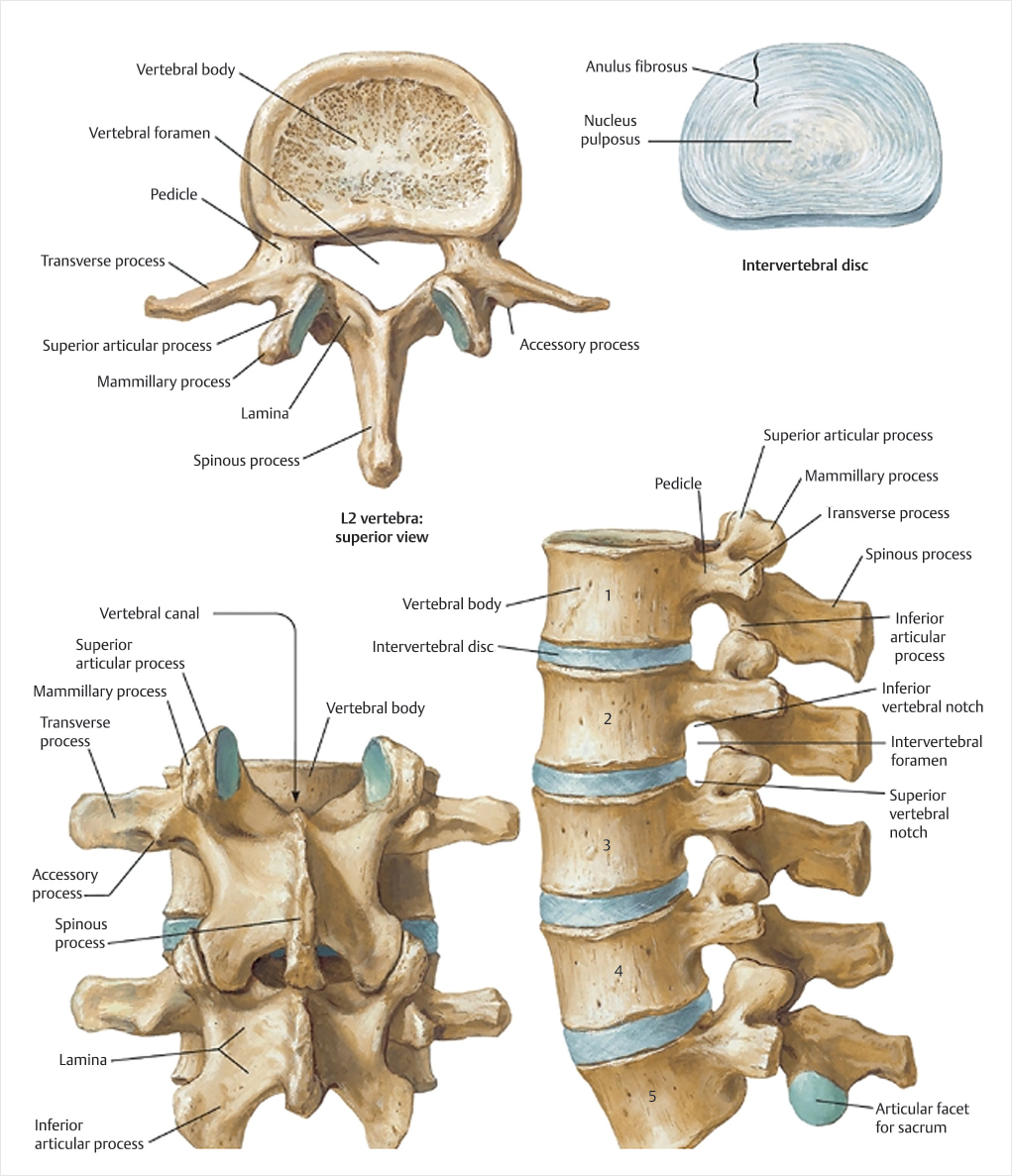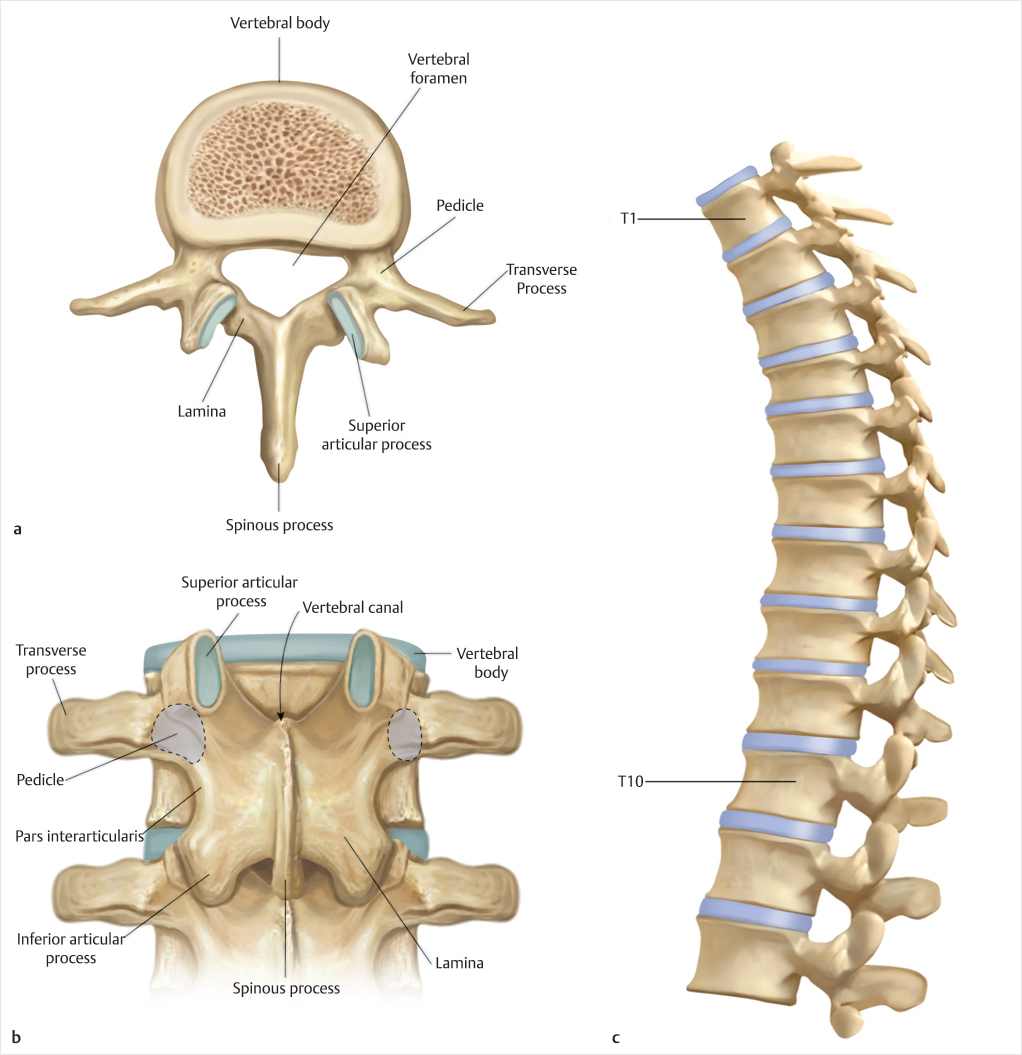
Fig. 2.1 (a–c) Anatomy of the thoracic spine. (Source: An H, Singh K, ed. Surgical anatomy. In: Synopsis of Spine Surgery. 3rd ed. New York, NY: Thieme; 2016.)
Summary
Vertebral compression fractures (VCFs) result from either trauma or pathologic weakening of the bone by conditions such as osteoporosis or malignancy. They often cause severe pain, physical limitation, and disability, and lead to increased morbidity and mortality with considerable heath care expenditures. Fracture classification systems have been designed to identify spinal instability and guide treatment. The public health and economic impact is considerable. Regardless of etiology, timely and accurate diagnosis will assist in determining the appropriate treatment.
