Q5. What is dementia?
A5. “Dementia” is an umbrella term that refers to any disease that has these 4 characteristics:
There are 100 or more diseases that cause dementia. All meet these 4 criteria, but they differ in the specific aspects of thinking they impair, in the neurological symptoms they cause, in how rapidly they progress, in what causes them, and in how they are treated.
There are more than 99 causes of dementia. The 4 most common are Alzheimer disease, Lewy body dementia, vascular dementia, and frontotemporal dementia.
Alzheimer disease is the most common cause of dementia. The diagnosis of definite Alzheimer disease requires evidence of the specific changes in the brain described in Q7, but when a doctor uses the following criteria when assessing a patient, the diagnosis agrees with what is found later, at autopsy, more than 90% of the time:
1. A slowly progressive dementia, which means that the person has had slowly worsening memory or other cognitive (thinking) difficulties for more than 6 months.
2. Lack of evidence of any of the other 99 causes of dementia after physical, neurological, and psychiatric examinations, and on laboratory testing and brain imaging.
3. The presence of memory impairment plus at least one of the following:
• impairment in executive function (abstraction, judgement, initiation, and persistence and stopping of thought or action);
• impairment in language expression (called “aphasia”);
• impairment in doing everyday activities (called “apraxia”) that is not attributable to impaired strength or sensation;
• impairment in accurately perceiving the world visually (called “visual agnosia”).
4. If under age 70, a positive amyloid PET scan or spinal fluid markers supporting the presence of Alzheimer disease.
Q6. Does every case of Alzheimer disease begin with memory impairment?
A6. While the vast majority of people with Alzheimer disease have difficulty remembering new information as their first symptom, not everyone does. Occasionally, the first symptom is difficulty finding and expressing words (see Q18), difficulty accurately perceiving the world around them, declining ability to function at work or home (see Q8), or apathy.
Q7. Is it true that Alzheimer disease can be diagnosed only at autopsy?
A7. If the doctor follows the criteria described in Q5, then autopsy confirms the diagnosis of Alzheimer disease made during life about 90% of the time. In the remaining 10%, one or several of the other diseases that cause dementia are present. It is likely that some combination of amyloid PET scan (see Q9 and Q10), tau PET scan, or spinal fluid measures of amyloid and tau breakdown products will improve the accuracy of diagnosis made during life in the near future, but the usefulness of such testing has not yet been proven.
Microscopic findings in 3 diseases that cause dementia. Neuritic plaque (top left) and neurofibrillary tangles (top right) are characteristic of Alzheimer disease, cortical Lewy bodies (bottom left) are characteristic of dementia with Lewy bodies, and Pick bodies (bottom right) are characteristic of frontotemporal dementia (FTD). Courtesy of Dr. Richard E. Power and Dr. Olga Pletnikova.
At autopsy, Alzheimer disease is characterized by abnormal structures called “neuritic plaques” and “neurofibrillary tangles” that are found in specific areas of the brain. The plaques consist of a core of amyloid protein surrounded by a mixture of the breakdown products of brain cells. They are located in the tissue between cells. The tangles consist of twisted fibrils of the protein tau. These are located within cells. Q26 discusses these structures in more detail.
Q8. I have heard that there are stages of Alzheimer disease. How are they identified?
A8. There are several widely used descriptions of how Alzheimer disease progresses. Each has strengths and weaknesses. I favor a 3-stage model that was first described in the early 1950s.
Significant variability occurs in all diseases, so any description of staging must be understood as a broad generalization. The average person with Alzheimer disease lives about 10 years, and each stage averages about 3 years in duration. However, some people go from first symptom to death in 3 or 4 years and others live for more than 20 years.
People in this stage have difficulty learning new information but remember information from the more distant past. People also have difficulty organizing more complicated activities and may make subtle social errors.
Executive function refers to a set of abilities that are crucial to organizing life. They include knowing when to start, continue, change, and stop an activity, as well as the abilities to abstract, generalize, and detect social cues.
People in this stage often remain independent, but their ability to do so declines as the disease progresses. People should be encouraged to continue doing activities they have always enjoyed, to participate in family events, and to remain socially active as long as there is no significant risk of harm to them or others. Some people are able to work but may require increased supervision.
