One of the strengths of MRI is the significant amount of intrinsic contrast between tissues. This contrast is based upon differences in signal intensity between adjacent pixels representing the tissues in the image. It is a result primarily of differences in the T1 and/or T2 relaxation times of the tissues under observation accentuated by the chosen TR and TE. In spite of this inherent contrast, it may be challenging to distinguish pathologic from normal tissue. The pathologic tissue may have similar T1 or T2 times compared to normal tissue. In addition, the voxel may contain significant amounts of normal tissue, which will make the image pixel values similar to those from normal tissue. One approach to increase the signal difference between normal and pathologic tissue is to administer a contrast agent.
Contrast agents for MRI have several advantages over those used for computed tomography (CT). CT agents are direct agents in that they contain an atom (iodine, barium) that attenuates or scatters the incident X-ray beam differently from the surrounding tissue. This scattering permits direct visualization of the agent itself, regardless of its location. Most MRI contrast agents are indirect agents in that they are never visualized directly in the image, but affect the relaxation times of the water protons in the nearby tissue, meaning that one molecule of contrast agent may affect the signal of many nearby spins. The concentration and dosage for MRI agents are therefore significantly lower than for CT agents, which in part explains the lower occurrence of adverse reactions to MRI agents. They are normally excreted through the renal or biliary systems within 24 hours, though the excretion half-time varies substantially from agent to agent. Contrast agents are usually categorized as T1 or T2 agents based on their primary effect of shortening the T1 or T2 relaxation times, respectively. However, these agents also shorten the other relaxation times to a lesser degree. The amount of reduction depends on the concentration of the agent: when concentrated, T1 agents shorten T2 or T2* times and, when dilute, T2 agents reduce T1 times. Contrast agents may also be grouped into intravenous and oral agents, depending on the route of administration. The following is a brief discussion of MR contrast agents with emphasis on those in current clinical use. Safety issues related to the use of contrast agents are described in Chapter 16.
15.1 Intravenous agents
15.1.1 T1 relaxation agents
Virtually all intravenous contrast agents currently in clinical use are T1 relaxation agents and are gadolinium-based agents. Gadolinium, a rare earth metal, has a large magnetic moment, but is toxic as a free metallic ion. Gadolinium agents are designed as chelate complexes, which bind to the gadolinium ion and keep it water-soluble, thereby reducing its toxicity. The primary mode of operation for T1 contrast agents is as a relaxation sink for the water protons.
As mentioned in Chapter 3, T1 relaxation depends upon the “lattice” receiving the energy that the protons have absorbed from the RF excitation pulse. This energy transfer occurs most efficiently when the protons are in the innermost layer of atoms surrounding the metal ion, known as the coordination sphere. Because the chelate molecules are relatively large and have many bonds to the metal ion, there is limited free space in the inner coordination sphere, which prevents the protons on large molecules such as fat from getting sufficiently close to the metal ion for efficient energy transfer. The tissue water is able to diffuse into the inner coordination sphere of the metal ion and give up its energy, then exchange with the bulk tissue water, enabling additional water molecules to enter the coordination sphere. This diffusion/exchange happens very rapidly (∼106 times per second) so that the bulk tissue water is relaxed when the subsequent excitation pulse is applied (Figure 15.1). The result is that the tissue water near the contrast agent has a larger net magnetization than water in the neighboring tissue and will contribute more signal in a T1-weighted image (Figure 15.2). In addition, the rapid exchange process enables many water molecules to be affected by a single chelate complex, which allows low concentrations of contrast agent to be used in clinical studies.
Figure 15.1 Exchange of water molecules in coordination sphere of gadolinium – chelate contrast agent. The chelate molecule causes steric hindrance (crowding) around the gadolinium atom, restricting its access. An excited water molecule is small enough to reach the inner sphere and transfer its energy to the gadolinium ion, then leaves the complex unexcited as another molecule replaces it.
