
| True or False | |
| There’s nothing you can do to improve the look of wrinkles. | ____ |
| As you age, you don’t sweat as much. | ____ |
| You don’t need sunscreen as you get older. | ____ |
| Everybody loses some hair with age. | ____ |
| (Answers at end of chapter) | |
What do you know about your skin? I bet you didn’t know it is the body’s largest organ! (I’ll let you in on a secret: Medical school professors always ask medical students, “What’s the body’s largest organ?” There’s always a lot of giggling and even some blushing until they hear the answer.) On one level, the role of skin is pretty simple: It helps protect your internal organs from the outside environment. It also allows you to handle many things that are dirty or dangerous—like a baby’s soiled diaper or that scary container in the back of the fridge—without worrying that germs will get into your bloodstream.
There’s a lot more to your skin, though, than just keeping the germs out. For instance, skin helps you maintain your body temperature. It contains your sweat glands, which cool you down in the summer and keep heat in on a chilly winter day. Your skin plays a big part in maintaining fluid balance, too. You might have heard that burn victims need huge amounts of fluid to keep them alive; that’s because their skin has become so damaged that it can’t keep enough water inside their bodies to maintain organ function.
Skin also alerts us to what’s going on in the outside world. You might not have eyes in the back of your head, but I bet you know when someone is standing behind you and literally breathing down your neck. The nerve endings in your skin also warn you when the stove is hot, let you know that your drink needs ice even before you taste it, and tell you when it has just started to rain.
As you age, your skin undergoes a lot of changes. Some of these changes are inevitable, but others are preventable or can at least be delayed for a while. When it comes to age-related skin changes, wrinkles are the first issue that comes to mind for most people. But wrinkles are only one effect of our skin’s aging process; as we approach middle age and beyond, our skin will undergo changes in texture, strength, and resilience. You’re going to see some new spots and bumps. Some of these are more bothersome than dangerous, while others should send you right to the doctor. In other words, some changes are a normal part of aging, and some are not.
Don’t panic. While wrinkles may be inevitable, getting older doesn’t have to be a disaster for your skin. Knowing what to expect can help you take steps to protect your skin and keep it healthy as it ages with you.
Your skin is made up of three layers:
Knowing a little bit about the functions of these layers and what they contain will help you understand the normal changes that come with aging as well as what you can do to keep your skin looking and feeling healthy.
The epidermis is the top layer—the one you see every day. The cells in this layer are renewed constantly, with the whole cycle of renewal taking about a month. That’s right—you basically get a whole new layer of skin every month. Most of the cells in your epidermis are keratinocytes, which are largely dedicated to protecting the more sensitive, deeper layers of skin. These cells create a barrier against the elements, holding in fluids and protecting us against dangerous bacteria and viruses. The epidermis also contains melanocytes, the cells that give your skin its color.
Cross section of the human skin.
The next layer is the dermis. It holds blood vessels that feed the skin and nerves that carry sensations from it. Pressure, pain, and temperature are all recognized here. It also contains your oil glands and hair follicles. The dermis contains an important molecule called hyaluronic acid, which holds on to water to keep skin looking full and even. (We’ll come back to hyaluronic acid in a little while.)
The dermis also contains collagen and elastin, two molecules that are essential to the appearance of your skin.
• Collagen allows skin to withstand physical stress without breaking or tearing. It also makes up most of the skin’s mass. Without collagen, your skin would be a lot thinner and more easily damaged.
• Elastin does what it sounds like: It contributes elasticity to the skin. It lets skin “bounce back” from pressure and from everyday bumps and collisions. Think of elastin as a new crisp, tight rubber band.
Underneath the dermis is the hypodermis. “Hypo” is derived from Greek and usually means “low” or “insufficient.” But in anatomical terms, “hypo” means “below” or “under.” Therefore the hypo-dermis is below the dermis. This layer contains a lot of fat cells to help cushion your skin and protect you from injury. These cells also serve as insulation, to help keep your body warm.
When it comes to wrinkles, everyone’s different. Your genetic background has a big impact on how your skin will age. If your parents and grandparents had wrinkles in their fifties and sixties, chances are you will as well. I know America is all about fairness, but some people are just genetically gifted!
Genes aren’t the only reason you get wrinkles, though. One of the biggest factors for premature aging is the amount of time you’ve spent in the sun over the years. When we were younger, of course, we thought a suntan made us look healthy and sexy. But as we get older, we pay a price for that mistaken belief. Sun-related aging, which doctors call photoaging, is superimposed on top of your natural aging process. So if you spent a lot of time at the beach working on your tan in your younger years, you will develop wrinkles sooner than your friends who stayed in the shade.
You might have noticed that people with naturally dark skin often seem to have fewer wrinkles than those with fair skin. That’s because high levels of pigment protect their skin from sun damage. Naturally dark skin, however, is not the same as dark skin from tanning.
Did you ever wonder why your face seems to be the main place wrinkles appear? It feels like a cruel joke, but there’s a reason your face ages first: Your facial muscles move your skin around a lot, causing folds and creases to appear and disappear. All of that folding and creasing puts stress on your skin, and eventually those temporary creases become permanent (so your mother was right—if you make “that expression,” your face really will freeze that way). Aging and sun damage contribute to the process by decreasing the skin’s ability to rebound. Most other muscles in your body serve to move your bones, like when you bend your knees or pick something up with your hands.