This stage is characterized by impairments in 3 distinct aspects of cognition: language, praxis, and visual perception. Since people vary in the extent to which each capacity is impaired, it is important to identify each individual’s remaining abilities and limitations in each. The symptoms of this stage are referred to as “cortical” because these functions of the brain are located in the outer layer of the brain, the cortex.
Language: People with Alzheimer disease can develop problems both expressing themselves with words and understanding what is being said to them. These language impairments are referred to medically as “aphasia.” They are similar to what happens when people have a stroke or other injury in the brain’s language area.
These impairments in language make it difficult for people to express what they want to say. People with aphasia will sometimes say a word they do not mean to say, will sometimes say words that have no meaning, or will not be able to express what they want to say. Aphasia can result in a person’s being unable to answer questions accurately. For example, the person might not be able to say that they are in pain or to describe when and where it hurts.
Communication with a person who is having trouble expressing and understanding spoken language can often be improved by:
People who are unable to understand what is said to them will have difficulty following directions. This can be tested for by asking them to carry out a multistep request. For example, if asked to “Please take the dishes into the kitchen and bring out the dessert,” they may do one step but not the other or may just stare at the person making the request.
Communication with a person who is experiencing an aphasia, or language impairment, can often be improved by speaking in short phrases or sentences rather than in long, complex sentences; succinctly repeating what you have said or asked; using nonverbal communication, such as visual cuing (pointing, for example) and touch; and asking the person to do one task at a time rather than making requests that involve multiple steps. Speech-language pathologists, psychologists, nurses, and doctors can help identify ways to improve communication with a specific individual.
Praxis: The word “apraxia” refers to the inability to carry out a learned physical (or “motor”) activity even though strength and sensation are normal. Examples include difficulty dressing, cooking, bathing, and using eating utensils. Like all symptoms in Alzheimer disease, these impairments develop gradually. A person may still be able to do parts of the activity but not the most complicated aspects of it. For example, a person may be able to put on pants or a blouse but not be able to put on a belt or bra, or use a zipper.
When observing a person with an apraxia, you can often figure out what they can still do on their own and what they need help with. If a person is having difficulty dressing, for example, observe whether they can put on slacks but not a belt.
The goals of helping people with impaired abilities are to maximize their independence while simultaneously helping them accomplish what they cannot do on their own. For example, a person developing difficulty using eating utensils will gradually lose these skills over months or years. The most complex task is using a knife, while the simplest is using a spoon. For people developing difficulty using a knife but still able to use other utensils, cutting their food in the kitchen before bringing it to the table will enable them to feed themselves with a fork and spoon. This means they are fully independent. Since there is no knife at their place setting, you have also helped them avoid the utensil they have difficulty with.
“Talking people through” tasks they are having difficulty with—that is, explaining each step as you go—may calm them and allow them to accept help with dressing, bathing, getting up from a chair, and feeding themselves.
Visual Perception: People with Alzheimer disease gradually develop difficulties in several aspects of visual perception. These impairments are called “agnosias.” Some people with agnosia are unable to recognize familiar faces or places. Others are unable to observe more than one thing at a time even though there are several objects in front of them. For example, they may report that there are only peas on a plate when there are also several other items on the dish. People with agnosias might recognize people by their voices but not by looking at them.
The goal of helping people with impaired abilities is to allow them to do everything they can while helping them accomplish what they cannot.
Being unable to recognize familiar places means that the person can never be in a familiar environment. This is a common source of distress in people with dementia, but hugging the person, engaging them in conversation, and finding activities they are able to enjoy can help them feel connected.
Problems in walking, controlling urination and bowel movements, and swallowing develop gradually in this stage. People do not necessarily develop all of these impairments, and it is not possible to determine who will and will not develop any of them.
People with stage 3 symptoms need more physical support. They may need help with toileting and walking. As the stage progresses, food may need to be cut in very small pieces or pureed to aid in swallowing. Falls become common and some people lose the ability to walk.
Q9. How do brain scans work? Can they detect dementia and specific causes of dementia?