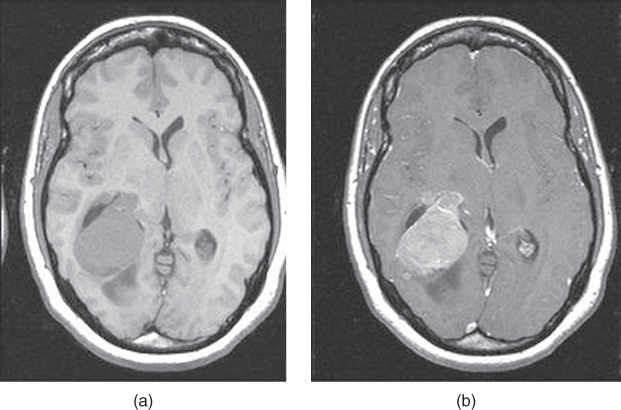
Figure 15.2T1-weighted spin echo images before and after administration of gadolinium–chelate contrast agent: (a) no contrast agent present; (b) contrast agent present. Signal increase due to presence of agent.
Gadolinium-based contrast agents (GBCAs) are categorized both by the molecular shape of the chelate and by the ionicity of the chelate complex (Figure 15.3). The molecular shape may be linear (the less stable architecture) or macrocyclic, and the ionicity may be nonionic (neutral, less stable) or ionic. Table 15.1 lists the agents that are currently available for clinical use. Many of the agents are nonspecific extracellular agents, in that the agents diffuse rapidly from the vascular space into the interstitial space of the tissue (see Figure 12.4). In the brain, they remain within an intact blood–brain barrier. A relatively small dose is typically administered through intravenous injection. The major elimination pathway of these agents is through glomerular filtration and renal excretion. The half-life is typically in the order of 90 minutes with virtually complete elimination of these agents within 24 hours.
Figure 15.3 MRA of renal arteries following half - dose of gadolinium – chelate contrast agent: (a) acquired image from three - dimensional volume acquisition; (b) MIP projection.
Table 15.1 Thermodynamic and kinetic stability measurements of gadolinium chelates (from Port et al., 2008). (Abbreviations: Kcond = conditional stability constant at physiological pH; Ktherm = thermodynamic stability constant; T1/2 = half-life.)
Gadolinium chelate
Type of structure
Thermodynamic stability
Kinetic stability at pH 1.0 at 25°C
(at pH 7.4)
DOTAREM® (gadoterate meglumine)
Macrocyclic ionic
25.6
19.3
338 h
GADAVIST® (gadobutrol)
Macrocyclic nonionic
21.8
14.7
43 h
PROHANCE® (gadoteridol)
Macrocyclic nonionic
23.8
17.1
3.9 h
MULTIHANCE® (gadobenate dimeglumine)
Linear ionic
22.6
18.4
MAGNEVIST® (gadopentate dimeglumine)
Linear ionic
22.1
17.7
OMNISCANTM (gadodiamide)
Linear nonionic
16.9
14.9
OPTIMARKTM (gadoversetamide)
Linear nonionic
16.6
15.0
Other formulations of gadolinium-chelated contrast agents have both hydrophilic and hydrophobic properties. Two examples of these use benzoxypropionic tetraacetate (BOPTA) and ethoxybenzyl diethylenetriaminepentaacetate (EOB-DTPA) as the ligand. The presence of a hydrophobic ligand enables hepatocyte uptake of these agents and elimination by the biliary system, rather than strictly through renal excretion. Approximately 5% of Gd-BOPTA is eliminated by the hepatobiliary system and 95% by renal excretion, whereas 50% of Gd-EOB-DTPA is eliminated by the hepatobiliary system and 50% by renal excretion. The dual pathways of elimination for these agents enable postcontrast imaging emphasizing both tissue perfusion (immediately following administration) and hepatocellular uptake and bile duct elimination (subsequent times). The combined effect of their ease of use and dual-phase behavior have been of significant benefit as liver contrast agents.
The following description of adverse events incorporates information derived from the 2013 Manual on Contrast Media of the American College of Radiology (ACR) (ACR, 2013) and the 2014 Guidelines of the European Society of Urogenital Radiology (ESUR) (Thomsen, 2014).
The frequency of all acute adverse events after an injection of 0.1 or of gadolinium chelate ranges from 0.07% to 2.4%. This frequency is about 8 times higher in patients with a previous reaction to gadolinium-based contrast media. Second reactions can be more severe than the first. Persons with asthma and various other allergies, including allergies to other medications or foods, are also at greater risk, with reports of adverse reaction rates as high as 3.7%. Although there is no cross-reactivity, patients who have had previous allergic-like reactions to iodinated contrast media are also in this category.
Adverse reactions to IV contrast agents can usually be defined as acute, late, and very late events. Acute adverse events occur within 1 hour of contrast medium injection and may manifest as mild, moderate, and severe, with the great majority of reactions being mild. These reactions can be divided into two categories: allergy-like/hypersensitivity and chemotoxic (Table 15.2).