Though we all worry about gaining fat, as we get older, we actually lose fat in the hypodermis. Along with changes to collagen and elastin, this loss of fat contributes to the sagging of skin that used to look smooth and resilient.
In addition to gaining a few wrinkles, the look and feel of your skin changes as you age. Aging skin contains less water and lipids than younger skin. Lipids consist of fats, oils, waxes, and similar substances produced in your body. Without them, your epidermis could not do its job as a barrier to the outside world. As we get older, we have fewer lipids in the outermost layer of our skin, which means we cannot hold on to water as well, and therefore we develop drier skin. Certain lipids in the top layer of the epidermis help prevent unwanted bacteria from multiplying.
Our skin also produces less sebum as we age—the stuff that clogged your pores as a teenager and caused you to break out. At the same time, the renewal of skin cells in your epidermis no longer works as smoothly as it used to. All these factors combine to make skin drier and rougher as you get older.
Have you ever noticed that your or an elderly family member’s skin appears thinner or even translucent? That’s also a normal part of aging, and it’s made more noticeable because the blood vessels beneath the skin’s surface are becoming more visible.
Our skin becomes more delicate as we age. A scrape or bump that would lead to a minor scratch on younger skin can actually cause older skin to tear, almost like a piece of tissue paper. That’s because the epidermis and dermis have become more fragile, and loss of elastin decreases the skin’s ability to bounce back from impact. That once fresh, tight rubber band begins to get a little stretched out over the years.
Have you noticed that you seem to sweat less these days? That’s a skin change, too. As we age, the output from our sweat glands declines; this may be one reason why older adults tend to be at a higher risk of heat stroke in the summer than younger folks. When we don’t sweat as much, our bodies can overheat easily. It’s important for older adults to drink plenty of fluids when they’re exposed to extreme heat to prevent overheating.
My generation didn’t think much about sunscreen when we were kids, and I’m sure we’re paying for it now. I wouldn’t be surprised if today’s children, who get slathered with SPF 50 before setting foot on the beach, have different experiences with their skin as they age. But for those of us who had a suntan every summer for most of our younger lives, sun damage is a big deal.
One of the things that happens when you get a suntan is that ultraviolet (UV) radiation from the sun causes molecules called free radicals to form in your skin. Free radicals interact readily with other molecules in your body, altering their structures. Reactions caused by free radicals damage collagen and elastin, and slow down the production of new collagen. Damage from free radicals is part of normal aging, so there’s no way to avoid it completely. But staying out of the sun and wearing sunscreen when you do go outside will definitely help protect you from the worst effects of UV rays.
The sun produces two types of radiation that you need protection from: ultraviolet A and ultraviolet B rays. They’re abbreviated UVA and UVB, and that’s what you’ll see on your sunscreen label. (There’s actually a UVC as well, but the ozone layer blocks most of it out.) UVB radiation, which is mostly absorbed in the epidermis, is the main cause of sunburns. Exposure to UVB radiation also contributes to aging and can cause skin cancer. UVA light penetrates more easily into the dermis. It also ages your skin. Both UVA and UVB light can cause lasting damage, so look for sunscreens with UVA and UVB protection and a sun protection factor (SPF) of at least 15. Higher SPF numbers provide more protection but not typically much more. I recommend SPF 15 because it protects against about 93 percent of UVB rays; SPF 30 protects against 97 percent. I often see people buying sunscreen with a high SPF like 60, mistakenly thinking that it will protect them enough to stay outside all day. It won’t. SPF 60 is not twice as powerful as SPF 30.
And when the sunscreen bottle says to reapply after 2 hours? Do it. It’s not a marketing ploy to get you to buy more sunscreen. Sunscreen does wear off, especially when you sweat. And some of the ingredients may actually become less effective the longer they’re exposed to sunlight.
I get a lot of questions nowadays about vitamin D and sunscreen. Your body makes vitamin D when your skin is exposed to UVB light. And we need vitamin D for all kinds of things: It helps keep our bones strong, our immune systems working, and our kidneys, liver, and thyroid gland functioning properly. The logical next question is if we’re limiting our exposure to the sun by using sunscreen, should we take vitamin D supplements? The reality is that you probably don’t need more than half an hour of exposure to the midday sun, a couple of times a week, in order for your body to make enough vitamin D.1 You can also get vitamin D from the foods you eat—common grocery items such as milk and cereal are fortified with vitamin D, and fish such as tuna and mackerel are natural sources of the vitamin. If you do choose to take a daily supplement, I usually recommend a dosage of 400 to 600 IU per day. Don’t go much above this; higher doses can be dangerous.
If you’re considering taking a vitamin D supplement, be aware of your local climate: If you live in the northern United States, winter sunlight might not be strong enough to trigger vitamin D production. Dark-skinned individuals may also need some supplementation.
In addition to sun exposure, smoking is another lifestyle choice that can affect your skin. In fact, premature skin aging due to smoking even has a name: it’s called smokers’ wrinkles.2
Why does a smoker’s skin age faster? Because all of that smoke comes into contact with the top layer of the skin, and it causes irritation. Smoking also affects blood circulation, including the blood that feeds skin. And the movements that go along with smoking—pursing lips around that cigarette—can create creases that eventually become wrinkles. The moral of the story is—you guessed it—don’t smoke.

Sun Exposure Map of US—This map represents the number of sunny days per year per area—lighter grays mean more sunshine, darker grays mean less sunshine.
