Shoulder
Standard radiographs
Shoulder injury:
▪ The AP view is standard in all departments.
▪ The precise second view will vary.
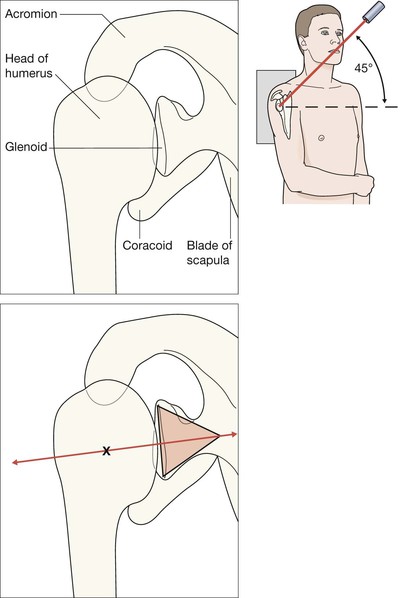
□ We prefer the apical oblique projection (aka Modified Trauma Axial, MTA; see p. 76), because it allows gentle positioning of the patient, provides excellent demonstration of dislocations and shows fractures extremely well1,2.
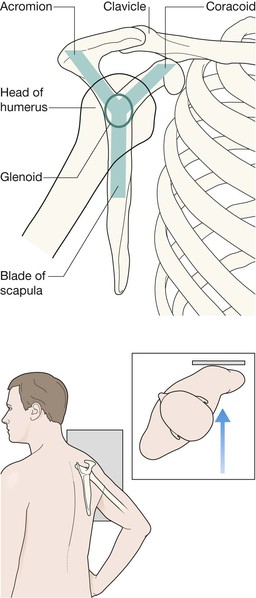
□ Second best: the scapula Y lateral (see p. 77). The patient is comfortable as the arm is not moved, and a true scapula Y lateral will show posterior dislocations3. But this view must be technically very precise, and fractures can be difficult to identify.
□ The axial (armpit) view is not recommended. It will show a posterior dislocation and most fracture fragments, but it requires abduction of the injured arm which can be very painful. It can also cause further damage. Frequently it results in a poor radiograph.
Note our descriptive emphasis in this chapter
We are strong advocates that the second view for an injured shoulder should be the apical oblique radiograph rather than any alternative second view. Consequently, our descriptions concentrate mainly on the AP view and the apical oblique view of the injured shoulder.
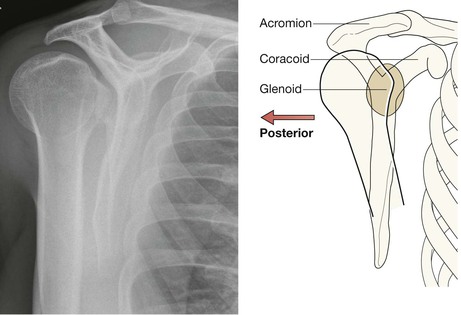
Normal anatomy
AP view
The normal humeral head does not appear round and symmetrical. Its shape mimics the head of an old fashioned walking stick. This is due to the radiographer positioning the humerus in external rotation.
The articular surfaces of the glenoid and the humerus parallel one another.
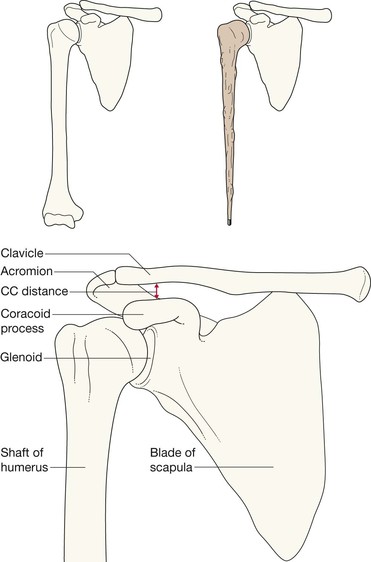
The inferior cortex of the lateral part of the clavicle aligns with the inferior cortex of the acromion process. There is no step between these cortices.
Lateral scapula view—ie the Y view3
The humeral head overlies the centre of the glenoid. The Y is formed by the junction of the scapular blade, the coracoid and the spine of the scapula. On this view anterior is towards the ribs and posterior is away from the ribs.
Analysis: the checklists
The AP radiograph
Ask yourself five questions.
1. Is the humeral head lying directly below the coracoid process?
2. Does the humeral head have a walking stick shape, and does its articular surface parallel the glenoid margin?
No = use the second view to rule out a posterior dislocation.
3. Is the acromioclavicular joint normal—ie do the inferior cortices of the clavicle and acromion process align?
No = subluxation or dislocation at the acromioclavicular joint.
4. Is the coracoclavicular distance more than 1.3 cm?
Yes = stretching or rupture of the coracoclavicular ligaments (see p. 86).
5. Is there a fracture of the head or neck of the humerus, the glenoid margin, the clavicle, the body or neck of the scapula, or a rib fracture?