Table 15.2 Acute adverse reactions after contrast media injection (from ACR, 2013)
Allergy-like/hypersensitivity
Chemotoxic
Mild
Mild urticarial Mild itching Erythema
Nausea/mild vomiting Warmth/chills Anxiety Vasovagal reaction which resolves spontaneously
Late adverse events occur 1 h to 1 week after injection and usually manifest as skin reactions similar in type to other drug-induced eruptions (maculopapular rashes, erythema, swelling, and pruritus are most common). This type of reaction has not been described after GBCAs.
Very late adverse events usually occur more than 1 week after contrast medium injection and generally reflect deposition of unchelated gadolinium into the extravascular tissues. Unchelated gadolinium is virtually always bound to biologic anions, with phosphates and hydroxyapatites being among the most common biological anions. The most severe recognized form of deposition is termed nephrogenic systemic fibrosis (NSF), which is causally related to the combination of severe acute/chronic renal failure and gadolinium administration. The great majority of NSF cases have occurred in patients in stage 5 chronic renal failure. The classification of chronic renal failure is presented in Table 15.3. The vast majority of cases of NSF are related to the administration of Omniscan, Optimark, or Magnevist, with occurrences of NSF having a frequency of in 1 million doses in all of the other contrast agents in the setting of their solitary use. Gadolinium is an analog to calcium, and bone deposition in humans has been documented, with a much greater extent of deposition reported to occur with Omniscan compared to Prohance. Currently the long-term consequences from bone deposition have not yet been described. Since children are in a state of much more active bone development it is strongly recommended to only use the most stable gadolinium chelates in pediatric populations. Most recently, a high signal has been described in the basal ganglia of individuals who have undergone multiple repeat MR examinations.
Table 15.3 Chronic kidney disease (CKD) classification based upon the glomerular filtration rate (GFR) (from CKD Work Group, 2013)
GFR stages
GFR
Terms
G1
>90
Normal or high
G2
Mildly decreased
G3a
Mildly to moderately decreased
G3b
Moderately to severely decreased
G4
Severely decreased
G5
<15
Kidney failure
15.1.2 T2 relaxation agents
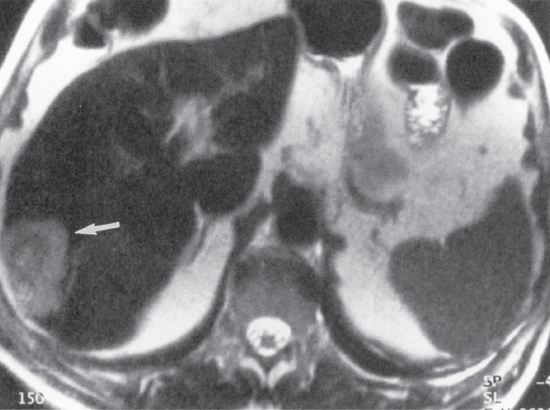
The other class of intravenous contrast agents are T2 relaxation agents. They are typically macromolecules containing several iron atoms that collectively form a superparamagnetic center. The large magnetic susceptibility of the macromolecule distorts the local magnetic field in the vicinity of the agent, causing the nearby water protons to dephase more rapidly than the surrounding tissue. This condition results in significant signal loss in T2-weighted spin echo or gradient echo images. The most common T2 contrast agents are based on superparamagnetic iron oxide (SPIO) particulate molecules, also known as ferumoxides. These agents are selectively absorbed by the reticulo-endothelial cells located in the liver, spleen, and bone marrow. Normal tissue in these organ systems take up the agent and have a low signal on T2- or T2*-weighted images. Lesions that do not contain reticulo-endothelial cells in appreciable numbers do not take up the agent and remain unaffected and therefore have a relatively high signal (Figure 15.4).
Figure 15.4T2-weighted single-shot echo train spin echo image of liver following administration of superparamagnetic iron oxide contrast agent. The T2 relaxation times of the normal tissue are reduced by the iron oxide, while the metastatic lesion shows less agent uptake.