When I was a kid, it seems like I injured some part of my body at least once a week. There was always some bump, bruise, or cut in the process of healing. And every time I got hurt, my skin would heal quickly, without even leaving behind a scar. Sure, big injuries can have a lasting impact even on young skin, but those everyday cuts and scrapes were no big deal. Have you noticed that these days, even small cuts and scrapes seem to take a long time to get better? And when they do, sometimes there’s a patch of discoloration where the injury was?
What’s going on? Remember that the epidermis—the top layer of skin—is constantly growing and renewing itself. That process is part of how the skin makes repairs when you cut yourself—and like many other processes, it slows down as we age. Wounds tend to be slower to close, which can raise the risk of infection. Healing in the dermis becomes less efficient with aging, too. Healing requires special white blood cells to move in, clean the wound, and tell other cells to get to work. Skin cells have to replicate and grow, and new blood vessels have to form. All of these processes slow down as we get older.
For healthy older adults, these changes may not be a big deal. Wounds still heal, even if they do so a little more slowly. But for people who have chronic illnesses, such as problems with circulation in their legs, diabetes, or cancer, impaired or slow healing can become a serious problem. It’s important to be more vigilant with cuts and bruises, especially if they seem to be taking a long time to heal. If you have a deep cut or wound, be sure to apply an antibacterial ointment and change the bandage often. If you notice that it seems to be taking an unusually long time to heal, or seems to be getting worse, see your doctor.
Age spots are darkened patches, like large freckles, that appear on sun-exposed areas of your skin. Age spots tend to fade if you stay out of the sun, but they don’t go away completely. They’re a normal part of aging.
Some people will also notice little bright red spots on their skin. These small red dots are called cherry angiomas, and they’re made up of dilated blood vessels that didn’t form correctly. You might be alarmed when you first notice a cherry angioma, but it’s pretty harmless. Cherry angiomas tend to appear on the trunk of the body, but they can show up anywhere. It’s pretty common for them to appear after age 40, and by the time we reach age 70, three out of four of us will have at least one. These cherry angiomas are similar to the ones that appear in infants—except that they usually disappear in the very young, and they don’t disappear in the very old.

Age Spots—Also called liver spots, these dark colored marks appear on sun-exposed areas and occur due to sun damage over a number of years.
Let’s face it: Next to wrinkles, most people’s biggest concern about the effects of aging is what happens to their hair. That includes hair loss, changes in hair texture and color, and new hair growing where you don’t want it. Why does our hair change so much as we get older?
Your hair loses pigment as you age—which is a fancy way of saying, it turns gray. And it’s not just the hair on your head that turns gray. By age 60, the average person has at least 50 percent gray hair on his or her body, with an even higher percentage of gray on his or her head.
The hair on our heads also tends to thin as we get older. That’s because we have fewer active hair follicles as we age, and the thickness of each strand also decreases. Hair growth slows down, too. You probably noticed that you don’t need to get a haircut as often as you used to once you approached middle age.
Most men are eventually affected by male pattern baldness. Twenty percent of men begin to notice some hair loss as early as puberty. By age 30, about 30 percent of men will note some baldness or become completely bald, and by age 50, nearly 50 percent of men will be bald or have a receding hairline. It’s all normal.
Men can expect balding to start at the front of their hairline, with receding hair on each side making an “M” shape over their forehead. Hair at the crown of the head will start to thin, too. Eventually the balding patches meet, leaving hair just around the sides of the head.
While there’s still no scientific explanation for male pattern baldness, there seems to be a hormonal link—the changes in hormone levels as we age may affect the changes in our hair follicles. But as in the case of wrinkles, genetics plays a role, too. If hair loss runs in your family, you’re more likely to lose your hair. We used to think that only the genes of your maternal grandfather (your mother’s father) mattered when it comes to determining your odds of losing your hair. And those genes do have a big influence. But your father’s genes also play a role—if your dad was bald, chances are you will be, too. Oddly, the genes of your paternal grandfather (your father’s father) don’t seem to have as much of an impact. Okay . . . enough with the genetics lesson!
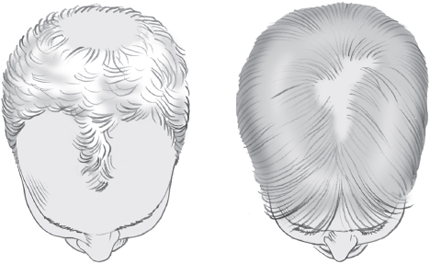
Male/Female Pattern Baldness—Men (left) lose hair along the forehead and on the crown of the head, while women (right) lose hair predominantly on the top of the head.
While it’s not something many women like to talk about, there is such a thing as female pattern baldness, too. Women tend to notice it much later in life than men and typically do not lose any hair until after menopause. Women’s hair usually thins all over, but female pattern baldness can also affect just the top and back of the head. Women may first notice hair loss near the part in their hair. My female patients tell me that this kind of hair loss is deeply embarrassing to them. I know it’s not a lot of consolation, but it’s usually a normal aspect of aging.
You can expect the hair elsewhere on your body to thin out, too, but the remaining strands often become thicker and coarser. Look at older men and you’ll probably notice bushier eyebrows and thicker hairs in the nose and ears. Older women often find themselves battling facial hair that wasn’t there before. It’s okay to tweeze these hairs if you want to, as long as it doesn’t irritate your skin. Remember, older skin doesn’t heal as well when it is irritated.