A9. Brain scans rely on a variety of atomic particles to visualize the contents of the brain. Standard X-rays can distinguish bone from water, but they do not visualize brain tissue, because it is mostly water.
CT scans of the brain take multiple X-ray pictures from different angles. A computer program then takes this information and generates a picture of the soft tissue of the brain and of the bones of the skull.
MRI scans use a strong magnet to generate a very brief magnetic field. This “lines up” water molecules and results in an image that can be captured on a computer screen. MRI scans can directly visualize brain tissue, flowing blood, and actively working brain cells.
Neither CT scans nor MRI scans can diagnose Alzheimer disease. They can detect old and new strokes, brain tumors, brain abscesses, normal pressure hydrocephalus (NPH), and subdural hematomas (collections of blood between the lining of the brain and brain tissue which press on the brain and cause symptoms).
PET scans rely on radioactive chemicals that are linked to some other compound of interest and injected into a person’s bloodstream. These radioactive compounds emit a particle called a “positron” that is converted into pictures.
Glucose (fluoro-deoxy glucose, or fdg) PET scans can detect distinct patterns of diminished brain metabolism compatible with Alzheimer disease and frontotemporal lobar dementia.
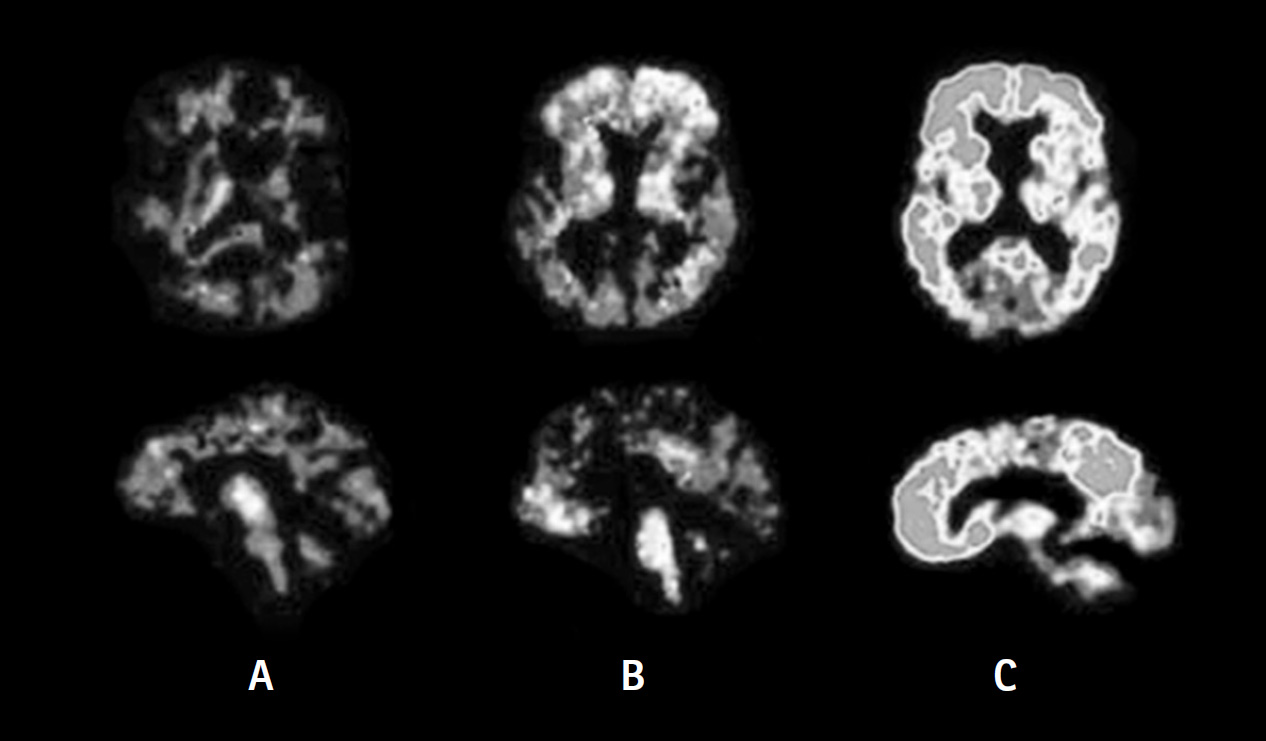
Amyloid-beta PET scans showing a range of amyloid deposits in the brains of those with normal cognition or with Alzheimer disease. A shows no evidence of amyloid deposits in the brain of someone with normal cognition. B shows some evidence of amyloid deposits in the brain of someone over age 70 with normal cognition. C shows significant amyloid deposition in the brain of someone with Alzheimer disease.
