most important thing—more important than my family.”
Parent B: “No one can take the place of your friends.”
Parent A: “Especially Jean. She’s been my best friend since kindergarten. I could never find another friend like her. I’ll be lost without her.”
Parent B: “Jean is a really special friend—the kind that only comes along once in a lifetime.”
Parent A: “I can’t leave her. I won’t have anyone to talk to or hang out with.”
Parent B: “Not seeing Jean every day is going to be hard on you. I wonder if there’s anything you could do to make it easier on both of you?”
Parent A: “Nothing will help. Not moving is the only thing.”
Parent B: “You seem heartbroken. Maybe you and Jean can put your heads together and figure out a way to make this move a little less hard on both of you.”
Parent A: “Can I come back and stay with her all summer?”
Parent B: “Visiting each other may be an option.”
Parent A: “I’m going to call her right now. Maybe we could make scrapbooks for each other.”
Parent B: “Or get cell phones with unlimited long distance.”
Parent A: “Really? That would help … a little.”
Role-Play Empathy and Mirroring
• Review the principles of empathic exchanges, that is, the need to take turns, wholly listening for the sake of understanding and empathizing before relating one’s own agenda.
• Ask parents to identify examples of distressing situations. Use these situations to illustrate the empathy busters, then empathy and mirroring.
• Sample scenario cards are available in the Module 3 PACK-Teen Therapist’s Toolbox on the book’s companion website.
• Discuss “What About My Teen?” examples.
• Have parents pair up and take turns practicing expressing empathy and using mirroring in front of group.
• Have parents break out into small groups to practice further.
Review the PACK-Teen Mantras
Review, Answer Questions, and Wrap Up
Family Homework
• Encourage families to post a comprehensive vocabulary of feeling words (provide handouts from book’s companion website) on their refrigerator or in another obvious, highly trafficked area.
• Ask each family member to identify his or her current feeling while checking in during family meals regarding their day. In addition, encourage parents and teens to reflect upon and name their emotions throughout the day every day.
• The parents are encouraged to schedule family meals, at least weekly, where all members gather at a table and each person takes a turn sharing the best and worst parts of their day, to model and facilitate practice of conversation and listening skills.
Joint Session for Module 3
• Pair teens with parents from different families, or “adopt” another parent/s.
• Hand-out worksheets for “Empathy Interviews” and have the group perform these, writing down answers.
• Have the group join back together and go around the room, one question at a time, having the teens report on the parents and vice versa.
• Set up for empathy role-plays by reviewing good listening skills, empathy formulas, mirroring stems with the whole group and writing them on the board.
• Also provide copies of either “business cards” or handouts with empathy formulas, mirroring stems, and a feelings vocabulary.
• Invite the parent–teen “adopted” pairs to role-play giving and receiving empathy using either sample empathy scenarios or their own examples, using toy microphones to ensure only one member of each pair is speaking at any time.
• Encourage the pairs to offer feedback regarding what went well and what didn’t, including providing constructive, affirmative suggestions for future empathic communication.
• Invite teens and parents to report to the group, regarding their experiences.
• Have teens return to their own parents and repeat the same exercise, incorporating feedback from their “adopted” parent and then have the pairs rehearse roles.
• Encourage them to initially practice, including at home with their real parents, “low-stakes” agenda items, then graduate to medium- and finally “high-stakes” issues, as they increase their comfort, ease, and mastery of empathic communication techniques.
Handouts/Business Cards
Module 3-PACK-Teen Parent Handout #10
Multiple Choice Test on Empathy
Directions: Select the answer that would be most typical for you, in response to statements by your teen.
1. “I was completely humiliated today when Susan announced I had a huge zit!”
c. Sounds like you felt really embarrassed.
2. “The idiot coach didn’t play me the whole game!”
a. Maybe if you practiced more…
b. I’m sure he knows what he’s doing.
c. You must be really disappointed.
3. “I’m going to kill Joey for using my iPod!”
a. You shouldn’t be so selfish!
b. You seem really frustrated.
c. He’s little and doesn’t know any better.
b. You should go anyway. I’m sure you’ll have fun!
c. You think school dances are stupid, huh?
5. “I have a math final tomorrow and I’m gonna’ fail!”
a. Relax. I’m sure you’ll do well.
b. If you had spent more time studying, you wouldn’t be worried now.
c. You sound worried. I’ll bet you wish it were over & done with.