There are some times, however, when hair loss is not considered a normal part of aging. If your hair loss is sudden (over the course of a couple of months); if it’s associated with pain or severe itching of the scalp; or if you feel very tired, you should see your doctor. Thyroid problems and malnutrition can cause unexpected hair loss.
| Skin Changes: What’s Normal and Not Normal As We Age | |
| Normal | Not Normal |
| Drier, rougher-looking skin | Patches of dry or scaly skin that never seem to heal |
| Nails that are a little yellowish and less translucent than they used to be | Whitish, yellow, or dark spots on nails |
| Gradual hair loss | Sudden hair loss or hair falling out in clumps |
| Itchy skin that improves with moisturizers | Itching all over |
| Age spots | New moles or lumps, or moles that change appearance |
Your nails won’t escape aging, either. You’ll find that your nails grow more slowly over time, and their appearance may change. Young, healthy fingernails and toenails are smooth, strong, and translucent. Older nails can turn dull and become more opaque, and they may take on a yellowish tint. Ridges or furrows may appear on their surfaces. Some people develop a pattern called Neapolitan nails, with a line of white at the bottom, pink in the middle, and an opaque section at the fingertip. It’s all normal.
When our nails turn a dark color, however, it’s usually due to an infection. Whereas most other infections in our bodies are caused by bacteria, infections in our nails are caused by fungus. Fungal infections can affect your nails at any age, but they’re more common as we approach middle age. A typical infection looks like whitish or blackish patches that can eventually cover the whole nail. The good news is that these types of infections rarely spread beyond the nail. The bad news is that they can be difficult to treat. They can sometimes be effectively treated with over-the-counter remedies, but your best bet is to see your doctor. You will usually need a prescription-strength antifungal medication to clear the infection.
Nails that are really thick and hard to cut, painful, brittle, bumpy, or discolored in other ways, or that peel away from the base, are not normal and should also be checked out by a doctor.
As we age, it’s normal to develop some skin problems. The conditions below are ones that I see commonly and am often asked about.
Xerosis is the fancy medical term for very dry, scaly skin. Most adults experience this problem to at least some degree by the time they are 70 years old. It tends to be worse in climates or seasons with low humidity, but it can be a problem any time. When xerosis is particularly severe, skin can actually crack and bleed.
To battle xerosis, it’s essential to keep your skin well hydrated. Look for thick creams that hold moisture in. Over-the-counter products containing urea or lactic acid are sometimes useful. Urea helps hold water in your skin; lactic acid helps smooth away the scaly, dry layer. If the air is dry where you live, a humidifier can also help.
You might hear that you should avoid taking baths or long showers if your skin is dry, but these can actually help. Bathe with a mild soap, using it sparingly. Then seal in the moisture with a hydrating skin cream as soon as you towel off. If home remedies aren’t helping, check in with your doctor. Sometimes a prescription steroid cream can help soothe the skin and give it a chance to heal. Steroid creams, however, cannot be used long term, especially on the face. They can cause your skin to become thinner, and if the steroids are absorbed into your bloodstream, they may cause complications in people with diabetes or glaucoma.
Itchiness is often a direct result of dryness. Treat the dryness and the itch will go away. But as you get older, there are lots of other reasons why your skin might itch. Check your list of medications: Believe it or not, some over-the-counter painkillers can cause you to feel itchy. If the itching comes on rapidly and seems to affect you all over, it is not normal and could be a sign of a more serious illness or an allergy.
It’s not uncommon to see a pimple or two even when you thought you’d be long past worrying about acne. Most of the patients who come to me for acne treatment are on the younger side, but medical research tells us that getting older doesn’t necessarily guarantee clear skin. In one study, trained examiners saw at least a few signs of acne in a third of adults between the ages of 45 and 58.3 Another group of researchers asked people about their own impressions. Among the older adults, 7 percent of men and 15 percent of women said they still had acne at age 50 or above.4 There’s not a lot of data on acne in adults beyond middle age, but I wouldn’t worry if an older patient told me they were continuing to see a pimple now and then.
What isn’t so common, as you get older, is to have the kind of prominent acne that you see in some teens and young adults. Based on the research data, I’d expect to see this type of acne in less than 5 percent of women and maybe 1 percent of men past their mid-forties. If you’re still having serious breakouts, or if you just recently started having them, see a doctor. (Actually, serious breakouts at any age would be a reason to seek treatment—we have a lot of ways to tackle acne these days.) If it’s just plain old acne, you can get treatment that’s tailored to older patients and therefore gentler on your skin than what would be prescribed to a teenager. Or you might find out that you actually have a different problem, like rosacea. Sometimes acnelike breakouts can also be caused by a chemical exposure at work or by a drug you’re taking.
When it comes to run-of-the-mill acne, we don’t know why some people still continue to break out into adulthood. Both blackheads and whiteheads develop when there is overproduction of the type of cells that line hair follicles, and a mixture of sebum and dead skin cells forms a plug. There also appears to be a link between acne and androgens: There are people whose cells don’t make androgen receptors, and they don’t produce sebum or develop acne. We know that androgens help regulate sebum production, and one theory is that people who have trouble with acne have sebaceous glands that are especially responsive to androgens. Other possible influences include effects of bacteria and genetics.
Sometimes older adults develop acnelike spots or bumps called senile comedones. (You might also hear these called solar comedones or Favre-Racouchot Syndrome.) They can look like whiteheads or blackheads, and they often show up on skin near the eyes. They’re thought to be related to sun damage, with changes in the dermis allowing hair follicles to fill up with dead skin cells. Senile comedones can be removed easily by a dermatologist, although they do tend to come back over time.