Keywords: vertebral compression fracture, vertebral fracture classification system, vertebral augmentation, osteoporosis, bone mineral density, trauma, multiple myeloma, malignancy, kyphoplasty
Vertebral compression fractures (VCF) result from either trauma or pathologic weakening of the bone by conditions such as osteoporosis or malignancy. They often cause severe pain, physical limitation, and disability, and lead to increased morbidity and mortality.1–6 Vertebral fractures, whether they are symptomatic or asymptomatic, are associated with increased morbidity and mortality, and patients with osteoporotic vertebral fragility fractures have an increased risk of mortality compared to age-matched controls.7–9 Annual health care expenditures to diagnose and treat vertebral fractures are considerable and are on the rise.10
The thoracolumbar region is the most common location for fractures of the vertebral column.11–13 The thoracic spine is functionally rigid due to coronally oriented facet joints, thin intervertebral disks, and stabilization offered by the rib cage, so significant trauma is required for fracture or dislocation unless the vertebrae are pathologically weakened by disease (▶Fig. 2.1). The presence of the spinal cord in this region predisposes the patient to neurological injury if the canal is compromised causing significant impingement on indwelling the neural tissue. The lumbar spine, on the other hand, is relatively flexible due to the thicker intervertebral disks, sagittally orientated facet joints, and absence of the rib cage (▶Fig. 2.2). The relatively lesser incidence of neurological injury in lumbar fractures can be attributed to the large size of the neural canal and the greater resilience of the cauda equina nerve roots. The thoracolumbar junction (T10–L2) is uniquely positioned between the rigid thoracic spine and the mobile lumbar spine. This transition from the less mobile thoracic spine with its associated ribs and sternum to the more dynamic lumbar spine subjects the region to significant biomechanical stress.12,13 Among thoracolumbar injuries, 50 to 60% affect the transitional zone (T11–L2), 25 to 40% affect the thoracic spine, and 10 to 14% involve the lower lumbar spine and sacrum.14
Vertebral fractures may have a profound and untoward effect on quality of life. The presentation of patients with VCFs varies depending on etiology, severity, and the level or levels affected. Discrete onset axial back pain after lifting or bending is often reported and may or may not be associated with sciatica. Pain is typically positional, worsened by weight-bearing activities, transition from one position to another, and by lying supine. Patients without significant trauma rarely have neurologic deficits, but elderly osteoporotic patients, in particular, have marked functional impairment with activity reduced by postural changes and pain. Multiple thoracic fractures can result in severe kyphosis, which may lead to restrictive lung disease.15 Lumbar fractures may alter abdominal anatomy, leading to constipation, abdominal pain and distention, reduced appetite, premature satiety, and urinary incontinence.16 These restrictions increase the risk of losing independence, social isolation, and clinical depression.
Osteoporosis is the most common condition associated with VCFs and affects approximately 700,000 individuals each year in the United States and 30 to 50% of people older than 50 years worldwide.17–20 Osteoporosis or “porous bone” is a systemic bone disorder resulting from an imbalance between bone formation and bone loss and is characterized by diminished bone strength. Bone strength is dependent on both the quality of the bone and the bone mineral density (BMD). Bone quality refers to architecture, mineralization, accumulation of damage (microfractures), and turnover. Bone density is determined by peak bone mass, which is usually attained by age 30 and subsequent bone loss.21
Osteoporosis can occur in both sexes, but is more common in women following menopause.21 Both men and women have age-related decline in BMD in middle age due to increased bone resorption as compared to bone formation. This is especially common in women as they experience more rapid bone loss in the early years after menopause.21 Peak bone mass is achieved only after linear bone growth has ceased. Therefore, bone mass attained early in life may be the most important determinant of skeletal strength later in life.21,22 Factors that affect achievement of peak bone mass include lifetime calcium and vitamin D intake, physical activity, smoking, alcohol, eating disorders, and endocrine disorders.22 Characteristics associated with low bone mass later in life include female sex, increased age, estrogen deficiency, white race, low body mass index (BMI), and a family history of fractures.21
As a complication of osteoporosis, VCFs are associated with significant morbidity and mortality and are an increasing public health risk as the population continues to age (▶Fig. 2.3). Vertebral fracture incidence increases substantially with age in both males and females. The annual incidence of vertebral fractures increases from 0.9% among middle-aged women in their 50s to 60s to an incidence of 1.7% among those 80 years and older.10,17,23 The mere presence of a vertebral fracture is associated with increased risk of future fractures. If the patient presents with one VCF, the risk of having another one within the first year is increased by fivefold.17 If the patient has two fractures, the risk increases to 12-fold and if three or more fractures are present, the risk is 75 times increased for having another vertebral fracture.
Fig. 2.1 (a–c) Anatomy of the thoracic spine. (Source: An H, Singh K, ed. Surgical anatomy. In: Synopsis of Spine Surgery. 3rd ed. New York, NY: Thieme; 2016.)
BMD as measured in gram per square centimeter (g/cm2) and its related T-score are used to screen for the objective presence of osteoporosis. The T-score is the number of standard deviations above or below the mean BMD for a healthy 30-year-old reference patient. The U.S. standard is to use data for a 30-year-old of the same sex and ethnicity, but the World Health Organization (WHO) recommends using data for a 30-year-old white female for everyone. Values for 30-year-olds are used in postmenopausal women and men older than 50 years because they better predict risk of future fracture. The criteria of the WHO are as follows: Normal is a T-score of -1.0 or higher. Osteopenia is defined as between -1.0 and -2.5. Osteoporosis is defined as -2.5 or lower, meaning a bone density that is 2.5 standard deviations below the mean of the reference.24
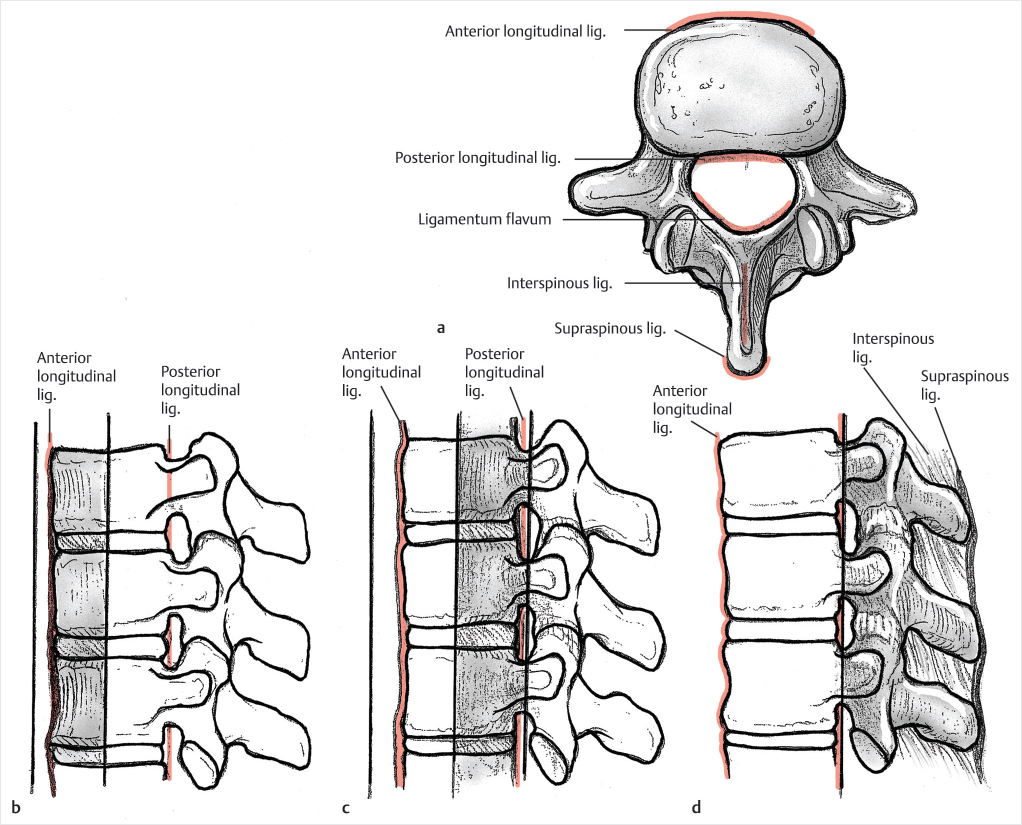
Fig. 2.2 Anatomy of the lumbar spine. (Source: Kim D, Choi G, Lee S, ed. Anatomy of the intervertebral foramen. In: Endoscopic Spine Procedures. 1st Edition. New York, NY: Thieme; 2011.)
It should be noted that while bone density scanning and determination of the patient’s BMD and T-score are valuable from a screening and treatment monitoring perspective, it does not determine which vertebral fractures are osteoporotic VCFs as a greater proportion of vertebral fragility fractures occurs in patients with either a normal bone density or with osteopenia as compared to patients whose T-score shows osteoporosis. The clinical scenario and amount of force required to produce that VCF is a far better determination of whether the patient’s fracture is traumatic or the result of osteoporosis than their T-score.
Using data from the National Health and Nutrition Examination Survey (NHANES), an estimated 16% of U.S. men and almost 30% of U.S. women aged 50 and over have osteoporosis as defined by their bone BMD.25 An estimated 50% of women and 20% of men in the United States will sustain an osteoporotic fracture at some point in their lifetime.16 The prevalence of vertebral fracture is similar in men and women and increases with age from less than 5% in those younger than 60 years of age to 11% in those age 70 to 79 years to 18% in those aged 80 years or older.26 The age-correlated prevalence rates in the United States are very similar to those in Europe, as published by the European Vertebral Osteoporosis Study.18,27–31
Fig. 2.3 Vertebral compression fracture is illustrated by the black arrows and shown in the sagittal plane (a), coronal plane (b), and axial plane (c). (These images are provided courtesy of Dr. M. R. Chambers.)