Amyloid PET scans show if the abnormal protein is located in the brain and, if so, where it is.
SPECT scans use radioactive particles called “photons.” The images are less detailed than those produced by PET scans and are less expensive. SPECT scans are used to diagnose dementia with Lewy bodies and Parkinson disease dementia.
Q10. Why is the amyloid PET scan only helpful if the person is under age 70?
A10. After age 70, many people who are normal in their thinking have “positive” amyloid PET scans, meaning the scans show that they have beta-amyloid deposited in their brains. This is shown in the figure in Q9. It is not currently known whether all individuals over age 70 who have normal thinking but an abnormal amyloid PET scan will eventually develop Alzheimer disease.
Q11. If there is no blood test for Alzheimer disease, why was blood drawn when my husband was evaluated?
A11. Blood is drawn as part of the evaluation of dementia because a number of medical diseases can cause the symptoms of dementia. Among these are vitamin B12 deficiency and diseases of the thyroid, kidney, liver, and adrenal glands. Blood tests can detect these and other potential causes of dementia that can be treated. Some uncommon causes of dementia have specific blood tests that the doctor might order if they are suspected. Blood levels of certain medications are available and can determine if the dosage is too high and possibly causing cognitive impairment. Scientists are working to develop blood tests to help diagnose Alzheimer disease but so far they have not proven accurate enough.
Q12. Are there specific tests to diagnose the other 99 forms of dementia?
A12. Each of the other forms or causes of dementia has a distinct clinical picture that is different from Alzheimer disease. As a result, making the correct diagnosis depends on:
Everyone with possible dementia should have a thorough assessment because a potentially treatable cause of their symptoms might be detected.
Q13. Does mild cognitive impairment (MCI) fit under the dementia umbrella? What is the likelihood that a person with MCI will develop a dementia?
A13. MCI is best thought of as a condition between normal aging and dementia. The evaluation for MCI and dementia are the same, but in MCI:
The technical definition of MCI requires that the person has a decline of 1.5 to 2 standard deviations on a test of cognitive performance compared to people who are similar in age and education. This indicates a 30% to 65% likelihood that the decline is meaningful compared to the 95% likelihood that is required for a diagnosis of dementia.
About 10% of people with MCI develop dementia each year after the diagnosis of MCI is made. This means that about 50% of people with a diagnosis of MCI will meet criteria for dementia by the fifth year after diagnosis. In those people with MCI who develop dementia, Alzheimer disease is often the underlying disease, but MCI can also be the earliest symptom of other illnesses causing dementia, including vascular dementia, dementia with Lewy bodies, and Parkinson disease dementia.
About 25% of people who meet criteria for MCI return to normal a year later, but these individuals are still at increased risk of developing dementia in the long run.
Q14. I took my wife to our local memory evaluation center and they recommended neuropsychological testing. It seems expensive. Should we go through with it?
A14. There are 2 levels of cognitive testing. Primary care physicians, neurologists, geriatricians, and psychiatrists administer short cognitive tests that take 5 to 10 minutes. These tests assess abilities in memory, executive function, perception, and language (see Q8).
Neuropsychologists are trained to administer batteries of tests that are much more detailed and comprehensive. The results of this testing are very helpful in certain circumstances but are often not necessary for making an accurate diagnosis, assessing the severity of the dementia, or making treatment recommendations. Because this testing is expensive and time consuming, I recommend it only in the circumstances mentioned below.