Apical oblique view1,2
Ask yourself three questions.
1. Do the articular surfaces of humerus and glenoid lie immediately adjacent to each other—ie does the centre of the triangle base line up with the centre of the glenoid articular surface?
No = a glenohumeral joint dislocation or subluxation.
2. Is there a fracture of the head or the neck of the humerus?
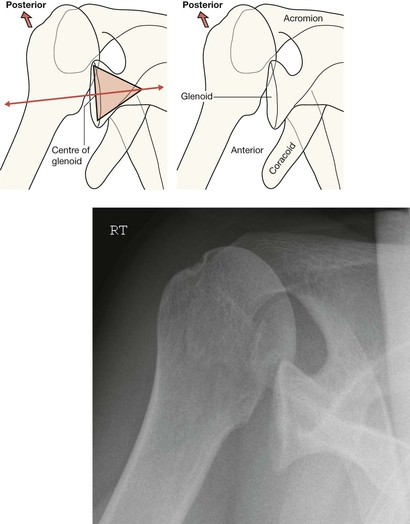
The apical oblique view is excellent in demonstrating a posterior dislocation at the glenohumeral joint.
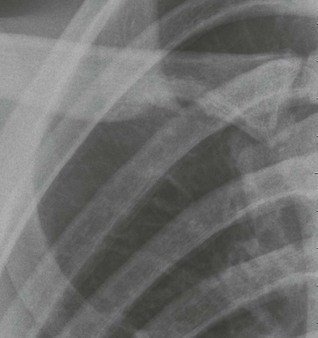
This radiograph shows a posterior dislocation. The two drawings illustrate how an inexperienced observer can readily detect the abnormal alignment on the radiograph.
See p. 76 for the expected normal alignment on an apical oblique view.
The common fractures4–9
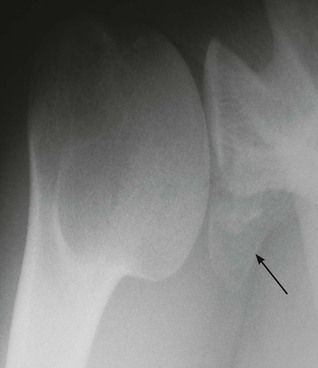
Greater tuberosity of the humerus
Often undisplaced and is then very subtle (arrow). Examine the AP view very carefully.
Occasionally these fractures are invisible on the plain radiographs.

Humeral head and/or rim of the glenoid
A recognised complication of an anterior dislocation.
This apical oblique view shows the abnormal articular surface of the humeral head with a fragment (arrowhead) adjacent to it; a defect in the rim of the glenoid is also present (arrow). The glenohumeral articulation is normal.