As many as a third of adults, typically between ages 30 and 65, have seborrheic dermatitis. What is it? It’s a common skin condition that causes dandruff, and it can also cause flaky, scaly skin around your eyebrows, alongside your nose, around your groin, and even inside your ear canal—basically any place on the body where the glands that make sebum are especially abundant.
Seborrheic dermatitis may look bad, but it can be treated. Dandruff shampoo usually does the trick for hair. Tar and salicylic acid preparations can help in other places. Seborrheic dermatitis all over the body is not normal, however, and can indicate a more serious disease. If it persists for several weeks despite treatments, see your doctor.
Rosacea isn’t exactly a disease of aging, but it is more common among older adults than younger ones. No one knows exactly what causes it. Rosacea involves reddening of the skin, usually on the face but sometimes involving the neck, scalp, ears, chest, or other areas of the body. It often appears in the form of red bumps that look like acne. Small blood vessels may appear as little red lines just under the surface of the skin. Rosacea can also make your nose look bulbous and bumpy.
Rosacea is nearly three times more common in women than it is in men. People with pale skin seem to be most susceptible, but anyone can develop rosacea. Lots of famous people have had rosacea, including Bill Clinton, Mariah Carey, Cameron Diaz, and William Shatner. Remember what W.C. Fields looked like? That’s the classic case of rosacea.
Rosacea can be treated, so see your doctor if you notice these kinds of changes in your skin. You may be given antibiotic pills or creams, or even acne medications. Some folks may prefer laser therapy, which typically has good results.
If you aren’t already aware of a disease called shingles, odds are you’ll start to hear about it as you grow older or if you care for an elderly parent. Shingles is the common name for what doctors call herpes zoster. That’s not the same herpes virus that’s transmitted via unprotected sexual intercourse. Shingles is caused by varicellazoster virus, the same virus that causes chicken pox. If you’ve ever had the chicken pox—and if you’re reading this book, you probably did because the chicken pox vaccine didn’t exist until fairly recently—you’re at risk of developing shingles. That’s because the virus can linger in your body long, long after those itchy chicken pox blisters have healed. Your immune system keeps it from causing chicken pox again, but it actually can hide out in certain types of nerve cells. As you get older, your immune system can become weaker and may be less able to keep the virus from sneaking back out again.
The second time around, the varicella-zoster virus usually affects just one area or side of the body. Shingles starts with pain, itching, or burning over one section of skin. The initial symptoms usually last a few days, although sometimes they’ll go on for weeks before blisters appear. Over the course of about a week, the blisters crust over and begin to heal. The classic sign is blisters on one side of the back that don’t cross the center. If you see that, it’s probably shingles.

Shingles—A small constellation of painful, itchy, red bumps and blisters that occur in a narrow horizontal strand. This blistering rash only appears on one side of the body and never crosses over the midline.
You can treat the symptoms with over-the-counter pain medicines, anti-itch creams, and home remedies like cool compresses. Prescription antiviral drugs can usually speed recovery, and I recommend them. If the blisters are affecting your eyes, definitely get help immediately because your vision could be damaged.
Some people who develop shingles have lingering pain, a condition called postherpetic neuralgia. It tends to improve with time, but a small percentage will still have pain even a year after the blisters are gone. Treating shingles with antiviral medications can reduce the risk that the pain will linger.
You can lower your risk of getting shingles with a one-time vaccine that’s recommended for adults age 60 and over. I urge my older patients to get this vaccine.
I cannot tell you how many times I’ve been in a grocery store or at a cocktail party when someone pulls me aside and points to some type of lump or bump on their skin and asks, “Is this normal?” Everyone worries about abnormalities they see on their skin, but the dairy aisle is not the best place for dermatological consult. So I’ve compiled a list (below) of some of the most common skin growths that occur as we age. Hopefully, this will help put your fears to rest.
Skin tags are probably the least scary of the growths you might see. Skin tags are small, soft, fleshy growths, usually the same color as the rest of your skin. Sometimes they’re attached by a short stalk. They’re probably caused by the friction of skin rubbing against skin, which is why they’re often found near folds on the neck and in the armpits. They’re hardly ever cancerous, so the main issue is whether they bother you. If a skin tag tends to get irritated or if it just looks ugly, you can have it removed. It’s usually a simple, quick procedure that can be performed right in the doctor’s office. Do not try to cut these off yourself. I repeat: Do not try to cut these off yourself! Skin tags can often bleed, and I’ve had to treat patients who decided they could use scissors or a razor and avoid a trip to the doctor. Bad idea.
Seborrheic keratoses are dark-colored growths that look like they’re “stuck on” the surface of your skin. I’ve even heard some doctors describe them as looking like “brown wax globs” on the skin. This tends to be a hereditary condition, and some people are especially susceptible, with 10 or more seborrheic keratoses scattered across their skin. These growths also tend to appear more often as we get older.
These growths aren’t likely to become cancerous, although occasionally it can be hard to tell the difference between a seborrheic keratosis and a skin cancer; the only way to know for sure is through a biopsy. If these growths bother you, you can have them removed. Ointments and lotions don’t work on these lesions, so don’t waste your money on fancy products.
What many people do not realize is that these keratoses can often indicate another medical condition—the most common is diabetes. Anytime I see seborrheic keratoses on a patient, I always screen for diabetes. Make sure your doctor checks blood sugar if you or a loved one has a bunch of these “brown wax globs.”