The tests administered by neuropsychologists are particularly helpful in distinguishing normal aging from the earliest signs of mild cognitive impairment (MCI) and dementia (see Q2). In-depth testing is helpful when a person has, or is suspected of having, depression, since certain tests can help distinguish a mood disorder from a cognitive disorder—or may suggest that both are present. Neuropsychological tests are also helpful in identifying which aspects of cognition are relatively unaffected and which are more severely impaired. This determination can help identify a specific cause of dementia.
Neuropsychological testing is particularly helpful in unusual situations, for example when someone is young, having trouble at work, or experiencing symptoms whose cause is unknown. Even if it is unclear whether someone is experiencing the earliest symptoms of MCI or dementia, neuropsychological tests can provide baseline data to which subsequent testing can be compared.
Q15. My mother has been diagnosed by her primary care doctor as having vascular dementia. Does it really matter what the cause of dementia is?
A15. Vascular dementia is the most difficult cause of dementia to diagnose accurately. Even when dementia experts diagnose vascular dementia, they are wrong 25% to 50% of the time, if autopsy is used as the standard. Most often the correct diagnosis is Alzheimer disease. However, in the past decade it has become clear that the relationship between Alzheimer disease and vascular dementia is complicated. They occur together more than would be expected by chance. This has led many experts to conclude that brain vascular disease likely contributes to the development of Alzheimer disease.
Vascular dementia is most accurately diagnosed when there are signs of prior stroke on the neurological examination and evidence of one or more strokes on a brain MRI or CT scan. Some doctors, however, make the diagnosis when there is evidence on a brain MRI of changes compatible with brain vascular disease without evidence of stroke. I believe that anyone with a diagnosis of probable vascular dementia should be carefully assessed for the presence of Alzheimer disease and that the treatments for Alzheimer disease be considered, because both diseases might be present.
I do believe it is important to obtain as accurate a diagnosis as possible. If the diagnosis is vascular dementia and future strokes can be prevented, then the person will not decline. Some causes of dementia, including normal pressure hydrocephalus (NPH) (see Q92) and chronic subdural hematoma, can be surgically treated. An accurate diagnosis also determines whether anti–Alzheimer disease medications or anti–Lewy body dementia medications are prescribed. Obtaining an accurate diagnosis helps predict the future development of new symptoms, information that is important for care planning.
Q16. What is Lewy body dementia? How is it diagnosed and treated?
A16. Dementia with Lewy bodies (DLB) was identified as a common cause of dementia in the 1980s. The Lewy body is the microscopic pathological hallmark of Parkinson disease, and in Parkinson disease it is generally seen in a very specific area of the brain called the “substantia nigra,” so named because it normally looks black.
DLB was first identified when a group of doctors in England noticed that some patients they had diagnosed with Alzheimer disease when living had Lewy bodies (see the figure in Q9) in the outer layer of their brain, the cortex, at autopsy. When these doctors looked at the medical records of these patients, they realized that visual hallucinations and mild parkinsonism (meaning Parkinson disease–like symptoms) were present in almost all the patients, usually very early in the disease.
DLB is diagnosed when dementia and Parkinson-like symptoms develop within one year of each another. About 85% of people with DLB experience visual hallucinations. The dopamine transporter SPECT scan (DAT scan) (see Q9) is abnormal in dementia with Lewy bodies.
Q17. Does Parkinson disease cause dementia?
A17. Experts argued about this question before there were good treatments for Parkinson disease, because it was difficult to distinguish between the slowing down and soft voice characteristic of Parkinson disease and changes in thinking characteristic of dementia. Because they are so effective, the drug treatments for Parkinson disease have dramatically improved quality of life, diminished the movement symptoms, and extended life span, but they also revealed that half or more of people with the illness will develop declining cognition at some point in the disease. This is referred to as “Parkinson disease dementia (PDD).”
Many people with Parkinson disease do not develop cognitive decline, even after years of physical symptoms. Some people with Parkinson disease also develop Alzheimer disease, because both diseases become common as people age. People with the dementia of Parkinson disease have difficulty accessing what they know and early problems with visual perception. Many people with Parkinson disease are able to come up with correct answers or perform activities correctly, if given time. This is not dementia, it is slowing.