More than 2 million osteoporotic fractures including 700,000 VCFs were diagnosed in 2005 and that number of osteoporotic fractures is projected to increase to over 3 million fractures by 2025, an increase of 52%.32 Importantly, this calculation may be an underestimate as it has been projected that less than one-third of all vertebral fractures are clinically diagnosed (see Chapter 34: Treatment of Osteoporosis after Vertebral Augmentation).33
The spine is the most frequent site of bone metastasis.34 In patients with cancer, the risk for pathologic VCF results from bone involvement, with fracture incidence estimated to be 24, 14, 6, and 8% among patients with multiple myeloma (MM) and cancers of the breast, prostate, and lung, respectively.35,36 These fractures are most often of the compression or burst type and may result in axial or radicular pain, and sometimes neurologic and/or motor/sensory deficits. The incidence of symptomatic metastatic spinal tumors in the United States is estimated to be approximately 160,000 per year37 and between 6 and 24% of these patients are predicted to have a VCF at some point over the course of their disease.35 Unfortunately, pathologic fractures of the spine are often the initial manifestation of a metastatic malignancy (▶Fig. 2.4).
Although often perceived as a rare disease, MM is in fact the second most commonly diagnosed hematologic malignancy in the Western world.38 MM comprises 1.6% of all bone malignancies in the United States and occurs primarily in the elderly, with a median age at diagnosis of 69 years.39 The 5-year survival rate is less than 50%.40 VCFs are the most common type of fractures in patients with MM, occurring at the onset of the disease in 34 to 64% of patients.41,42
Fig. 2.4 Sagittal short tau inversion recovery (STIR) MR image with a region of decreased signal present within the posteroinferior portion of the L2 vertebral body consistent with a blastic metastasis (white arrow). Decreased height and normal marrow signal is noted in the L1 vertebral body (white arrowheads) consistent with a chronic osteoporotic vertebral compression fracture vertebral body. (This image is provided courtesy of Dr. M. R. Chambers.)
Unlike osteoporosis, which causes weakening of trabecular bone structure and lower bone mass, the mechanisms of MM leading to significant structural weakness are varied and remain incompletely understood. There is increased osteoclast precursor differentiation and, consequently, enhanced bone resorption.43 Early diagnosis and treatment are critical in slowing the disease progression and the corresponding deterioration of the patient’s quality of life.44
Most MM patients report back pain at the time of initial diagnosis.45 Up to 80% of patients with MM are diagnosed during routine imaging.46 Radiological findings include diffuse bone loss, focal osteolytic bone lesions, bone marrow edema, and fragility fractures of the axial skeleton.47 Bone marrow edema is a common MR imaging finding of acute VCFs but may be difficult to see due to bone marrow signal abnormalities seen in patients with MM.48 Diffuse bone loss alone is often misdiagnosed as osteoporosis until more symptoms associated with MM develop.49 When focal osteolytic lesions or significant diffuse bone loss is evident, risk for vertebral fractures is high.50
The patient’s osteoporosis status could be an indicator of disease progression to MM.51 Twenty percent of osteoporotic patients presenting with vertebral fractures may have either monoclonal gammopathy of undetermined significance or MM.50 Almost 80% of MM patients are diagnosed with osteoporosis and the level of BMD has a major impact on survival.52,53 However, there are several problems with the use of BMD as a diagnostic tool of MM. First, the decline in BMD as a result of aging and/or osteoporosis is well understood; it declines 0.1 to 0.2% per year due to aging while after menopause and onset of osteoporosis, it peaks to 1 to 2% and then slows back to the decline seen in normal aging.47 The decline in BMD in MM-induced osteoporosis is less well understood and unpredictable. In a recent study, Borggrefe et al found that BMD of fracture cases in MM patients were significantly reduced in men, but not in women.54 Second, as has been mentioned previously, BMD and T-score as determined by dual X-ray absorptiometry (DXA) has been challenged as a limited tool for the diagnosis of osteoporosis itself as it only partially estimates fracture risk. The use of DXA as a diagnostic evaluation tool in MM is even less valid.55 Also, routine assessment of BMD in MM patients is not recommended due to methodological difficulties in these patients and the frequent use of bisphosphonates in all symptomatic MM patients.56 Finally, there are no established and well-defined clinical criteria to differentiate osteoporotic VCFs and MM-induced osteoporotic VCFs, but MR imaging can be helpful in patients who are suspected to have MM (▶Fig. 2.5).57
The annual incidence of traumatic spinal injuries is greater than 160,000 in North America.58 According to Hu et al, the incidence of traumatic spinal injuries was 64/100,000 population/y in Canada alone.59 Of the injuries to the thoracolumbar region, around 50 to 60% affect the transitional zone (T11–T12), with another 25 to 40% affecting the thoracic spine, and the remainder affecting the lower lumbar spine and sacrum.14 The peak incidence of thoracolumbar fractures is observed in patients who are between 20 and 40 years of age with these injuries being more common in men.14,60 Thoracolumbar fractures are associated with neurologic injury in 20 to 36% of cases61,62 and the type of fracture affects both the chances for and the extent of a neurological deficit. In a multicenter study, the incidence of neurological deficit ranged from 22 to 51% depending on the fracture type (AO Classification type A: 22%; type B: 28%; type C: 51%; ▶Table 2.1).11,63
Fig. 2.5 Multiple myeloma. Mid-sagittal T2-weighted MR images of the lumbar spine show multiple, well-circumscribed, high-signal-intensity lesions throughout the lumbar spine (white arrows) consistent with plasma cell infiltration of the lumbar spine bone marrow. (Source: Khanna A, ed. Extradural tumors. In: MRI Essentials for the Spine Specialist. 1st ed. New York, NY: Thieme; 2014.)
Most thoracolumbar fractures are associated with trauma and 65% occur due to motor vehicle injuries or falls from a height, with a lesser portion of these fractures attributed to sports injuries or violence. Due to the high-velocity nature of these traumatic fractures, they are commonly associated with other injuries such as hemopneumothorax, rib fractures, vessel injuries, and diaphragmatic rupture.64,65 Seatbelt (Chance) fractures and flexion–distraction injuries are other traumatic spinal fractures that are often associated with intra-abdominal visceral injuries. First described in 1948 by G.Q. Chance, the Chance fracture is a purely bony injury extending from posterior to anterior through the spinous process, pedicles, and vertebral body (VB), respectively. Seen most often in the upper lumbar spine in adults, it typically results from excessive flexion, as caused by a lap belt (without shoulder belt support) injury during a motor vehicle accident. Incidence has been reduced dramatically by the required use of shoulder belts in motor vehicles.
History and physical examination help guide the choice of the initial imaging modality. Many times, advanced and/or dynamic imaging will be needed to detect spinal instability. A careful history regarding vertebral fracture injury mechanism, pain, and the presence or absence of neurological symptoms is essential. The patient may report pain associated with movement and/or with prolonged positions and give-way weakness or a feeling of “instability.” Axial, nonradiating back pain of stabbing or aching quality is the most common symptom. Patients with neurological injury may complain of weakness, paresthesia, or anesthesia below the injury level and may have urinary retention. Thorough inspection of the spine should be performed after a careful log roll maneuver to look for abrasions, tenderness, local kyphosis, and a palpable gap in between spinous processes. Neurological assessment should follow the standard American Spinal Injury Association (ASIA) guidelines (▶Fig. 2.6).66
Table 2.1 AO classification system
Type A: Compression injuries |
Failure of anterior structures under compression; posterior soft tissue is intact even with posterior element fractures |
A1: Wedge fracture—fracture of a single end plate without involvement of the posterior wall • A1.1: End plate impaction – Up to 5 degrees of end plate impaction – Posterior wall is intact |
• A1.2: Wedge impaction – Greater than 5 degrees of end plate impaction – Posterior wall is intact |
• A1.3: Biconcave (VB collapse) – Symmetric loss of VB height – Posterior wall is intact |
A2: Split fracture—fracture of both end plates without involvement of the posterior wall • A2.1: Sagittal – Extremely rare in the thoracolumbar spine – Posterior wall is intact |
• A2.2: Coronal – Posterior wall is intact |
• A2.3: Multiple (pincer) – Central VB is crushed and filled with disk material – Posterior wall is intact |
A3: Burst fracture—fracture with any involvement of the posterior wall; only a single end plate is fractured • A3.1: Incomplete – Upper or lower half is burst – Posterior wall is NOT intact – Fracture fragments are retropulsed into the spinal canal to some degree – Posterior ligamentous complex remains intact |
• A3.2: Burst split – One half of the VB is burst – The other half is has split sagittally – Posterior wall is NOT intact – Fracture fragments are retropulsed into the spinal canal to some degree |
• A3.3 (and A4): complete—fracture with involvement of the posterior wall and both end plates – More frequently associated with neurologic injury – Posterior wall is NOT intact – Fracture fragments are retropulsed into the spinal canal to some degree |
Type B: Distraction |
Failure of the posterior or anterior tension band. |
B1: Posterior soft tissues (subluxation with transosseous tension band disruption [chance fracture]) |
B2: Posterior tension band disruption together with a type A fracture (classified separately) |
B3: Anterior disk (extension spondylolysis)B3: Anterior disk (extension spondylolysis) |
Type C: Multidirectional with translation |
Failure of all elements leading to dislocation or displacement |
C1: Anterior posterior (dislocation) |
C2: Lateral (lateral shear) |
C3: Rotational (rotational burst) |
As the spinal cord normally ends between the L1 and L2 level and the cauda equina fills the distal canal, varied neurological injury patterns can be observed with thoracolumbar fractures. Neurological injuries at or above L1 can injure the spinal cord and injuries below L2 typically affect only the nerve roots of the cauda equina. Conus medullaris syndrome, characterized by exclusive damage to sacral innervations to the bowel and bladder with intact lumbar nerve roots, is a unique feature of T12–L1 injuries.