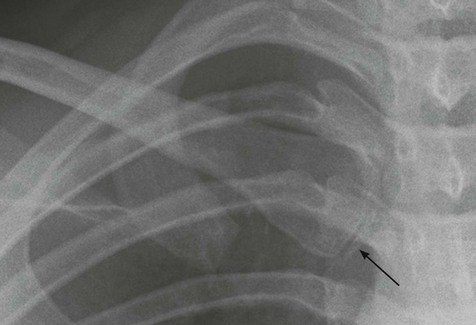
Clavicle
Accounts for 35% of all fractures involving the shoulder region6.
▪ Fractures of the mid third account for 85% of clavicular fractures. Most of these occur in patients less than 20 years old. Lateral third fractures occur less frequently, and mainly in adults.
▪ In young children, a Greenstick fracture may occur (pp. 18–19), and appears as a slight kink in the bone.
▪ Clinical impact guideline: a clavicle fracture in an infant is a recognised complication of traumatic birth delivery; be careful not to misdiagnose this finding as a non-accidental injury.
Fracture of the middlethird of the clavicle.
Most mid third fractures occur as a result of a fall on the shoulder. Some result from a transmitted force (ie a fall on the outstretched hand).

Fracture of the lateral third of the clavicle.
Often due to a direct blow to the clavicle (eg during a contact sport, a fall, or a road traffic accident).
Clinical impact guideline: more likely than a middle third fracture to be associated with delayed union or non union10.

The common dislocations4,8,9
Anterior dislocation of the glenohumeral (GH) joint
GH dislocations are the commonest traumatic dislocations of the skeleton. Anterior dislocations represent 95% of all GH dislocations. The appearances shown here are characteristic and on the whole the diagnosis is straightforward.
Anterior GH dislocations are often accompanied by fractures of the greater tuberosity of the humerus: see p. 80.

Anterior dislocation of GH joint: Apical oblique view.
The head of the humerus is seen well away from the glenoid articular surface and positioned anteriorly.
When you draw in the glenoid cone or triangle (see p. 76), the line passing through the apex of the triangle does not pass through the centre of the head of the humerus.
A bonus from an apical oblique view: exquisite visualisation of bones and articular surfaces.

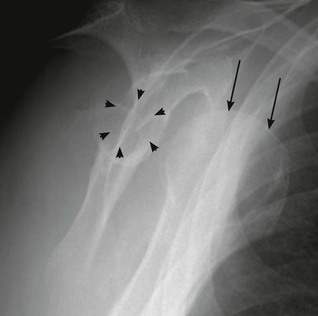
Anterior dislocation of GH joint: Scapula Y view.
The humeral head (arrows) does not cover the glenoid (arrowheads). The glenoid is identified as being at the junction of the three limbs of the “Y” (see p. 77).
A disadvantage of the scapula Y: fractures are often not visible.
Pitfall: Haemorrhage causing subluxation.
Following an injury, usually with an intra-articular fracture, there may be extensive haemorrhage into the joint. The increase in fluid volume may push the head of the humerus inferiorly (as shown), but not medially. This inferior displacement can be misinterpreted as a dislocation.
The haemorrhage will absorb within a week or two and consequently the subluxation will resolve.

Anterior dislocation of the glenohumeral (GH) joint with accompanying fractures
A fracture of the greater tuberosity of the humerus frequently accompanies a dislocation.
▪ Always scrutinise both shoulder views for a fragment detached from the glenoid rim or from the posterior and superior aspect of the head of the humerus. If a fragment enters the joint it may prevent a successful reduction.
▪ Compression injuries also occur: Hill–Sachs deformity and Bankart's lesion (see opposite).
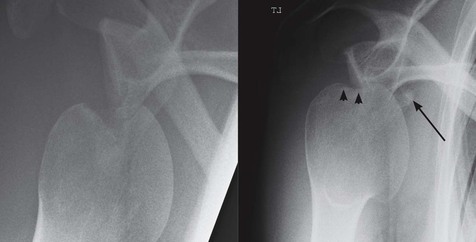
Patient (left) with a fracture of the greater tuberosity and an anterior dislocation on this apical oblique view. Patient (right) with an anterior dislocation and a fragment (arrow) detached from the head of the humerus (arrowheads).
A previous anterior dislocation had caused a fracture of the inferior margin of the glenoid (arrow).
Hill–Sachs deformity.
A compression fracture (arrow) of the posterolateral aspect of the humeral head.
This injury results from impaction of the humeral head against the glenoid margin. It occurs in as many as 50% of anterior dislocations7.