Parkinson disease dementia is diagnosed when a person has had Parkinson disease for more than one year before the symptoms of dementia begin. People with Parkinson disease dementia usually have impairments in memory, executive function, and perception but not in language or praxis (see Q8 for a discussion of these symptoms). The dopamine transporter SPECT scan (DAT scan) is abnormal in both Parkinson disease and Parkinson disease dementia (see Q9).
Mental and physical slowing may be caused by Parkinson disease, but this is not the same thing as dementia. Many people with Parkinson disease are able to come up with the correct answer or do something correctly if they are given time. This is not dementia but slowing.
Q18. What is frontotemporal dementia? What are tauopathies?
A18. Frontotemporal dementia (FTD), also called “frontotemporal lobar dementia (FTLD),” refers to a group of diseases with different clinical symptoms but with similar microscopic abnormalities. Distinctive abnormalities are found on the glucose (fdg) PET scan and MRI (see the figure in Q9).
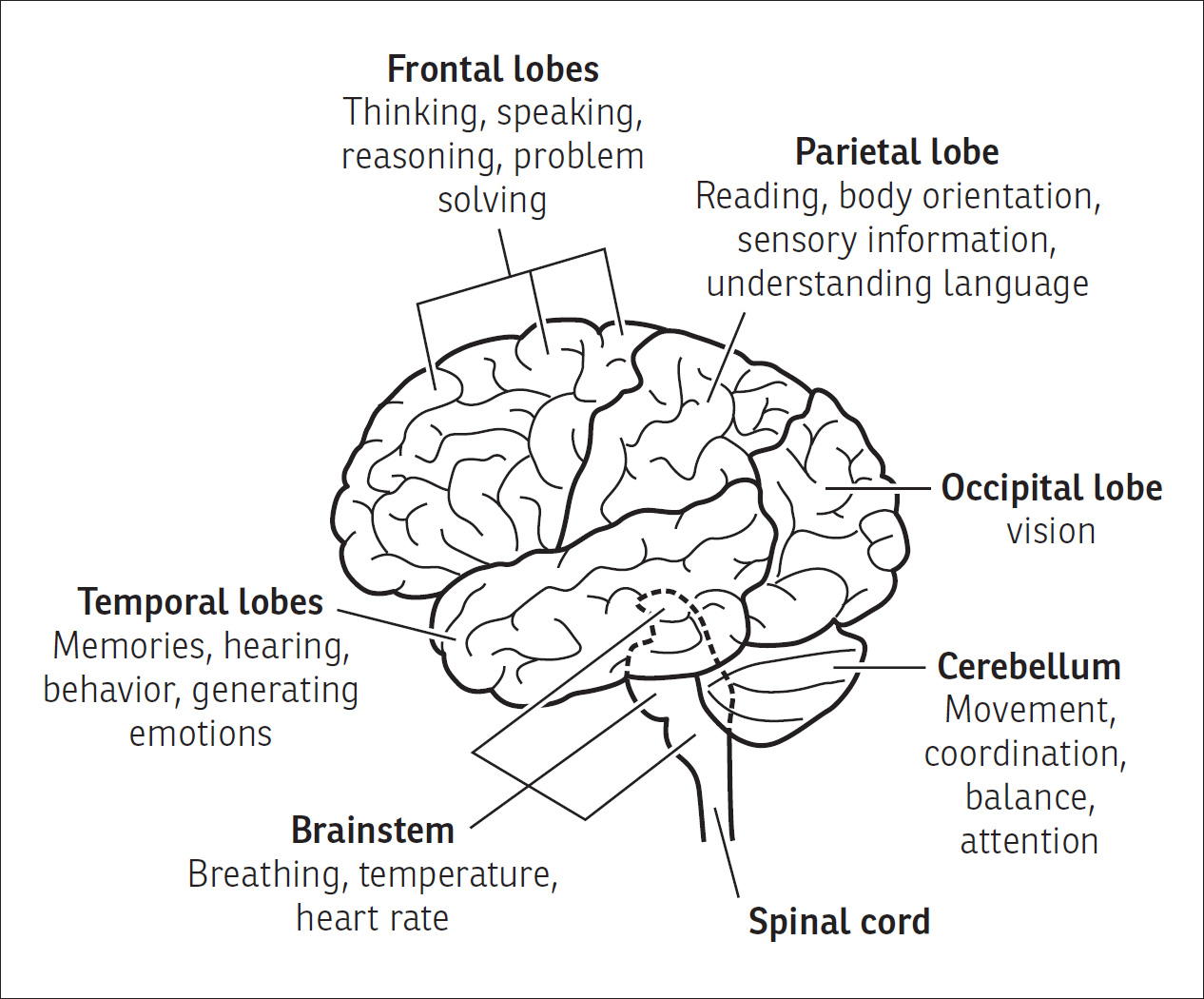
The name of the disease derives from the primary location of the brain abnormalities. FTD starts in the frontal lobes, temporal lobes, or both. By contrast, Alzheimer disease originates in deeper structures of the brain and abnormalities are seen in the parietal lobes on PET scans.