Actinic keratoses are more worrisome. These are considered precancerous. They’re confined within the top layer of skin (epidermis) and aren’t dangerous unless they start to grow deeper. Unfortunately, we can’t be sure which ones will grow and become dangerous. Actinic keratoses start out as rough, scaly patches and develop into hard, rough growths. It’s rare to have just one of these growths; typically, you’ll have 10 or more. Even if they don’t bother you, your doctor may advise you to have them removed. There are lots of ways to remove them, including minor surgery, freezing, laser treatment, and special creams that cause the growth to peel off.
Skin cancer is pretty common (it’s the most common form of cancer), and it does occur in middle age and beyond. In fact, most skin cancers are diagnosed in patients over the age of 60. There seems to be a myth that skin cancer only occurs in young people. That’s simply not true. Luckily, most of the skin cancers that occur in middle age and beyond can be treated pretty easily, but they need to be detected early. The most common skin cancers are:
Basal cell carcinoma is a slow-growing skin cancer that won’t usually spread to other parts of the body, but it’s not something to ignore. Left untreated, a basal cell carcinoma can become a large tumor. At that point, removing it becomes more difficult, and it can be disfiguring. The people at the greatest risk have fair skin that doesn’t tan easily, with blond or red hair and light eyes. Sun damage raises your risk as well. Basal cell carcinomas are usually found on the head or neck, often on the nose. They can also turn up in other places, including areas that aren’t usually exposed to sun.
Basal cell carcinomas can take a few different forms. They can be pinkish or whitish bumps, with a pearly appearance and prominent blood vessels. As the tumor grows, a crust forms in the center. Sometimes it will appear to heal, but it’s actually still there and will continue to grow, with cycles of crusting over and healing. Basal cell carcinoma can also look like a dark growth with a pearly border; a flat, waxy-looking area; a smooth, round cyst; or a scaly spot.
Squamous cell carcinoma is less common than basal cell, and it’s also more dangerous. It’s a faster-growing cancer that can spread to other parts of the body, although that usually won’t happen right away. Bigger, deeper tumors are more likely to spread. Again, light skin, blond hair, and blue eyes mean increased risk, but people with dark skin can get this cancer, too. Squamous cell cancers tend to turn up on sun-exposed areas like the scalp, ears, forehead, lower lip, and hands, but they can appear in other places, too. Sometimes they grow in scars or skin ulcers (open sores that extend to the dermis).
Squamous cell carcinoma tends to look like a bump or nodule that is firm to the touch. It can also look like a well-defined scaly patch, or a flat plaque on top of raised, reddened skin. Sometimes people describe it as looking like a sore that won’t heal.
Melanoma is the most dangerous form of skin cancer, responsible for about 80 percent of skin cancer deaths. It’s particularly deadly in the elderly. Finding a melanoma early is important, because this cancer spreads quickly once it starts growing down into the skin. Melanomas often look like an irregularly shaped freckle that seems to spread out horizontally. They’re often found on parts of the body that aren’t regularly exposed to the sun, so it’s not clear to what degree sun exposure affects your risk.
Doctors use an ABCDE rule to help them decide if a spot or lump is suspicious. We typically apply this rule for melanomas, but it should be applied to any skin lump/bump you are concerned about.
• Asymmetry. If you draw a line down the middle, the two sides don’t match. They do not look the same. A normal mole is equal on both sides and is round.
• Border. The edges aren’t smooth; they can be bumpy or notched. Normal lesions are typically smooth to the touch.
• Color. The spot contains multiple shades of brown or black, or it has areas of other colors such as red or blue. A normal mole typically has one color, usually a shade of brown.
• Diameter. The spot or lump is wider than a pencil eraser.
• Elevation. The mole is raised above the surface. Most normal moles tend to be flat.
If you have a spot on your skin that meets any of these criteria, or that seems to be changing shape or is irregularly shaped, make an appointment with your doctor to have it checked out. Another important factor to keep in mind is that sores that don’t heal are always considered to be abnormal. Even though I noted earlier that it takes longer for our skin to heal as we get older, a sore should still be able to heal on its own. If a sore hasn’t healed for a couple of weeks, see your doctor.
1 Stay out of the sun. If you’re going to be outside for long, use a good sunscreen with UVA and UVB protection and don’t forget to reapply. It’s also a good idea to cover up with a broad-brimmed hat, long sleeves, and long pants. (Lightweight fabrics will keep you cooler, but make sure the sun doesn’t shine right through them.)
2 Moisturize. A good moisturizer will combat the dryness that comes with aging, ward off itching, and help keep your skin looking supple and smooth. And men need to moisturize, too! Ideally, you should moisturize twice a day. You might also want to consider using a moisturizer that also contains sunscreen.
3 Get checked for skin cancer. Skin cancer is linked to sun exposure, but it can also turn up on parts of your body that rarely see the sun—and that are hard for you to see, too. Have your doctor check your skin regularly for any changes. And if you see a new mole or anything else unusual, see your doctor.
4 Stay away from smoke. If you smoke, it’s time to quit! If you’re around people who smoke, try to get them to quit. Your lungs will thank you, and so will your skin. Smoking brings on wrinkles and makes you look old before your time.
5 Eat right. There’s no magic food to keep you looking young, but eating a balanced, nutritious diet will help your whole body look, feel, and function at its best—on the inside and the outside.
If you watch late-night television, you know that there’s always a “new” product out there that seems to promise eternal youth. We all know that’s not possible. But there are some credible and legitimate products available that can help prevent and even undo some of the effects of aging.