Currently, the only T2 contrast agent licensed for clinical use in the United States is Feridex (magnetite-dextran; Bayer HealthCare AG, Leverkusen, Germany), though its sale was discontinued in the US due to limited sales. It is usually administered as a slow drip infusion over 30 minutes. A further delay of 30 minutes prior to imaging allows for maximal uptake of the agent by reticulo-endothelial cells. Contrast enhancement can be observed from 30 minutes to 4 hours following infusion. Feridex has a good safety profile, but has a potential side effect of acute back pain developing during infusion, occurring in less than 3% of patients. This side effect is usually self-limiting and disappears when the infusion is stopped or slowed. The most important clinical indication for Feridex is in the determination of the extent of liver metastases in patients under consideration for surgical resection. This agent can also distinguish between hepatic origin tumors that contain reticulo-endothelial cells and tumors that do not. Resovist (magnetite/maghemite-carboxydextran; Bayer HealthCare AG, Leverkusen, Germany) is another formulation of a ferumoxide agent that can be administered in a small dose by bolus injection. The advantage of this agent is ease of administration and the lack of back pain as a side effect. It is an ultra-small particulate iron oxide (USPIO) that also increases T1 contrast in dynamic gradient echo scanning immediately following administration, enabling one agent to affect both T1- and T2-weighted scans. Iron-oxide particulate agents are not currently approved for use in liver by the US Food and Drug Administration (FDA).
SPIO agents formulated to a smaller particle size than used for liver imaging are under investigation as contrast agents for the examination of lymph nodes. Normal or hyperplastic lymph nodes take up the agent and lose signal on T2-weighted images, whereas malignant lymph nodes do not take up the agent and therefore appear relatively high signal. Iron oxide particles have also been used to label monoclonal antibodies targeted to specific tissue receptor sites. Asioglycan protein receptor contrast agents are one example that is under development.
15.2 Oral agents
Oral MRI contrast agents are typically nonspecific in nature. They are most often used in abdominal and pelvic studies to provide differentiation of bowel from adjacent structures and to provide better delineation of bowel wall processes. Oral agents may be categorized as positive or negative agents. Positive agents increase the overall signal intensity within the image, generally by shortening the T1 or T2 relaxation times of tissue water. These agents are generally solutions of paramagnetic metal ions or metal–chelate complexes. Many of these agents are present in naturally occurring products (manganese in green tea and blueberry juice) or in over-the-counter medications (ferric ammonium citrate; Geritol; Beecham, Bristol, UK, and Tennessee, US). Other agents have been specifically formulated for use with MRI such as Lumenhance (manganese chloride; Bracco Diagnostic, Princeton, New Jersey, US) and Magnevist Enteral (gadolinium-DTPA; Bayer HealthCare AG, Leverkusen, Germany) as T1 relaxation agents and OMR (ferric ammonium citrate; Oncomembrane, Seattle, Washington, US) as a T2 relaxation agent. Positive agents can provide excellent delineation of the bowel, but the increased signal may induce greater artifacts as a result of respiratory motion or peristalsis.
The other type of oral contrast agent is a negative agent. Negative agents eliminate the tissue signal from the area of interest. Two approaches are used for negative agents. One method reduces the T2 relaxation times using suspensions of ferumoxide particles. The particles may be suspended in aqueous solution (Ferumoxsil; Advanced Magnetics, Cambridge, Massachusetts, US) or adsorbed on to a polymer. The other approach uses an agent that contains no protons and therefore produces no visible MR signal. The most common agent of this type is Perflubron (perfluorooctylbromide (PFOB); Oxygent; Alliance Pharmaceutical, San Diego, California, US). Barium sulfate, clay, and air have also been used for intraluminal studies. One significant problem with many negative contrast agents, particularly iron-based agents and air, is that they increase the local magnetic susceptibility, which may induce significant dephasing artifacts at high field strengths.
For many applications, distention of gastrointestinal segments using water or water-based oral agents may achieve sufficient diagnostic value. For an evaluation of gastric processes, distention with orally administered water may be adequate, while for colorectal processes, endorectal administration of contrast agents is required.
 One of the strengths of MRI is the significant amount of intrinsic contrast between tissues. This contrast is based upon differences in signal intensity between adjacent pixels representing the tissues in the image. It is a result primarily of differences in the T1 and/or T2 relaxation times of the tissues under observation accentuated by the chosen TR and TE. In spite of this inherent contrast, it may be challenging to distinguish pathologic from normal tissue. The pathologic tissue may have similar T1 or T2 times compared to normal tissue. In addition, the voxel may contain significant amounts of normal tissue, which will make the image pixel values similar to those from normal tissue. One approach to increase the signal difference between normal and pathologic tissue is to administer a contrast agent.