6. “I’m gonna’ run away from home!”
b. You’re being silly. I don’t want to hear that kind of talk.
c. You sound very unhappy. I’ll bet you wish a lot of things were different around here.
Module 3-PACK-Teen Empathy Buster Summary Cards Therapist Tool #3
Module 3-PACK-Teen Parent Handout #11
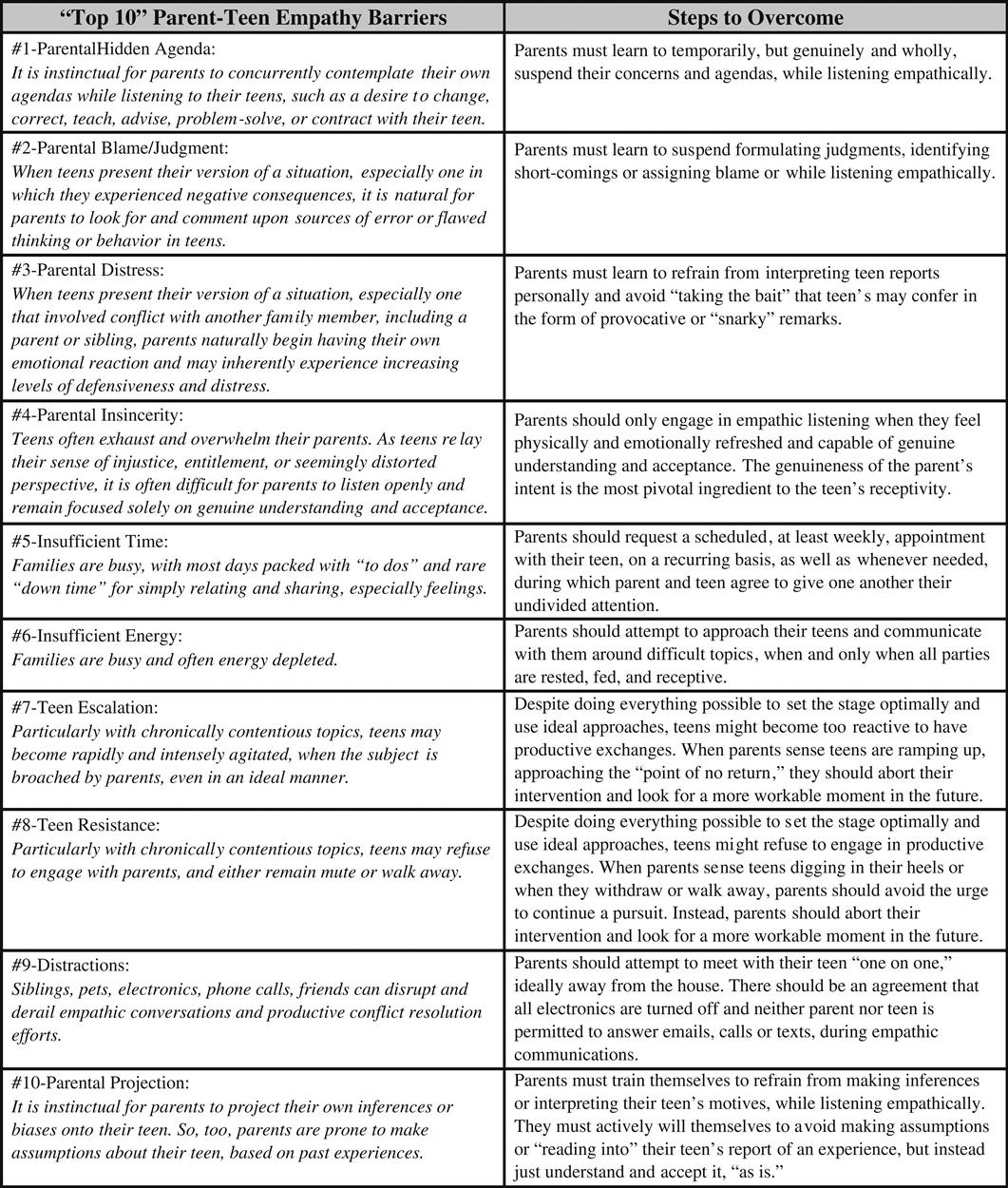
Module 3-PACK-Teen Parent Handout #12
Parental Empathy in a Nutshell
• To understand what another person is experiencing (feeling, thinking).
• To convey to another person in words that you understand what he or she is experiencing (feeling, thinking).