Most anti-aging skin care products address the visible changes: wrinkles, age spots, and dull or dry skin. If you remember what you learned at the beginning of the chapter about the layers of your skin, you’ll see why the following products can be helpful.
Before you use any kind of anti-aging product or treatment, I recommend making an appointment with a board-certified dermatologist, who can help you make a plan that’s right for your skin. I also recommend caution when it comes to visiting an expert in an “anti-aging” center. I’m sure some of them are good, but my experience is that many sell products and offer recommendations that aren’t based on medical fact.
Many of the anti-aging products contain some form of vitamin A, and they probably work by helping to thicken skin that has thinned with age as well as reducing the loss of collagen. Some of the ingredient names you’ll see are tretinoin, retinol, retinyl acetate, retinyl propionate, retinyl palmitate, or retinaldehyde. Some of these products are available over the counter, but for others you’ll need to get a prescription from your doctor. None of these elixirs will make you look 21 again, but they can make a difference. Fine lines, dark spots, pore size, and skin texture may all improve. You might eventually see changes in deeper wrinkles, too. The vitamin A-based formulas can irritate your skin, so follow the package directions carefully and stop using them if redness or irritation occurs, or if you don’t notice any improvement in your skin.
I advise caution when it comes to cosmeceuticals. They don’t have to meet the same strict standards that prescription drugs or even over-the-counter medicines must meet. This means that often, they haven’t been thoroughly studied. A cosmetics company could test a product on 10 people and claim that “clinical trials have shown” that it works. From a doctor’s perspective, most cosmeceuticals aren’t backed by much proof. Still, some of the ingredients have shown promise and might be worth a try. Here are a few examples.
• Alpha hydroxy acids seem to help improve skin texture and even out skin tone. They work partly by helping to exfoliate the top layer of your skin, removing dead cells to reveal fresher-looking skin. They may also increase the production of collagen.
• Salicylic acid is thought to have effects similar to alpha hydroxy acids but to be less irritating to skin. This is the same ingredient in some adult acne medications.
• Niacinamide is a form of vitamin B3 that’s said to reduce fine lines, even out skin tone, shrink pores, and improve skin texture. Research so far suggests that over several weeks, a niacinamide-based cream might improve the look of age spots and help reduce the appearance of fine wrinkles. There’s also a chance it could shrink pore size by reducing sebum production.
• Kinetin is a plant growth hormone. It seems that using a lotion containing kinetin could improve the texture of skin and decrease fine wrinkles. It might also help restore or maintain your skin’s function as a barrier against outside irritants.
• Vitamin C. Research seems to suggest that vitamin C might actually work to reduce fine lines, possibly by increasing collagen production. It may also help to lighten discolored skin. The problem with using vitamin C in skin creams is that it isn’t very stable and it’s not very well absorbed by your skin. The companies who make these products have been working on better formulas, but right now I’m not sure you’d be getting your money’s worth. Eating foods rich in vitamin C or taking supplements won’t have as much of an effect.
Over-the-counter creams and prescription drugs only go so far. If you are looking for more dramatic effects, you may consider an in-office procedure.
Microdermabrasion uses tiny crystals to essentially sand off the epidermis, reducing wrinkles and evening out color. Lasers and chemical peels can also treat spots and wrinkles by removing a thin layer of skin. These treatments can indeed make you look somewhat younger, but they also carry a risk of scarring and discoloration.
Injections really can plump up skin and smooth out wrinkles, and the effect lasts for at least a few months.
Collagen has been used this way for many years, and it’s sometimes used in combination with newer options. If you choose a collagen injection, you might want to consider the source of the collagen: Depending on the product, it may come from animals, from human cells grown in a lab, or even from human cadavers. It’s also possible to have collagen made from a small piece of your own skin. Results usually last a few months.
There are a number of other injections that reduce wrinkles by plumping up the skin. I mentioned hyaluronic acid earlier in the chapter—remember, it holds water in the skin and helps it maintain elasticity. Depending on the product, you’ll see results for a few months to a year with this type of injection.
Another filler is made from tiny spheres of calcium hydroxylapatite. This is a mineral substance found in bone, although the stuff in the injection is man-made. The idea is that it encourages the skin to make more collagen, which can mean longer-lasting results, although you might need a touch-up after a few months.
Botulinum toxin (“botox”) shots have certainly gotten popular in recent years. Sometimes it seems there isn’t a celebrity left in Hollywood who can move the muscles in his or her forehead! Botulinum toxin is the same thing that causes the symptoms of botulism, a form of food poisoning that temporarily paralyzes you. Used properly, in tiny quantities, it can weaken your facial muscles just enough that creases don’t form in your skin. The idea is that if you don’t make those creases, your skin won’t wrinkle.
Growth hormone is often advertised as an anti-aging miracle drug. It’s true that your growth hormone levels decline as you age, but there’s no proof that adding it back will make your skin look younger. Growth hormone can cause serious side effects, so until there’s a good scientific study to support its use in fighting aging, it’s not something I recommend using for anti-aging purposes.
Arnold is a 67-year-old man whose only medical problem is high cholesterol. He and his wife recently retired, and were planning an RV trip across the country. When Arnold came to see me, he was complaining of cold symptoms and wanted me to prescribe “some antibiotics to make this go away before we hit the road.” I performed a quick exam, and we discussed his symptoms. I let him know that antibiotics wouldn’t help relieve his cold, and offered some suggestions for managing the discomfort. But at the end of the appointment, Arnold’s wife of 45 years, Cheryl, stuck her head into the exam room and asked her husband, “Did you tell him about the spot?”