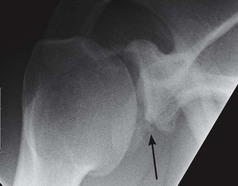
Bankart's lesion.
A fracture of the anterior lip of the glenoid.
It results from impaction by the humeral head on the glenoid during dislocation.
This apical oblique radiograph was taken following a successful reduction. The glenoid fragment is well shown inferiorly (arrow).
Subluxations and dislocations at the acromioclavicular joint (ACJ)
This joint is the sole bone to bone attachment of the upper limb to the rest of the skeleton.
Assess this joint on the AP view only. The other projections may mislead.
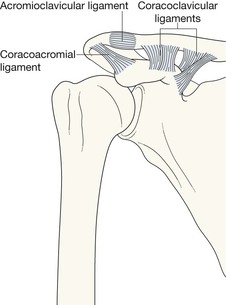
The ligaments
The coracoclavicular (CC) ligaments attach the patient's arm to the body, and prevent vertical movement of the clavicle and ACJ. The normal distance between the coracoid and clavicle on the AP view is usually less than 1.3 cm4,5. Complete dislocation of the ACJ indicates rupture of CC ligaments (see opposite).
Abnormal findings:
▪ The inferior cortices of the clavicle and acromion do not align.
▪ If the CC distance is greater than 1.3 cm then rupture of the CC ligaments is probable.
Stress radiographs will help in equivocal cases of CC ligament rupture. The radiograph should ideally be obtained with the weights hanging from the wrists, in order to ensure full relaxation of the upper limb muscles.

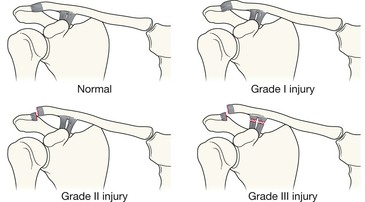
Grading the injuries to the ligaments11.
Grade I: Stretching or partial rupture of ACJ ligament, but intact CC ligaments. Radiological findings: normal, or slight step at ACJ.
Grade II: Rupture of ACJ ligament and stretching of CC ligaments. Radiological findings: a step at the ACJ. May need stress views if equivocal.
Grade III: Rupture of ACJ ligament and rupture of CC ligaments. Radiological findings: a step at the ACJ and increased CC distance (ie greater than 1.3 cm). May need stress views to show the full extent of the damage.

Clinical impact guidelines.
ACJ subluxation (left) is invariably treated conservatively, usually with an excellent outcome. On the other hand, a complete ACJ dislocation (right) is an important injury. Opinion regarding management varies. It will be treated conservatively by some surgeons who then reserve surgery for those who develop persistent symptoms. Other surgeons advise early surgery for nearly all ACJ dislocations, particularly for manual workers and athletes.
Uncommon but important injuries
Posterior dislocation at the glenohumeral (GH) joint
The naming of this injury is arguably inaccurate. It is very rarely a complete dislocation. Despite the notable posterior displacement it is, invariably, a major subluxation.
On many occasions there will be an accompanying fracture of the anterior aspect of the humeral head.
Uncommon. Fewer than 5% of shoulder dislocations. As many as 50% are overlooked even when initial radiographs show the abnormality7.
Often caused by violent muscle contraction; either during a convulsion or from an electric shock. Sometimes, both shoulders will dislocate simultaneously8.
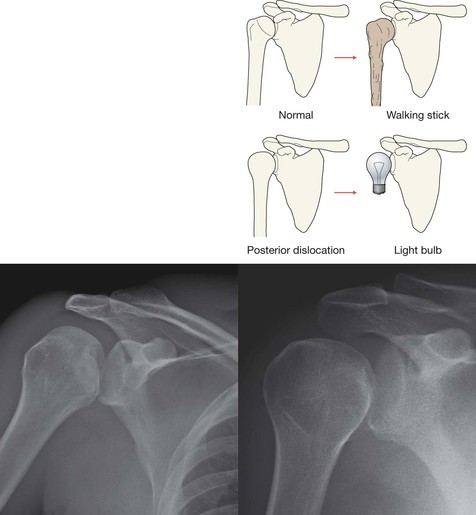
Posterior dislocation: characteristic appearances on the AP view.
The rotated and posteriorly displaced humeral head loses the normal parallelism of the articular surfaces, as in the two posterior dislocations below.
The humeral head frequently appears rounded—no longer the contour of an old fashioned walking stick. The globular contour has been likened to a light bulb or drumstick appearance (right).

