Ankle & hindfoot
Normal anatomy
Lateral view—bones and joints
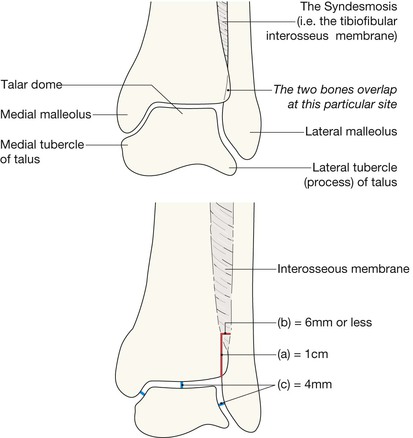
The lateral and medial malleoli can be identified. Helpful hints to aid identification:
The posterior lip (or tubercle) of the tibia, conventionally and inaccurately referred to as the posterior malleolus, is well shown.
The calcaneum and its sustentaculum tali are demonstrated. Bohler's angle can be assessed for normality.
The base of the 5th metatarsal is often included.



AP mortice
The mortice projection is obtained with slight (20°) internal rotation so that the fibula does not overlap the talus.
The joint space should be of uniform width all the way around. This space is well seen medially, it continues over the superior aspect of the dome of the talus, on to the lateral side of the joint.
The width of the joint space measures approximately 4 mm2.
The surface of the talar dome should be smooth, smooth, smooth. No irregularity, no notching, no defect.
The lateral process (also known as the lateral tubercle) of the talus is an important structure. The talocalcaneal ligament attaches to this part of the bone.
A useful rule: the bones of the tibia and fibula should always overlap on the mortice view. Any clear separation between these two bones should lead you to question whether the interosseous membrane is torn.

Analysis: the checklists1,3,4
AP mortice
Check the:
▪ Malleoli—fracture or … fractures?
▪ Tibiofibular interosseous membrane—any suggestion of a rupture?
□ If normal, the tibia and fibula should show some degree of overlap.
□ A measurement: the width of the space between the distal tibia and fibula at a point 1.0 cm proximal to the tibial articular surface should not exceed 6 mm5.
□ Medial and lateral processes (ie the tubercles, p. 268)—any fragmentation?
▪ Joint width—does any part exceed the normal 4 mm3?
▪ Epiphyses and growth plates in children—normal? (see pp. 15 and 280).

Normal features and measurements (ie rules of thumb) relating to:
(1) the interosseous membrane, and (2) the various articulations at the mortice joint.
Normal AP mortice view.
All of the checkpoints are normal.
Note that part of the fibula overlaps part of the tibia. This is a characteristically normal appearance on a mortice view.

Normal AP mortice view. A child.
The growth plates and all of the other checkpoints are normal.

Lateral view
Check the:

Measuring Bohler's angle.
Draw a line from the highest point anteriorly to the highest midpoint. Then draw a line from the highest point posteriorly to the highest midpoint. The angle subtended should be 30° or more.



Common fractures/torn ligaments
The malleoli3,6
▪ Most ankle fractures involve one or both malleoli. These fractures are often easy to diagnose because you will know precisely which bones are tender.
▪ The direction of the applied forces will determine the particular fracture (or fractures) and any associated ligamentous damage:



Transverse fracture of the medial malleolus; oblique and transverse fractures of the distal fibula and lateral malleolus; lateral subluxation of talus.

Multiple fractures affect the tibia and fibula. Note the wide separation at the tibiofibular joint indicating rupture of the interosseous membrane.

Small fragments (arrow) are detached from the lateral process of the talus.
This indicates ligamentous damage.

We have taken illustrative license with the earlier cases in this section by only providing AP radiographs. In all instances it is essential to assess both the AP and lateral radiographs as a pair. In this patient the AP view shows the transverse fracture of the lateral malleolus and the lateral subluxation of the talus. The lateral view shows the full extent of the fibular fracture and its displacement. It also allows assessment of the posterior lip of the tibia, the talus and the calcaneum.
Base of the 5th metatarsal
An avulsion fracture. This common injury results from avulsion of the metatarsal tuberosity at the insertion of the peroneus brevis tendon. The fracture occurs as a consequence of forced inversion.

Fracture of the base of the 5th metatarsal.
A twisted ankle (ie if a forced inversion injury) will often result in a transverse fracture of the base of the 5th metatarsal. The radiograph shows a typical appearance.

The calcaneum
The calcaneum is the most commonly injured bone of the hindfoot. Types of calcaneal fracture are shown on pp. 278–279. See also infrequent calcaneal injuries on p. 288.
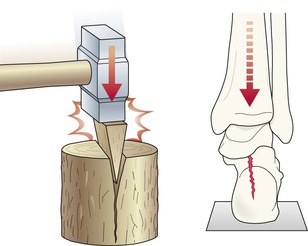
Most severe injuries occur following a fall from a height.
The fracture partly results from the talus driving into the calcaneum, like a wedge of steel slamming down into a block of wood.