• Empathy is NOT “Putting yourself in someone else’s shoes,” but rather “Imagining you are someone else (i.e., your teen), in someone else’s shoes.”
Important Note: Feelings are not right or wrong; they just are. If a teen detects you are not validating his or her feelings, he or she will become more upset and simply work harder to convince you that he or she has a good reason to be upset (upping the ante).
• Defuse a potentially explosive situation
• Make an empathic connection and/or a stronger relationship
• Help the teen build his or her feelings vocabulary
• Teach the teen to discuss and/or process intense negative feelings rather than act them out
• Build self-esteem (“My feelings and/or thoughts matter, so I matter!”)
• “You seem__________(feeling word).”
• “You sound_________(feeling word).”
• “You look__________(feeling word).”
• Fill in the blank with a feelings word (e.g., mad, sad, glad, frustrated).
Empathy Busters (S.S.S.S.S.L.U.R.P.P.E.D.D.)
• Sympathy: “You poor thing.” “How horrible that is.” “My poor baby.”
• Sarcasm: “I’ll give you something to cry about.” “Oh, it’s just the end of the world.” “Boo hoo, whah, whah, what a crying shame.”
• Shame, blame, and put downs: “Sounds like you deserved it.” “You should have known better.” “Why did you provoke him?” “You are so selfish.”
• Scolding: “You should have known better.” “You should have studied harder.” “You should have practiced more.” “How dare you say that?”
• Lecturing: “You really need to work harder. If you don’t get your act together, you’re going to fail, and if you fail now, then you’ll grow up a failure. You should really take things more seriously.”
• Unsolicited advice: “Well if I were you….” “I think you should….” “Why don’t you just…?”
• Reassurance: “Your hair will grow back.” “There are other fish in the sea.” “Nobody will notice.” “There will be other games (or tests, friends, dances, and so forth).”
• Philosophy lesson: “Life is like that.” “Everything happens for a reason.” “This setback will make you stronger.” “It was God’s will.” “Big boys don’t cry.”
• Psychoanalysis: “Did it ever occur to you that the real reason…?” “You’re only saying that because….” “You’re just upset because….”
• Enemy (Defending the…): “What did you do to invite that?” “The teacher was just trying to….” “No wonder Johnny did that.” “You probably asked for it.” “I’m sure she didn’t mean it.”
• Dismissing feelings: “It’s not that big a deal.” “You shouldn’t feel that way.” “I’ll give you something to cry about.” “Get over it.”
• Detective: “So what happened?” “Why are you so mad (upset, sad, frustrated)?” “So what are you going to do?” “Why didn’t you study harder?”
Adapted with Permission from Cook, M. (2012). Transforming Behavior: Training Parents and Kids Together, Brookes Publishing, Baltimore, MD.
Module 3-PACK-Teen Empathy Summary Cards Therapist Tool #4
Module 3-PACK-Teen Empathic Communication Script Parent Handout #13
Sample Parent-Teen Empathic Communication Script:
Scenario: You recently informed your 15-year-old daughter of the need to move out of state.
Parent A (15 yo girl): “I just can’t leave my friends. I’m never moving. You’ll have to go on without me.”
Parent B (mother): “You sound really upset.”
Parent A: “Yeah I’m upset. Wouldn’t you be? I’m so mad. You and Dad are ruining my life.”
Parent B: “Your friends mean the world to you, and you can’t bear to leave them.”
Parent A: “That’s right. My friends are the most important thing—more important than my family.”
Parent B: “No one can take the place of your friends.”
Parent A: “Especially Jean. She’s been my best friend since kindergarten. I could never find another friend like her. I’ll be lost without her.”
Parent B: “Jean is a really special friend—the kind that only comes along once in a lifetime.”
Parent A: “I can’t leave her. I won’t have anyone to talk to or hang out with.”
Parent B: “Not seeing Jean every day is going to be hard on you. I wonder if there’s anything you could do to make it easier on both of you?”
Parent A: “Nothing will help. Not moving is the only thing.”
Parent B: “You seem heartbroken. Maybe you and Jean can put your heads together and figure out a way to make this move a little less hard on both of you.”
Parent A: “Can I come back and stay with her all summer?”
Parent B: “Visiting each other may be an option.”
Parent A: “I’m going to call her right now. Maybe we could make scrapbooks for each other.”
Parent B: “Or get cell phones with unlimited long distance.”
Parent A: “Really? That would help … a little.”