Numerous classification systems have been proposed to describe thoracolumbar spinal fractures resulting from osteoporosis, neoplasia, or acute trauma. Each system was designed to improve upon the last as a reliable way to identify spinal instability and, ultimately, to guide treatment.
In 1938, Watson-Jones first described the concept of spinal instability and developed a system that integrated the posterior ligamentous complex to described seven fracture types in three major patterns: simple wedge fractures, comminuted fractures, and fracture-dislocations.67
Over a decade later in 1949, Nicoll improved the classification system by formally defining the anatomy that was responsible for spinal stability, including the VB, the disks, the intervertebral joints, and the interspinous ligament.68 He emphasized the importance of the interspinous ligament as a crucial component of stability.
Holdsworth was the first to describe stability in terms of two columns.69,70 In his two-column theory, compressing the anterior column causes distraction of the posterior column and vice versa. Holdsworth expanded on Nicoll’s assumption that the interspinous ligament was paramount in determining stability. He described a posterior ligamentous complex (the posterior column) and believed that the entire posterior column was crucial for stability. Therefore, loss of integrity to this posterior ligamentous complex would define instability. Holdsworth also described mechanisms of spinal injuries and defined six groups: anterior wedge-compression fractures, dislocations, rotational fracture-dislocations, extension injuries, burst fractures, and shearing fractures. This classification system predates the modern imaging modalities and is now rarely used.
Panjabi71 and White et al72 described three conceptually separate but interdependent components responsible for stability: (1) a passive subsystem consisting of the vertebrae, facets, intervertebral disks, spinal ligaments, and joint capsules; (2) an active subsystem of spinal muscles and tendons; and (3) a control subsystem for neural feedback, including the neural control centers and force transducers located in ligaments, tendons, and muscles.
Introduced in 1982, the Allen and Ferguson system, also rarely used, was a “mechanistic” system that classified spinal injuries based on three common mechanical modes of failure of the spine: compression–flexion, distraction–flexion, and compression–extension.73
Also introduced in 1982, the Denis three-column spinal stability classification system describes fracture types and included possible mechanisms of failure. The anterior column is defined as the anterior longitudinal ligament, the anterior half of the VB, and the anterior half of the annulus fibrosis. The posterior column consists of everything posterior to the posterior longitudinal ligament: the facet joints, pedicles, and supraspinous ligaments. The novel middle column contains a middle osteoligamentous complex formed by the posterior half of the VB, the posterior longitudinal ligament, and posterior annulus fibrosus (▶Fig. 2.7).74
As this model has an additional column, novel mechanisms of injury are described. There are four major types: compression, burst, seatbelt type, and flexion–distraction. Compression fractures are classified according to whether they are caused by anterior or lateral flexion. These injuries cause anterior column compression sometimes associated with posterior column distraction. Burst fractures are classified according to whether an axial load alone caused the fractures or whether flexion, rotation, and/or lateral flexion are also involved. These injuries cause anterior and middle column compression, and may sometimes also produce associated posterior column distraction. Seatbelt fractures are defined by their distinctive flexion–disruption mechanism of injury. The anterior column may be intact or distracted, but the middle and posterior columns are distracted. Fracture-dislocations are classified according to whether the dislocation involves rotation, shear, or flexion–distraction. Each of these injuries is further subdivided and can produce any pattern of column involvement (▶Table 2.2 and ▶Fig. 2.8). Minor fractures—those of the transverse processes, articular processes, pars interarticularis, and spinous processes involve only a part of the posterior column and are not thought to lead to acute instability.75
Fig. 2.7 Illustration of the three columns of the spine as described by Denis. (a) Axial view. The lateral views show the (b) anterior, (c) middle, and (d) posterior columns and their anatomic contents. (Source: Khanna A, ed. Traumatic conditions. In: MRI Essentials for the Spine Specialist. 1st ed. New York, NY: Thieme; 2014.)
Using this system, only compression fractures without involvement of the posterior wall would be amenable to treatment with vertebral augmentation. While low-velocity compression fractures were currently considered stable, Denis felt that all burst fractures were unstable and required surgical instrumentation for stabilization. As every burst fracture required the same treatment, the five subdivisions were thought to be of little value.
Table 2.2 Denis’ classification of spinal fracture
Type |
Mechanism |
Columns involved |
Compression • Anterior • Lateral |
Flexion Anterior flexion Lateral flexion |
Anterior column compression with/without posterior column distraction |
Burst • A • B • C • D • E |
Axial load Axial load plus flexion Axial load plus flexion Axial load plus rotation Axial load plus lateral flexion |
Anterior and middle column compression with/without posterior column distractionz |
Seatbelt |
Flexion–distraction |
Anterior column intact or distracted; middle and posterior column distraction |
Fracture-dislocation • Flexion–rotation • Shear • Flexion–distraction |
Flexion–rotation Shear (anteroposterior or posteroanterior) Flexion–distraction |
Any columns can be affected (alone or in combination) |
Source: Adapted from Dr. B. Nurboja and Mr. D. Choi. |
||
Fig. 2.8 Denis’ definitions of types of spinal fracture. (Adapted from Denis.75)
The following year, McAfee et al simplified this system and was the first to describe a stable burst fracture: a fracture having anterior and middle column compression without posterior column disruption. The McAfee system of classifying acute traumatic spinal injuries is based on three forces (axial compression, axial distraction, and translation within the transverse plane) as they act to injure the middle column. Computed tomography can be used as a reliable method of identifying unstable burst fractures by illustrating facet joint subluxation or disruption of the neural arch.76 With this system, vertebral augmentation would be appropriate for compression fractures, including stable burst fractures.
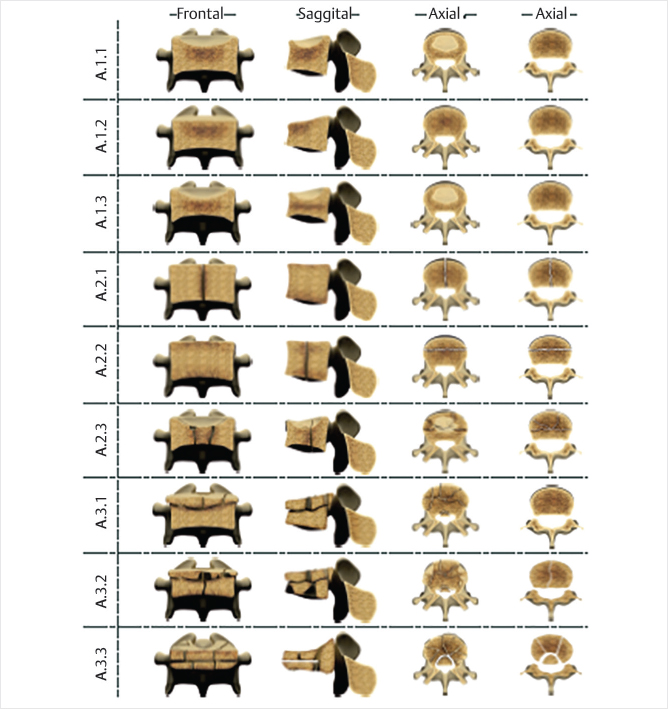
The AO (Arbeitsgemeinshaft fur Osteosynthesefragen) Classification is a highly detailed system published in 1994 by Magerl et al.61 This Swiss system returns to a two-column model and remains the basis for modern fracture fixation. It classifies thoracolumbar fractures into three major groups based on the mechanism of injury: compression (type A), distraction (type B), and multidirectional with translation or torsion (type C). It takes into account the morphological appearance, the direction of the force or mechanism of injury, and increasing destruction of the injury.77 Its comprehensive description includes the nature of injury, the degree of instability, and prognostic aspects that are important for choosing the most appropriate treatment.