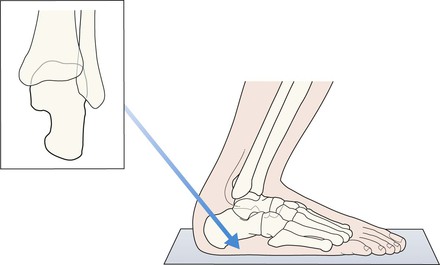
If a calcaneal fracture is suspected then an axial view should be obtained.
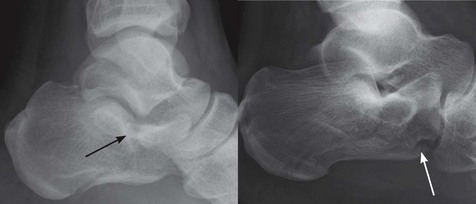
The fractures (arrows) through the body of the calcaneum are well shown.

Some fractures, particularly those involving the anterior process of the calcaneum (arrow), can result from a simple twisting injury.
Several types of calcaneal fracture
Intra-articular (75%)
Intra-articular fractures (arrows) involve the subtalar joint (left) or calcaneo-cuboid joint (right).

Some fractures will only become apparent when Bohler's angle is assessed on the lateral view (above).
This angle is normally 30–40°. If the fracture results in flattening of the bone then the angle will be considerably less than 30° (above right).
Flattening of Bohler's angle is the dominant feature in the calcaneal fracture shown in the radiograph on the right.
Extra-articular (25%)
Usually more difficult to detect compared with intra-articular fractures.
Extra-articular fractures involve the posterior part of the calcaneum or, alternatively, the anterior process of the bone1,4,8. Most of these fractures are sustained following a fall on the heel, but not from a great height. Occasionally a twisting injury may be the cause.


A sclerotic line or density in the body of the calcaneum (arrow) may be the only evidence of an impacted fracture. This is an extra-articular fracture through the tuberosity of the calcaneum and was sustained during a relatively minor fall on to the heel.
Growth plate (Salter–Harris) fractures
▪ Relatively common in children. A distal growth plate injury of the tibia is second in frequency to an injury of the distal growth plate of the radius.
▪ Growth plate fractures are described in detail on pp. 14–17.
▪ The most common growth plate fractures (types 1–4) are shown below.
The Salter–Harris classification/description of the fractures that involve the growth plate.


Salter–Harris type 2 fracture of the tibia.
A type 2 fracture is the most commonly occurring of the fractures that involve the growth plate.
Ligamentous injuries
Torn medial or lateral ligaments
If there is widening of one side of the mortice joint space then there is commonly an associated fracture elsewhere. Suspect widening if the joint space is wider than 4 mm medially or laterally3. Caution: the radiographs may appear normal even when there is severe ligamentous damage. Sometimes stress views will be required.

Fracture of the fibula.
The widened medial joint space indicates an associated ligamentous tear/rupture (the deltoid ligament).
Tear of the interosseous membrane
This injury is very easy to overlook1,5,9,10. The AP radiograph will often provide evidence of a tear/rupture. Look for widening of the space between the distal tibia and the fibula. A useful rule of thumb: suspect a tear of the tough tibiofibular syndesmosis whenever the distal tibia and fibula do not overlap slightly on the AP mortice view.
Also … apply the 6 mm rule (see p. 270).

The wide separation between the tibia and the fibula indicates a major tear of the interosseous membrane (the syndesmosis).
This membrane is a fairly rigid structure. It holds the shafts of the tibia and fibula together, and extends downwards from the superior to the inferior tibiofibular joint.
Infrequent but important injuries
Fractures of the talus
Talar fractures are rare. Many result from a high energy injury, often a road traffic accident or a fall from a height.

Neck of the talus4,11
An important injury because of the high risk of subsequent avascular necrosis (AVN) and secondary degenerative arthritis. AVN is caused by disruption of the blood supply to the body of the talus. Displacement of the fracture increases the probability of AVN. A displaced fracture is easy to detect. An undisplaced fracture is easy to overlook.


Talar dome–osteochondral fracture
A small but clinically important impaction fracture, usually consequent on an inversion injury1,12. The term osteochondritis dissecans was used in early descriptions of this lesion when it was assumed that the pathology was a spontaneous necrosis of bone in the dome of the talus. It is now generally accepted that most of these lesions are actually osteochondral fractures resulting from trauma.
In many cases the talar lesion is not an acute injury but has resulted from an earlier shearing or compression force.