Posterior dislocation: characteristic appearances on an apical oblique view.
The main mass of the humeral head lies posterior to the glenoid.
Posterior dislocation: characteristic appearance on a scapula Y view7.
The centre of the humeral head lies posterior to the junction of the three limbs of the Y (ie away from the ribs).
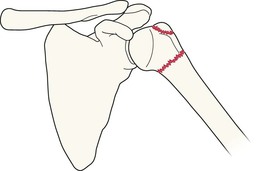
Fractures of the proximal humerus
Neck of humerus
Usually occurs in an osteoporotic elderly patient as a result of a fall. A greater tuberosity fracture may also be present.
In younger patients it is invariably caused by a violent force.
In children and adolescents the growth plate is involved (Salter–Harris fracture, p. 15).
Elderly patient. Impacted fracture of the neck of the humerus.
A large joint effusion (haemorrhage) has caused the head of the humerus to sublux inferiorly.

Fractures of the body or neck of the scapula
Usually result from a high impact event. Serious soft tissue or neurovascular injuries are recognised associations8.
You will only see what you look for…these fractures are easy to overlook. Always check the AP and the second view very carefully.
Road traffic accident. Transverse fracture through the body of the scapula (arrows).

Inferior dislocation of the humeral head (luxatio erecta)
Very rare and accounts for less than 0.5% of all shoulder dislocations. The clinical finding is classical—a Statue of Liberty appearance with the arm elevated and the forearm fixed and resting on the head5,12. The AP radiograph shows the head of the humerus nestling immediately inferior to the glenoid with the humerus pointing upwards. Usual cause: forceful hyperabduction of an abducted limb.
Pitfalls
Positioning
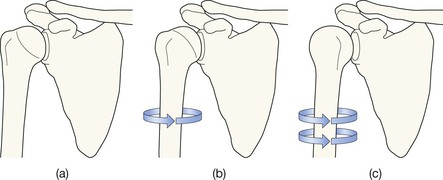
The effect of internal rotation on the contour of the humeral head. Standard AP radiographs are always obtained with the humerus positioned in slight external rotation and this accounts for the humeral head looking like a club-headed walking stick as shown in (a). However, the injured joint may be so painful that the patient holds the arm in internal rotation. When this occurs then a light bulb appearance (b,c) may result and can mimic a posterior dislocation. An error in interpretation will be avoided by checking the precise position of the humerus on the second view.
Developmental variants that can mislead

On the AP view in the immature skeleton, the growth plate for the humeral head lies obliquely, appearing as two separate lines. Either of these normal lines (arrows) may be mistaken for an undisplaced fracture.

The tips of the acromion and coracoid processes ossify from separate ossification centres. In children these secondary centres may be mistaken for fracture fragments.
Occasionally the secondary centre at the tip of the acromion does not fuse with the rest of the scapula, and remains as a separate bone—the os acromiale. It may be mistaken for a fracture. Interestingly, when present, this accessory ossicle is usually bilateral.
The medial clavicular epiphysis is one of the last of all the secondary centres to unite to the parent bone (at approximately 25 years of age). Do not confuse this epiphysis (arrow) with a fracture.
The rhomboid fossa.
A common normal variant. This notch or prominent depression in the inferior aspect of the medial portion of the clavicle is the point of insertion of the costoclavicular ligament attaching the clavicle to the costal cartilage of the first rib.
Do not mistake it for a pathological erosion of the clavicle.