The modified AO classification includes morphology of the fracture, neurological status, and description of relevant patient-specific modifiers (▶Fig. 2.9).78 The fracture morphology is assessed based on three main injury patterns: type A0–A4 (compression injury to the VB without posterolateral ligamentous complex [PLC] involvement), type B1–B3 (tension band disruption—the failure of posterior [PLC] or anterior [anterior longitudinal ligament] constraints), and type C (translation injuries). Neurologic status is classified as follows: no neurologic injury (N0), transient (resolved) neurologic deficit (N1), radicular symptoms (N2), incomplete spinal cord injury or any degree of cauda equina injury (N3), complete spinal cord injury (N4), and unknown neurologic status (NX). Two modifiers were also included: M1 to indicate indeterminate posterolateral complex status and M2 to designate patient-specific comorbidity (that might preclude general anesthesia and surgery, such as ankylosing spondylitis or diffuse burns overlying the surgical approach).
Based on this classification, type A4 fractures (burst fracture or sagittal split involving both end plates) and B1–B3 and C injuries almost always require instrumented surgical stabilization for optimal outcome.11 Vertebral augmentation may be indicated to treat type A injuries, specifically, A1.1, A1.2, A1.3, A2.1, A2.2, A2.3 and A3.1.
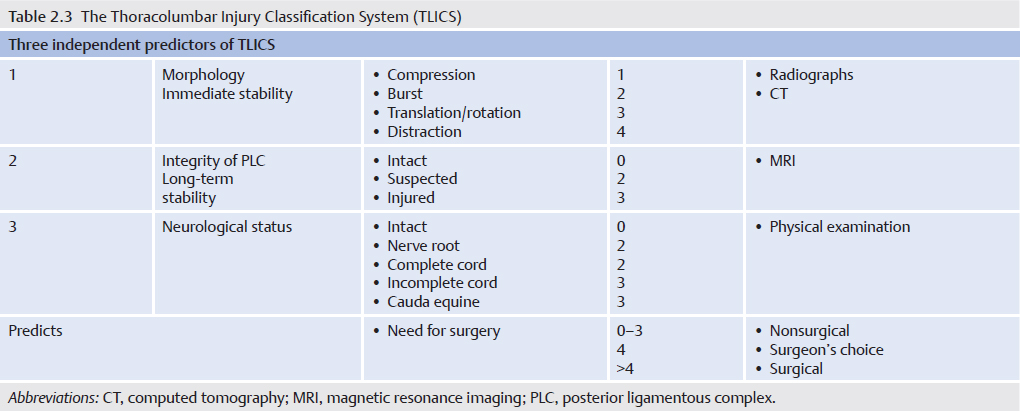
The Thoracolumbar Injury Classification and Severity Scale. (TLICS) was introduced in 2005 by the Spine Trauma Study Group (STSG; ▶Table 2.3). It has been validated and shown to have good reliability. It uses a composite scoring system based on the mechanism of injury (as determined by the morphology on imaging), integrity of the posterior ligamentous complex, and neurological status of the patient.79 Evaluation of the PLC requires MR imaging, a modality that has limited worldwide availability.80 The TLICS is designed to assist in clinical management of thoracolumbar spine injuries and uses features important in predicting spinal stability, future deformity, and progressive neurologic compromise, as well as predicting appropriate treatment recommendations.79,81 The three major morphologic descriptors are compression or burst, rotation/translation, and distraction. For compression injuries, the prefixes axial, flexion, or lateral more precisely describe the injury morphology.
A score of 3 or less, as with compression injuries, suggests a stable fracture, while a score of 5 or more suggests that surgical instrumentation for stabilization should be considered. This classification system also provides a guide for determining the optimal approach (anterior, posterior, and combined anteroposterior) for surgically treated patients based on the status of the posterior ligamentous complex and the patient’s neurologic status. A score of 4 might be handled conservatively or surgically, according to the physician’s judgment. A1, A2, and A3.1 fractures as classified by the AO system would be assigned 0 to 3 points using the TLICS system and vertebral augmentation would be included in the treatment options.
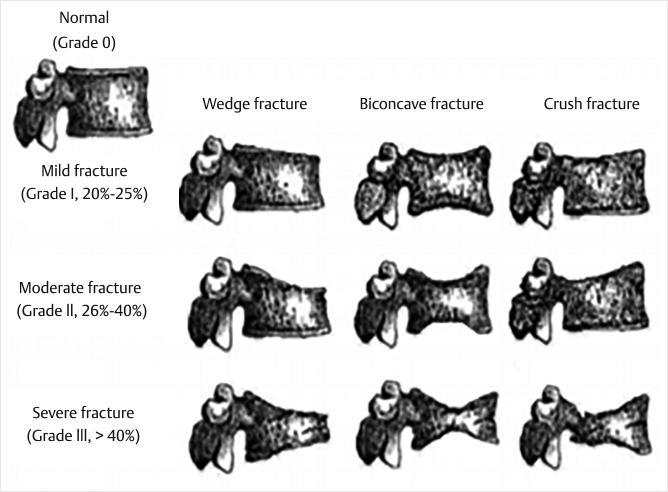
The systems described above were all designed to identify spinal instability and ultimately to guide treatment. The Genant semiquantitative method of classifying osteoporotic vertebral fractures was introduced in 1993 by Harry Genant, who noted82:
“Vertebral fractures are the most common consequence of osteoporosis, occurring in a substantial portion of the post-menopausal population. Most vertebral fractures, however, are not clinically recognized, and can accumulate silently. It is established that the presence of a vertebral fracture is a strong risk factor for subsequent osteoporotic fractures, and that those with low bone density and vertebral fractures are at highest risk.”
Prior to the introduction of the Genant system, osteoporotic vertebral fractures were frequently underdiagnosed worldwide, with false-negative rates as high as 30% despite a strict radiographic protocol that provided an unambiguous vertebral fracture definition and minimized the influence of inadequate film quality. Failure was a global problem attributable to either the lack of radiographic detection or a use of ambiguous terminology in imaging reports. A standardized method for viewing and describing vertebral fractures was needed.83
The Genant classification system is based on height loss involving the anterior, posterior, and/or middle VB (▶Fig. 2.10). In this semiquantitative assessment, each vertebra receives a severity grade based upon the degree of vertebral height loss. Unlike the other approaches, the type of the deformity (wedge, biconcavity, or compression) is not linked to grading. Thoracic and lumbar vertebrae from T4 to L4 are graded on visual inspection and without direct vertebral measurement as normal (grade 0), mildly deformed (grade 1: reduction of 20–25% of height over 10–20% of the vertebral area), moderately deformed (grade 2: reduction of 26–40% of height over 21–40% of the vertebral area), or severely deformed (grade 3: reduction of >40% of height and vertebral area; grade 0.5 designates “borderline” vertebrae that show some deformation but cannot be clearly assigned as a grade 1 fracture.)
The Genant semiquantitative method has been tested and applied in a number of clinical drug trials and epidemiological studies.82,84–87 The reproducibility of the method for the diagnosis of prevalent and incident vertebral fractures was found to be high, with intraobserver agreement of 93 to 99% and interobserver agreement of 90 to 99%. In experienced hands, the approach is both sensitive and specific.87 A “spinal fracture index” can be calculated from this semiquantitative assessment as the sum of all grades assigned to the vertebrae divided by the number of the evaluated vertebrae. Loss of individual vertebral height can be assessed on serial imaging for a meaningful interpretation of follow-up radiographs.7
The rationale for vertebral augmentation in stable vertebral fractures, regardless of etiology, is preservation or restoration of vertebral height, stabilization, or correction of kyphotic angulation and elimination of pain, allowing patients an early return to activity.
Prior to the introduction of vertebral augmentation procedures, management of patients with stable osteoporotic VCFs consisted primarily of rest, analgesic medications, and immobilization in an orthotic brace. Many of these patients develop disabling pain, deformity (kyphosis), and reduced pulmonary function. Additionally, bone loss in osteoporotic patients is accelerated by inactivity and may lead to continued and accelerated bone loss at a rate of up to 2% per week.9 Weight bearing is an important factor in preventing bone loss and is an important step toward halting or slowing progressive bone loss in the patients.88–92 While medical management, including nonsteroidal anti-inflammatory drugs, calcitonin, teriparatide, abaloparatide, bisphosphonates, and parathyroid hormone have been shown to offer some benefit in pain control and function, medications do carry risks of side effects. For example, bisphosphonates have been associated with osteonecrosis of the jaw and atypical femoral fractures.