In the early stages of FTD the symptoms can often be divided into two categories. The language variant of FTD begins with impairments in the expression or comprehension of spoken language. In some forms of this variant, people are aware of their speaking difficulties and become frustrated, but in other forms they are unaware of their deficits.
The behavioral variant of FTD begins in the frontal lobes, the part of the brain that controls executive function, the aspects of thinking that oversee, supervise, and coordinate cognitive function (see Q8 and Q18). Intact executive function underlies mental flexibility and the understanding of social cues. Given the complexity and subtlety of executive function, it is not surprising that the symptoms can be difficult to detect at the beginning of the disease. Early manifestations of impaired executive function include apathy (difficulty initiating activity), inflexibility in situations that are taxing, socially inappropriate language or behavior, inappropriate spending, and difficulty meeting the demands of work, house upkeep, or paying taxes.
Memory is often intact in both variants during the first several years of the disease. This is an example of why memory loss is not required for making a diagnosis of dementia. Over time, though, people usually develop symptoms of both variants.
At present, about one-third of people with FTD have a genetic cause for their disease, but in the majority of people with FTD, no cause can be found.
At autopsy, FTD is characterized microscopically by tau protein deposition, loss of cells in the frontal and/or temporal lobes, and a bubbly pattern referred to as “granulovacuolar degeneration (GVD)” (see the figure in Q7). Some people with FTD also have Pick bodies (another microscopic abnormality which was first described by Dr. Alzheimer in 1911) and/or the abnormal protein TDP-43.
The term “tauopathy” is used to refer to any disease characterized by tau protein deposits seen under the microscope. In addition to FTD, one of these diseases is progressive supranuclear palsy (PSP). People with this disease become stiff, have a backwards curved neck, move and think slowly, and lose the ability to voluntarily move their eyes. Cortical basal ganglionic degeneration (CBD) is another tauopathy. People with CBD are unable to recognize or use their arm or leg even though there is no evidence of weakness in that limb.
Q19. What is amyloid angiopathy? My father was diagnosed last year at age 51 and can no longer live by himself.
A19. Cerebral amyloid angiopathy (CAA) is a disease in which repeated strokes lead to dementia. It is caused by the deposition of the beta-amyloid protein along the walls of blood vessels in the brain. These deposits weaken the blood vessel walls and cause them to burst. The resulting bleeding within the brain is called a “hemorrhagic stroke.”
CAA usually develops in midlife. Because they have experienced multiple strokes, people with CAA often become unable to care for themselves within several years.
Some people with more classic Alzheimer disease also have amyloid deposition along the smaller blood vessels in their brain. This might be one reason that Alzheimer disease and vascular dementia occur together more often than they should occur by chance.
At present there is no treatment for the disease. Keeping blood pressure low does not prevent the bleeding into the brain. Whether amyloid-lowering drugs will lower the risk of strokes has not yet been determined.
Q20. What is CTE?
A20. It has been known for more than 100 years that boxers are at increased risk of developing dementia. More than 60 years ago, brain autopsy studies of boxers revealed the presence of neurofibrillary tangles, one of the abnormalities seen in Alzheimer disease. In the past this dementia was called “dementia pugilistica” because of its association with boxing, but now it is called “chronic traumatic encephalopathy (CTE).”