One of the strengths of MRI is the significant amount of intrinsic contrast between tissues. This contrast is based upon differences in signal intensity between adjacent pixels representing the tissues in the image. It is a result primarily of differences in the T1 and/or T2 relaxation times of the tissues under observation accentuated by the chosen TR and TE. In spite of this inherent contrast, it may be challenging to distinguish pathologic from normal tissue. The pathologic tissue may have similar T1 or T2 times compared to normal tissue. In addition, the voxel may contain significant amounts of normal tissue, which will make the image pixel values similar to those from normal tissue. One approach to increase the signal difference between normal and pathologic tissue is to administer a contrast agent. than water in the neighboring tissue and will contribute more signal in a T1-weighted image (Figure 15.2). In addition, the rapid exchange process enables many water molecules to be affected by a single chelate complex, which allows low concentrations of contrast agent to be used in clinical studies.
than water in the neighboring tissue and will contribute more signal in a T1-weighted image (Figure 15.2). In addition, the rapid exchange process enables many water molecules to be affected by a single chelate complex, which allows low concentrations of contrast agent to be used in clinical studies.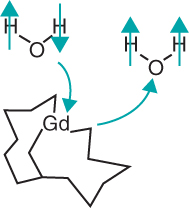
 is typically administered through intravenous injection. The major elimination pathway of these agents is through glomerular filtration and renal excretion. The half-life is typically in the order of 90 minutes with virtually complete elimination of these agents within 24 hours.
is typically administered through intravenous injection. The major elimination pathway of these agents is through glomerular filtration and renal excretion. The half-life is typically in the order of 90 minutes with virtually complete elimination of these agents within 24 hours.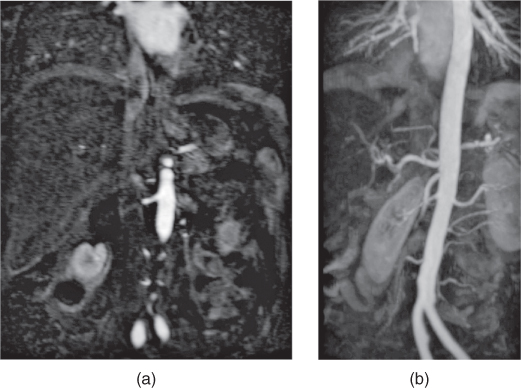
 at pH 1.0 at 25°C
at pH 1.0 at 25°C
 (at pH 7.4)
(at pH 7.4)



 of gadolinium chelate ranges from 0.07% to 2.4%. This frequency is about 8 times higher in patients with a previous reaction to gadolinium-based contrast media. Second reactions can be more severe than the first. Persons with asthma and various other allergies, including allergies to other medications or foods, are also at greater risk, with reports of adverse reaction rates as high as 3.7%. Although there is no cross-reactivity, patients who have had previous allergic-like reactions to iodinated contrast media are also in this category.
of gadolinium chelate ranges from 0.07% to 2.4%. This frequency is about 8 times higher in patients with a previous reaction to gadolinium-based contrast media. Second reactions can be more severe than the first. Persons with asthma and various other allergies, including allergies to other medications or foods, are also at greater risk, with reports of adverse reaction rates as high as 3.7%. Although there is no cross-reactivity, patients who have had previous allergic-like reactions to iodinated contrast media are also in this category. in 1 million doses in all of the other contrast agents in the setting of their solitary use. Gadolinium is an analog to calcium, and bone deposition in humans has been documented, with a much greater extent of deposition reported to occur with Omniscan compared to Prohance. Currently the long-term consequences from bone deposition have not yet been described. Since children are in a state of much more active bone development it is strongly recommended to only use the most stable gadolinium chelates in pediatric populations. Most recently, a high signal has been described in the basal ganglia of individuals who have undergone multiple repeat MR examinations.
in 1 million doses in all of the other contrast agents in the setting of their solitary use. Gadolinium is an analog to calcium, and bone deposition in humans has been documented, with a much greater extent of deposition reported to occur with Omniscan compared to Prohance. Currently the long-term consequences from bone deposition have not yet been described. Since children are in a state of much more active bone development it is strongly recommended to only use the most stable gadolinium chelates in pediatric populations. Most recently, a high signal has been described in the basal ganglia of individuals who have undergone multiple repeat MR examinations.