In geriatric patients with osteoporotic vertebral fractures, including those involving the posterior wall of the VB, kyphoplasty has been shown to be an effective procedure with only rare complications. Between 2002 and 2008, Krüger et al performed kyphoplasty on 97 patients, each with at least one AO classification A3.1 fracture. Ninety-seven patients (68 females; average age: 76.1 [59–98 years]) with involvement of the vertebra’s posterior margin were treated by kyphoplasty. The fractures of 75 patients were caused by falls from little height, 5 patients had suffered traffic accidents, and in the case of 17 patients, no type of trauma was remembered. According to the AO classification, there were 109 A3.1.1 fractures and 1 A3.1.3 fracture. Prior to surgery, all patients were neurologically intact. Seventy-nine fractures were accompanied by a narrowing of the spinal canal with a mean degree of narrowing of 15% (10–40). Overall, 134 vertebrae were treated by balloon kyphoplasty (81 × 1 VB, 22 × 2 VB, 3 × 3 VB). Cement leakage was observed after surgery in 47.4% of patients but in every case, patients remained asymptomatic form the leakage. Using the Visual Analog Scale (VAS 1–10), patients stated that prior to surgery their pain averaged 8.1, whereas after surgery it significantly decreased and averaged 1.6 (p < 0.001).93
In patients with pathologic fractures due to neoplasia, various types of medical, surgical, and radiologic oncology management are most often indicated for the primary disease. Treatment of pathologic fractures due to malignancy may include radiation, radiofrequency ablation, vertebral augmentation, and/or open surgical procedures to decompress neural elements, reduce tumor burden, and stabilize the spine.94 Evidence has shown that vertebral augmentation dramatically reduces pain and improves quality of life.95,96
In a systematic review to assess the efficacy of kyphoplasty in controlling pain and improving quality of life in oncologic patients with metastatic spinal disease or MM and pathologic compression fractures of the spine, Astur and Avanzi found moderate evidence that patients treated with balloon kyphoplasty displayed better scores for pain (Numeric Pain Rating Scale), disability (Roland–Morris Disability Questionnaire), quality of life (Short Form 36 [SF-36] Health Survey), and functional status (Karnofsky Performance Status) compared with those undergoing the conventional treatment. Patients treated with kyphoplasty also have better recovery of vertebral height.
The control group was any other treatment modality. This study concluded that balloon kyphoplasty could be considered as an early treatment option for patients with symptomatic neoplastic spinal disease, and called for further randomized clinical trials (RCTs) to improve the quality of evidence.97
An earlier RCT compared balloon kyphoplasty with nonsurgical management (NSM) and allowed an optional crossover at 1 month after enrollment and included patients with various neoplastic disorders including MM and breast, lung, and prostate cancers. They found statistically significant improvements in the patients’ pain, function, and quality of life as measured by the Numeric Rating Scale, the Roland–Morris Disability Questionnaire, and the SF-36 Health Survey, respectively. There was either no change in quality of life and activity or minimal change in back pain in the NSM patients. Seventy-three percent of the patients who initially received NSM crossed over to balloon kyphoplasty and 55% of these patients crossed over within on1 week of their 1-month follow-up visit. They concluded that balloon kyphoplasty provided better results than NSM at 1 month in all measures and these improvements seen at 1 month were generally sustained at 1 year. They also concluded the balloon kyphoplasty was safe for use in patients with neoplastic VB involvement as the number of patients with adverse events was similar between the balloon kyphoplasty and NSM groups.
Importantly, no system used to classify traumatic vertebral fractures addresses sagittal balance or persistent clinical ailments. The most frequently used classifications in traumatic vertebral fracture assessment are AO and TLICS. Using the AO classification scale, injuries classified as A1, A2 (except for pincer fractures: A2.3), and A3.1 are stable and may be treated with vertebral augmentation. Specifically, A1.1, A1.2, A1.3, A2.1, A2.2, and A3.1 may be safely treated with vertebral augmentation. According to the TLICS system, these same fractures are estimated as 3 or less points, do not require surgical instrumentation for stabilization, and are amenable to treatment with vertebral augmentation.
In fractures amenable to vertebral augmentation, Chen et al. found significant reductions in hospitalization time and mortality in patients treated with vertebral augmentation as compared with those patients treated with NSM.1 A more recent study showed slightly longer hospitalization but greater discharge to home for augmented patients as compared to much higher rates of discharge to long-term care facilities in the patients treated with NSM.6 Recent Medicare claims–based analyses of over 1 million VCF patients with 5- to 10-year follow-up, performed with propensity score matching to account for selection bias, concluded that there was a highly statistically significant reduction of both morbidity and mortality in patients treated with vertebral augmentation as compared to those treated with NSM.3,6 In these analyses comparing NSM to vertebral augmentation, NSM patients had significantly higher rates of pneumonia, deep venous thrombosis, cardiac complications, and urinary tract infections.3,6
Treatment of symptomatic VCFs with vertebral augmentation (vertebroplasty or kyphoplasty) has been shown in various studies to be a cost-effective intervention that both decreases pain and improves survival.98–100
Osteoporosis and associated osteoporotic fractures have a profound economic burden and public health impact. The number of osteoporotic fractures diagnosed annually may, in fact, be a gross underestimate given, as has been mentioned previously, that only an estimated one-third of all vertebral fractures are clinically diagnosed.33 This impacts the reimbursement strategies of payers, influences policy makers in the public health sector, and encourages the pharmaceutical companies to conduct clinical trials for new agents to reduce fracture risk.101
More recent data suggest that osteoporotic VCFs affect up to one million persons in the United States annually, and 25% of woman in their lifetime.20,102 A retrospective analysis using the Premier Perspective Database (now Premier Healthcare Database) revealed that among all osteoporosis-related fracture admissions for the years 2010 to 2013, the mean hospital cost was $12,839 (95% confidence interval [CI]) and the mean length of stay (LOS) was 5.1 days. During the admission, 7.4% of the patients were sent to the intensive care unit and the mortality rate was 1.5% with an additional or adjacent fracture occurring in 2.3% of the patients during the 60-day postdischarge period103 The majority of costs are incurred by inpatient care, long-term care facilities, and then outpatient care in that order.32 In the year following a fracture, medical and hospitalization costs were 1.6 to 6.2 times higher than prefracture costs and 2.2 to 3.5 times higher than those for matched controls with costs totaling up to $71,000 for a hip fracture and up to $68,000 for a vertebral fracture.104 Medicare pays for approximately 80% of these costs.32 In addition to the medical costs, there are other significant indirect costs that include reduced productivity due to disability, reduced earnings, and premature death.105 The cost of care of osteoporosis, in part due to an aging population, is expected to rise to $25.3 billion by 2025.32
Patients with bone metastasis secondary to prostate or breast cancer or MM are predisposed to skeletal-related events (SREs), including surgery or radiation to the spinal column, pathologic fractures, and spinal cord compression. Barlev et al examined costs from a payer perspective for SRE-associated hospitalizations among patients with MM or bone metastasis secondary to prostate or breast cancer.106 Patients with SRE hospitalizations were selected from the MarketScan commercial and Medicare databases (from January 1, 2003, through June 30, 2009). Sampled patients had on the average at least two medical claims with primary or secondary ICD-9-CM diagnosis codes for prostate cancer, breast cancer, or MM, and at least one subsequent hospitalization with principal diagnosis or procedure codes indicating bone surgery, pathologic fracture, or spinal cord compression. A total of 555 patients had 572 hospitalizations. The mean age range was 61 to 72 years, and the range of mean LOS per admission was from 5.9 to 11.6 days. The range of mean health plan payment per hospital admission across tumor types was $22,390 to 26,936 for pathologic fracture without spinal cord compression.106
When considering the estimated costs of hospital care and outpatient visits for patients with traumatic thoracolumbar spine fractures, one must remember that, although the LOS for patients treated operatively may be shorter than those treated nonoperatively, the total costs, including surgical expenses, may be higher. Cost-effectiveness then becomes central. That is, surgery must offer a better outcome for the increased cost. Outcomes must be factored into the analysis for a reliable cost-effective value. Unstable fractures and those with neurologic impairment may require surgical treatment, extensive rehabilitative services, and these patients often develop long-term disability.107
Siebenga et al compared surgical versus nonsurgical treatment for management of individuals with traumatic thoracolumbar spine fractures. This study included direct costs, general-practitioner visit and absenteeism costs, and private health care expenditures. The study included individuals with traumatic thoracolumbar spine fractures (T10–L4 fractures without neurological deficit) treated between 1998 and 2003 in a single European institution. Mean direct costs during this time period for the surgical treatment (US$ 21,960) were significantly higher than those for the conservative management (US$ 11,880). However, the general-practitioner visit costs, private expenditures, and absenteeism costs for the surgical group (US$ 13, US$ 550, and US$ 6630, respectively) were significantly lower than those for the nonsurgical group (US$ 34, US$ 816, and US$ 10,329, respectively).108
The Nationwide Emergency Department Sample (NEDS) is a set of hospital-based emergency department databases included in the Healthcare Cost and Utilization Project (HCUP) family. These databases are created by the Agency for Healthcare Research and Quality (AHRQ) through a Federal-State-Industry partnership. Based on the HCUP Nationwide Inpatient Sample (NIS) and NEDS databases queried, there were an estimated 795,300 hospital discharges and emergency department visits for spinal fractures in the United States in 2010–2011. The great majority of spinal fracture patients (773,000, or 97%) were treated for osteoporotic or pathologic VCFs with little or no trauma. Nearly half of discharges and visits for VCFs were for patients 75 years and older and 58% were females.107 Traumatic fractures were far less common, with 27,100 (3%) hospital discharges or outpatient visits reported. Numbers were too small for reliable reporting in the National Center for Health Statistics (NCHS) databases, which include outpatient and physician office visits. These fractures predominantly involved men (~60%) and were most likely to involve patients between the ages of 18 and 44 years.107
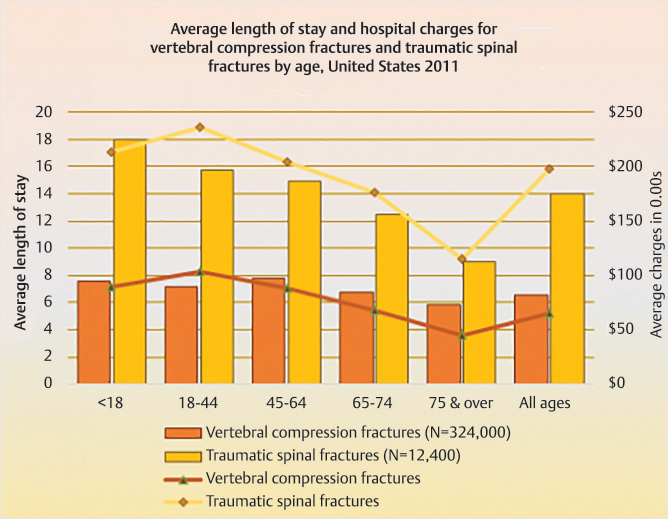
The average LOS for patients with a spine fracture diagnosis was 6.8 days and the average charge was $69,500. For patients with traumatic spinal fractures, the average hospital stay was more than twice as long as for osteoporotic/pathologic VCFs (14 vs. 6.6 days), and average charges three times as high ($197,700 vs. 65,700). Differences in LOS and charges were shown to be greater for those younger than 45 years (▶Fig. 2.11).