An osteochondral fracture is identified as either a focal defect (ie a lucent area) or an irregularity of the cortex. Most frequently situated on the medial or lateral aspect of the talar dome. Sometimes a small fragment will be detached from the dome and lie free within the joint.
Maisonneuve fracture
The ankle joint is in effect a bone ring and this particular ring extends as high as the knee because of the strong tibiofibular interosseous membrane. On occasion an external rotation injury of the ankle may cause an ankle injury but in addition the forces/energy acting within the interosseous membrane (the tibiofibular syndesmosis) may extend to the upper leg and cause a fracture of the proximal fibula13. The high fibular fracture may be overlooked because the main symptoms are around the ankle joint.
This combination injury is known as a Maisonneuve fracture. Suspect this injury whenever clinical examination of the upper leg is painful.

Maisonneuve fracture. Subluxation of the talus and evidence of rupture of the interosseous membrane.
The upper leg was painful and an additional radiograph revealed the high fracture of the shaft of the fibula.
Distal tibial fractures involving the articular surface
These fractures are rare, accounting for less than 1% of fractures of the lower limb14.
The usual cause: a high energy fall or RTA producing a compression fracture, often with comminution. Compression fractures of the tibia are rare because it is usually the calcaneum that received and accepts the major vertical force and is fractured.

Both patients had fallen from a height. Comminuted fracture of the tibia with involvement of the articular surface (arrows).
Complex Salter–Harris fractures
These two fractures are rare but need to be recognised early, as accurate reduction is essential in order to ensure normal growth and to avoid subsequent ankle deformity.
Triplane fracture3,15,16
This Salter–Harris type 4 fracture is a complex multi-directional fracture of the tibial epiphysis. It is a three plane fracture. As follows:
▪ Sagittal plane: vertical fracture through the epiphysis.
▪ Horizontal plane: transverse fracture through the growth plate.
Always suspect this complex fracture whenever the AP view shows a vertical fracture through the tibial epiphysis. Suspicion necessitates CT for full evaluation.
Pitfall: the full extent of the injury is often not evident on plain radiography.

Triplane fracture.
The fracture lines are indicated by the arrows.
The subsequent CT (right) shows the fracture in exquisite detail.
Tillaux fracture3,16
This Salter–Harris type 3 fracture is an avulsion fracture through the tibial epiphysis. The fracture involves a partially closed epiphysis (age 11–15 years). It occurs in adolescents in whom the medial part of the growth plate has fused, but the normal fusion has not yet reached the lateral aspect. It is a two plane fracture. As follows:
▪ Vertical plane: through the epiphysis.
▪ Horizontal plane: through the lateral part of the growth plate.
Pitfall. This fracture can sometimes be confused with a Triplane fracture on plain radiography. CT will distinguish.

Tillaux fracture.
This Salter–Harris type 3 fracture limited to the lateral aspect of the epiphysis and growth plate is well shown on the lateral and AP radiographs (arrows).


Os trigonum fracture17

The os trigonum is an elongation/enlargement of the posterior process of the talus. It is present in approximately 50% of feet and can be fused to the posterior aspect of the talus or it can be a free bone on its own. A fracture of a fused os trigonum can occur during a twisting injury at the ankle joint. A very high index of clinical suspicion is essential in order to raise the suggestion of a fracture. The two examples shown here are normal.
Talar dislocations—Infrequent but important
The subtalar joint has two parts and either part can dislocate as a result of a high energy force.

Dislocation of the talocalcaneal joint.
The talonavicular and talocalcaneal articulations are not anatomical—compare this with the normal articulations on the opposite page.
Several fractures/fracture fragments are also present.

Dislocation of the talonavicular joint.
Note that the head of the talus overlaps, ie it is displaced anterior to, the articular surface of the navicular bone (arrowheads).
The normal appearance at the talonavicular joint is shown in the other figures on the page opposite.
Pitfalls
Calcaneum: the apophysis

The normal calcaneal apophysis can appear very irregular, fragmented and/or sclerotic, as in these two examples.
Calcaneum: the anterior process
A fracture of the anterior process (p. 279) is a common injury. However, the anterior process can develop from a secondary ossification centre. If this centre does not unite with the parent bone it (the os secundum) can be mistaken for a fracture. Distinguishing between a fracture and an os secundum will depend on correlation with the clinical findings.

Normal accessory ossicles
Small bones lying adjacent to the tips of the medial and lateral malleoli are very common. They may be misread as avulsed fracture fragments. Occasionally an ossicle will be difficult to distinguish from a fracture and clinical correlation is important. Fractures are tender, accessory ossicles are not. Also:
▪ An accessory ossicle has a well defined (ie corticated) outline.
▪ An acute fracture fragment is ill defined (ie not corticated) on one of its sides.
Normal accessory ossicles at tips of the medial and lateral malleoli in a 10 year old.
A frequent finding.


The os trigonum (arrows). A common normal variant (p. 288). It may be attached to, or separate from the talus.