Arnold looked embarrassed. “Come on, Cheryl, Dr. Whyte doesn’t want to hear about that freckle.”
Actually, I did. A new or changing “freckle” on a man his age could be a cause for concern. The spot his wife was referring to was on Arnold’s back, so I asked him to remove his shirt. While he was undoing the buttons, he continued to apologize, saying, “I don’t know what she’s so worried about, I’ve never even gotten sunburned there.”
Arnold had a number of moles on his back. Cheryl said most of them have been there “forever,” but she pointed out one that she thought was new. It wasn’t very big, not even as big around as a pencil eraser, but it was irregularly shaped and the color was a mix of tan and brown. I wasn’t certain that it was a melanoma, but I didn’t like the look of it.
I referred Arnold to a dermatologist so that he could get a biopsy. “Sure, doc,” Arnold said, starting to put his shirt back on. “We’ll stop along the way. I bet my son out in Tucson knows a good dermatologist.”
Cheryl shook her head. “We’re not waiting that long. Tell him, Dr. Whyte!”
I agreed. Melanoma isn’t something to mess with. It’s important to catch it early, because if you treat it in its earliest stages, the outlook is good. Later on, though, survival rates aren’t so good. Once I explained this to Arnold, he agreed to make an appointment right away.
I also suggested that Arnold have a full screening for skin cancer, which involves a dermatologist carefully looking over your whole body to make sure there aren’t any other suspicious spots. (I could do that exam for Arnold, but I think it’s even better to let the dermatologist have a look.) Arnold agreed to request a full screening when he made his appointment.
A few weeks later, Arnold and Cheryl called me from the road. They kept the appointment with the dermatologist, who biopsied the “freckle” and didn’t find anything else suspicious. The diagnosis? Melanoma. But Arnold was lucky. We caught it early enough that, after surgery to remove the tumor, he didn’t need additional treatment. He’ll need regular checkups, and he’ll have to keep a careful watch for any other suspicious skin changes. Luckily, he has Cheryl to help keep an eye on him.
Here’s an area where today’s treatments really can fight the signs of aging. Think about how much progress we’ve made over the past 20 years when it comes to hair loss. When’s the last time you saw someone wearing a toupee? Probably more than a decade ago.
That’s because today we have more and better options. Minoxidil, which can be used by both men and women, is a medication you apply directly to your scalp, and it’s available over the counter. It isn’t always effective for everyone, but when it does work, it can actually stimulate new hair growth and stop hair loss from worsening. You’ll get the best results if you start using it when you first notice that your hair is thinning. Despite what you might see on some commercials, you’re not likely to see a full head of hair come back if you already have large bald patches. Minoxidil is a long-term commitment—if you stop using it, you’ll go right back to losing your hair again.
Finasteride is another option, although it’s available only for men. This prescription pill reduces levels of a form of testosterone that seems to trigger hair loss. Most men can use it without any problems, but side effects can include a decreased libido and erectile dysfunction. It can also affect blood tests used for prostate cancer screening. So be sure to let your doctor know you’re taking it, if he or she doesn’t already know. As with minoxidil, the effects of finasteride won’t last if you stop taking it. It can also take a while to see good results—sometimes up to 2 years.
Sometimes my patients ask me if it’s possible to “overdo it” with hair loss drugs. You’re supposed to apply minoxidil twice a day, but will it work faster if you put some on at lunchtime, too? Would three or four times a day be even better?
Like many things in life, more isn’t always better! I don’t recommend using minoxidil more often than directed. One reason is because minoxidil is also used, in pill form, to lower blood pressure. If enough of it is absorbed through your skin, you could end up feeling dizzy and even putting a strain on your heart. Gaining some more hair isn’t worth being dizzy all the time! If you are using minoxidil as prescribed and it isn’t working for you after a few months, talk with your doctor.
Laser treatments are another popular option, though it’s hard to say yet how well they work, or if there are any long-term safety concerns. There just aren’t enough studies yet.
You can also look into hair replacement surgery. Basically, a hair transplant involves moving hair from the back of your head to the front, a few strands at a time. You can also have more dramatic surgery that moves a whole flap of skin around to the front of your head. “Scalp reduction” surgery removes a piece of skin from the bald spot and pulls the back and sides of your scalp closer together. If you are interested in surgery, be sure to choose your surgeon carefully. Like any surgical procedure, there are risks. These can include infections, bleeding, pain, bad reactions to anesthetics, and poor results. There have been instances of death as well even with what seems like simple surgical procedures. Also, hair replacement surgery can often be expensive. Since insurance often does not pay for procedures considered to be cosmetic.
I can’t honestly tell you if or when plastic surgery might be “right” for you as a way to combat aging. Personally, I’m not fond of the idea of having myself cut open just to look younger. Complications are rare, but they can happen, and I’m not always sure it’s worth the risk. But some people do feel these procedures are worth it, and I’ve seen patients, friends, and colleagues who are really satisfied with the results.
I would actively recommend that a patient see a plastic surgeon for age-related changes in a few cases. For example, some people find that drooping eyelids start to impede their vision, and plastic surgery can help with that. Patients who have had significant weight loss also can benefit by having excess skin removed. Of course, if a patient is really interested in surgery to mask the signs of aging, I’ll recommend that they talk with a good surgeon about what can be done.
Answers to true/false statements: False, True, False, True