Fig. 2.11 Average length of stay and hospital charges for osteoporotic VCFs and traumatic spinal fractures by age in the United States, 2011. Source: United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed on [8/12/2018].
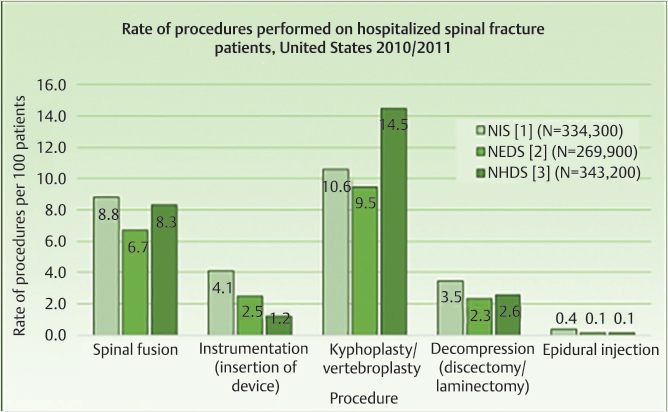
Fig. 2.12 Inpatient procedures for spinal fractures in the United States, 2010/2011. Source: United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org. Accessed on [8/12/2018].
Only a small proportion of patients hospitalized with any spinal fracture undergo surgery (▶Fig. 2.12). According to the NIS database, fusion (8.8%) and vertebral augmentation (kyphoplasty or vertebroplasty, 10.6%) are the most common procedures performed. Similar rates of procedures were found in the NEDS hospitalized patients and National Hospital Discharge Survey (NHDS) databases. Of patients discharged with the diagnosis of VCF, only 12% were treated with kyphoplasty or vertebroplasty. These patients were twice as likely to be female, and were most likely to be 65 years or older. The majority of spinal fusion procedures were performed on patients younger than 44 years with traumatic fractures.107
Cost-effectiveness analysis is a way of determining the value of an intervention.
Determining an acceptable cost-effectiveness threshold, that is, the amount we are willing to pay for an intervention, is a value judgment. Patients may have different thresholds than payers. Garber and Phelps suggest that “most, but not all, decision makers in the United States will conclude that interventions that cost less than $50,000 to $60,000 per quality-adjusted life year (QALY) gained are reasonably efficient.”109,110
In 2013, Borse performed cost–utility analysis of balloon kyphoplasty and vertebroplasty, the two most commonly employed augmentation procedures used to treat osteoporotic VCFs. The cost–utility ratio for vertebroplasty was $34,688 per QALY gained and that for a balloon kyphoplasty was $32,767 per QALY gained. In an incremental comparison between kyphoplasty and vertebroplasty, balloon kyphoplasty was more cost-effective when compared to vertebroplasty.111
For additional information regarding the cost-effectiveness of vertebral augmentation refer to Chapter 16: Cost-Effectiveness of Vertebral Augmentation.
VCFs can lead to severe pain, physical limitation and disability, and increased morbidity and mortality. In patients with conditions such as osteoporosis or malignancy, pathologic weakening of the bone allows even the most minor trauma to result in fractures. These fractures are very common and the public health and economic impact is considerable. The most common causes of vertebral fractures are osteoporosis, metastatic disease, MM, and trauma. Regardless of etiology, timely and accurate diagnosis is essential to determine the appropriate treatments.
Trauma patients with injuries leading to an unstable spine must be treated rapidly and with great attention to mechanism of injury, the type of injury, and the treatment necessary to adequately protect the spine. It is equally important to provide an accurate and timely diagnosis in patients with metastatic malignancies to the spine and in elderly patients with osteoporotic VCFs. One must consider all safe treatment options and the implications and literature evidence supporting these options. Conservative therapy often consists simply of rest and optimal pain management, but care must be taken to avoid dismissing the effects of pain and the side effects or lack of efficacy of medical management. Importantly, bed rest in an osteoporotic patient may accelerate bone loss, worsen the patient’s functional status, and significantly increase their chances of morbidity and mortality.
Given the social, public health, and economic impact of osteoporotic VCFs, it is imperative to understand the natural history of osteoporosis and invest not only in the interventional treatment of these fractures but also in the prevention of future fractures by treating the underlying condition of osteoporosis and in education of the patient of their underlying disease process that produced the osteoporotic fracture. When a compression fracture is secondary to osteoporosis, the physician should explain what osteoporosis is, why the patient likely has it, and how to best treat their condition, and to make sure that the patient receives treatment by either the physician that performs the vertebral augmentation or an osteoporosis specialty clinic. This is a treatment pathway that will optimize the patient’s bone health and reduce or prevent future fragility fractures. In addition to optimizing treatment, it is important that the patient understand the importance of bone health and the benefits of lifestyle modification such as adequate intake of calcium and vitamin D as well as exercise and fall prevention.
Vertebral augmentation offers safe and durable pain relief and an opportunity to significantly improve quality of life with an excellent risk–benefit ratio across a wide range of etiologies.