CTE has received a lot of attention in recent years because it appears to be associated with repeated head trauma in athletes playing American football, ice hockey, and soccer. There is increasing evidence that individuals who have experienced repeated concussions and head trauma in other settings are also at increased risk. At autopsy, which now is the only way to confirm the diagnosis, deposits of the tau protein are found deep within the folds of the brain.
The relationship between these disorders and Alzheimer disease is not clear and is being studied intensively. Both CTE and Alzheimer disease are characterized by tau deposits, but the deposits are usually located in different places in the brain. People who die from Alzheimer disease usually also have neuritic plaques at autopsy. Memory impairment is usually the first symptom of Alzheimer disease but may not be in CTE. Since many fewer people with CTE have been studied, it is difficult to make general statements about the disease at present. It is thought that the earliest symptoms of CTE are related to damage directly or indirectly involving the frontal lobes. Early symptoms are thought to include irritability, apathy, changes in personality, and impaired judgement.
Q21. Can alcohol or other drugs cause dementia?
A21. Many prescribed medications, over-the-counter medications, and legal and illicit substances can cause cognitive impairment. Prolonged, heavy alcohol use can directly impair brain cell function, but not all experts agree that it can cause permanent cognitive impairment on its own. Part of the difficulty in demonstrating cause is that heavy users of alcohol are also at increased risk of developing cognitive decline due to a nutritional deficiency and at high risk of sustaining a traumatic brain injury from a fall, being hit in the head, or having an automobile accident.
Long-term heavy marijuana use has been shown to result in cognitive impairment in some people. Sedating drugs such as opiates (including morphine, heroin, and codeine) can suppress breathing and lead to the death of brain cells from lack of oxygen. Sedating benzodiazepine drugs (including Valium, Xanax, and Ativan) can directly cause an inability to form new memories that is often reversible if the drugs are discontinued. High doses of benzodiazepines can suppress breathing and lead to a lack of oxygen that kills brain cells and results in dementia. Volatile organic compounds that are inhaled (including gasoline, spray paint, and solvents) can permanently impair brain cell function and cause cognitive decline, slurred speech, and poor balance.
Many prescribed and over-the-counter medications can impair memory formation and cause cognitive impairment. They include antihistamines such as Benadryl (diphenhydramine), as well as drugs for the following conditions: high blood pressure, heart rhythm disturbances, pain (including opiates and NSAIDs such as ibuprofen and naproxen), bacterial infections (including penicillin and ciprofloxacin), viral infections, depression, psychotic mental illnesses, muscle stiffness and rigidity, respiratory conditions, insomnia, seizures, and Parkinson disease. Steroids can cause thinking impairment. Some cancer chemotherapy drugs may cause cognitive difficulty (referred to as “chemo brain”), but this has not been well established. In addition, interactions among these and other drugs may cause cognitive decline.
Most of these drugs cause delirium, an often reversible disorder that is characterized by cognitive decline and inability to pay attention (see Q70). If the offending drug can be stopped, recovery is common, but if there is another underlying cause of dementia, the decline in cognition will not fully resolve.
Many prescribed and over-the-counter medications impair memory formation and cause cognitive impairment. These medication side effects may resolve if the offending medication is stopped.
Q22. Should we try to arrange a brain autopsy for my mother who is diagnosed with Lewy body dementia?
A22. Brain autopsies may be available for people enrolled in research studies that follow participants over time, but otherwise they are difficult to obtain. Most Alzheimer Disease Research Centers do not need additional autopsy material. Many communities do not have an expert in neuropathology, the subspecialty that would perform such an examination. Most research programs have limited ability to provide the service, and there is a significant cost associated with obtaining an autopsy.
It is true, though, that autopsy is the final and most accurate way to identify the cause or causes of dementia. As a doctor I have found autopsy to be a good way to continue my education. I have incorrectly attributed dementia to the wrong cause and learned from my error. Autopsies often reveal that multiple causes are present in very old individuals.
An autopsy might improve doctors’ ability to make the correct diagnosis in other family members in the future. This may be important for people in subsequent generations, since it could become the basis for recommending a preventive treatment that has to be taken for many years before the disease is likely to start.