[1] Chen AT, Cohen DB, Skolasky RL. Impact of nonoperative treatment, vertebroplasty, and kyphoplasty on survival and morbidity after vertebral compression fracture in the medicare population. J Bone Joint Surg Am 2013;95(19): 1729–1736
[2] Zampini JM, White AP, McGuire KJ. Comparison of 5766 vertebral compression fractures treated with or without kyphoplasty. Clin Orthop Relat Res 2010;468(7):1773–1780
[3] Edidin AA, Ong KL, Lau E, Kurtz SM. Morbidity and mortality after vertebral fractures: comparison of vertebral augmentation and nonoperative management in the Medicare population. Spine 2015;40(15):1228–1241
[4] Lange A, Kasperk C, Alvares L, Sauermann S, Braun S. Survival and cost comparison of kyphoplasty and percutaneous vertebroplasty using German claims data. Spine 2014;39(4):318–326
[5] Silverman SL. The clinical consequences of vertebral compression fracture. Bone 1992;13(Suppl 2):S27–S31
[6] Ong KL, Beall DP, Frohbergh M, Lau E, Hirsch JA. Were VCF patients at higher risk of mortality following the 2009 publication of the vertebroplasty “sham” trials? Osteoporos Int 2018;29(2):375–383
[7] Grigoryan M, Guermazi A, Roemer FW, Delmas PD, Genant HK. Recognizing and reporting osteoporotic vertebral fractures. Eur Spine J 2003;12(Suppl 2):S104–S112
[8] Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser 1994;843:1–129
[9] Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR; Study of Osteoporotic Fractures Research Group. Vertebral fractures and mortality in older women: a prospective study. Arch Intern Med 1999;159(11):1215–1220
[10] Baaj AA, Downes K, Vaccaro AR, Uribe JS, Vale FL. Trends in the treatment of lumbar spine fractures in the United States: a socioeconomics perspective: clinical article. J Neurosurg Spine 2011;15(4):367–370
[11] Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: an overview. Indian J Orthop 2015;49(1):72–82
[12] Wood KB, Li W, Lebl DR, Ploumis A. Management of thoracolumbar spine fractures. Spine J 2014;14(1):145–164
[13] el-Khoury GY, Whitten CG. Trauma to the upper thoracic spine: anatomy, biomechanics, and unique imaging features. AJR Am J Roentgenol 1993;160(1):95–102
[14] Gertzbein SD. Scoliosis Research Society. Multicenter spine fracture study. Spine 1992;17(5):528–540
[15] Harrison RA, Siminoski K, Vethanayagam D, Majumdar SR. Osteoporosis-related kyphosis and impairments in pulmonary function: a systematic review. J Bone Miner Res 2007;22(3):447–457
[16] Cosman F, de Beur SJ, LeBoff MS, et al; National Osteoporosis Foundation. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 2014;25(10):2359–2381
[17] Lindsay R, Silverman SL, Cooper C, et al. Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285(3):320–323
[18] Ensrud KE, Schousboe JT. Clinical practice. Vertebral fractures. N Engl J Med 2011;364(17):1634–1642
[19] Felsenberg D, Silman AJ, Lunt M, et al; European Prospective Osteoporosis Study (EPOS) Group. Incidence of vertebral fracture in europe: results from the European Prospective Osteoporosis Study (EPOS). J Bone Miner Res 2002;17(4):716–724
[20] Riggs BL, Melton LJ III. The worldwide problem of osteoporosis: insights afforded by epidemiology. Bone 1995;17(5, Suppl):505S–511S
[21] NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy, March 7–29, 2000: highlights of the conference. South Med J 2001;94(6):569–573
[22] Heaney RP, Abrams S, Dawson-Hughes B, et al. Peak bone mass. Osteoporos Int 2000;11(12):985–1009
[23] Ballane G, Cauley JA, Luckey MM, El-Hajj Fuleihan G. Worldwide prevalence and incidence of osteoporotic vertebral fractures. Osteoporos Int 2017;28(5):1531–1542
[24] Prevention and Management of Osteoporosis: report of a WHO Scientific Group. Paper presented at WHO Scientific Group on the Prevention and Management of Osteoporosis2000; Geneva, Switzerland
[25] Wright NC, Saag KG, Dawson-Hughes B, Khosla S, Siris ES. The impact of the new National Bone Health Alliance (NBHA) diagnostic criteria on the prevalence of osteoporosis in the United States: supplementary presentation. Osteoporos Int 2017;28(11):3283–3284
[26] Cosman F, Krege JH, Looker AC, et al. Spine fracture prevalence in a nationally representative sample of US women and men aged ≥40 years: results from the National Health and Nutrition Examination Survey (NHANES) 2013–2014. Osteoporos Int 2017;28(6):1857–1866
[27] Wong CC, McGirt MJ. Vertebral compression fractures: a review of current management and multimodal therapy. J Multidiscip Healthc 2013; 6:205–214
[28] Francis RM, Baillie SP, Chuck AJ, et al. Acute and long-term management of patients with vertebral fractures. QJM 2004;97(2):63–74
[29] Nevitt MC, Cummings SR, Stone KL, et al. Risk factors for a first-incident radiographic vertebral fracture in women > or = 65 years of age: the study of osteoporotic fractures. J Bone Miner Res 2005;20(1):131–140
[30] Melton LJ III, Lane AW, Cooper C, Eastell R, O’Fallon WM, Riggs BL. Prevalence and incidence of vertebral deformities. Osteoporos Int 1993;3(3):113–119
[31] O’Neill TW, Felsenberg D, Varlow J, Cooper C, Kanis JA, Silman AJ. The prevalence of vertebral deformity in european men and women: the European Vertebral Osteoporosis Study. J Bone Miner Res 1996;11(7):1010–1018
[32] Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 2007;22(3):465–475
[33] Cooper C, Atkinson EJ, O’Fallon WM, Melton LJ III. Incidence of clinically diagnosed vertebral fractures: a population-based study in Rochester, Minnesota, 1985–1989. J Bone Miner Res 1992;7(2):221–227
[34] Cho JH, Ha JK, Hwang CJ, Lee DH, Lee CS. Patterns of treatment for metastatic pathological fractures of the spine: the efficacy of each treatment modality. Clin Orthop Surg 2015;7(4):476–482
[35] Saad F, Lipton A, Cook R, Chen YM, Smith M, Coleman R. Pathologic fractures correlate with reduced survival in patients with malignant bone disease. Cancer 2007;110(8):1860–1867
[36] Beall DP, Chambers MR, Thomas S, et al. Prospective and multicenter evaluation of outcomes for quality of life and activities of daily living for balloon kyphoplasty in the treatment of vertebral compression fractures: the EVOLVE Trial. Neurosurgery 2019;84(1):169–178
[37] Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015;65(1):5–29
[38] Mitsiades CS, Mitsiades N, Munshi NC, Anderson KC. Focus on multiple myeloma. Cancer Cell 2004;6(5):439–444
[39] Anitha D, Baum T, Kirschke JS, Subburaj K. Risk of vertebral compression fractures in multiple myeloma patients: a finite-element study. Medicine (Baltimore) 2017;96(2):e5825
[40] Howlader N, Noone A, Krapcho M. SEER Cancer Statistics Review, 1975–2013. 2016. http://seer.cancer.gov/csr/1975_2013/
[41] Edwards BJ, Langman CB, Bunta AD, Vicuna M, Favus M. Secondary contributors to bone loss in osteoporosis related hip fractures. Osteoporos Int 2008;19(7):991–999
[42] Anselmetti GC, Manca A, Montemurro F, et al. Percutaneous vertebroplasty in multiple myeloma: prospective long-term follow-up in 106 consecutive patients. Cardiovasc Intervent Radiol 2012;35(1):139–145
[43] Mirza F, Canalis E. Management of endocrine disease: secondary osteoporosis: pathophysiology and management. Eur J Endocrinol 2015;173(3): R131–R151
[44] Pittari G, Costi D, Raballo M, Maulucci L, Baroni MC, Mangoni M. Intravenous neridronate for skeletal damage treatment in patients with multiple myeloma. Acta Biomed 2006;77(2):81–84
[45] Tipples K, Robinson A. Optimal management of cancer treatment-induced bone loss: considerations for elderly patients. Drugs Aging 2011;28(11): 867–883
[46] Sezer O. Myeloma bone disease: recent advances in biology, diagnosis, and treatment. Oncologist 2009;14(3):276–283
[47] Faiman B, Licata AA. New tools for detecting occult monoclonal gammopathy, a cause of secondary osteoporosis. Cleve Clin J Med 2010;77(4):273–278
[48] Layton KF, Thielen KR, Cloft HJ, Kallmes DF. Acute vertebral compression fractures in patients with multiple myeloma: evaluation of vertebral body edema patterns on MR imaging and the implications for vertebroplasty. AJNR Am J Neuroradiol 2006;27(8):1732–1734
[49] Kanis JA. Diagnosis of osteoporosis and assessment of fracture risk. Lancet 2002;359(9321):1929–1936
[50] Golombick T, Diamond T. Prevalence of monoclonal gammopathy of undetermined significance/myeloma in patients with acute osteoporotic vertebral fractures. Acta Haematol 2008;120(2):87–90
[51] Weiss BM, Abadie J, Verma P, Howard RS, Kuehl WM. A monoclonal gammopathy precedes multiple myeloma in most patients. Blood 2009;113(22): 5418–5422
[52] Tosi P. Diagnosis and treatment of bone disease in multiple myeloma: spot-light on spinal involvement. Scientifica (Cairo) 2013;2013:104546
[53] Coleman R. Skeletal Complications of Malignancy. Skeletal Complications of Malignancy Symposium, Bethesda, MD; 1997
[54] Borggrefe J, Giravent S, Thomsen F, et al. Association of QCT bone mineral density and bone structure with vertebral fractures in patients with multiple myeloma. J Bone Miner Res 2015;30(7):1329–1337
[55] Anitha D, Kim KJ, Lim SK, Lee T. Implications of local osteoporosis on the efficacy of anti-resorptive drug treatment: a 3-year follow-up finite element study in risedronate-treated women. Osteoporos Int 2013;24(12): 3043–3051
[56] British Committee for Standards in Haematology in Conjunction with the UK Myeloma Forum(UKMF). Guidelines on the Diagnosis and Management of Multiple Myeloma. 2010. http://www.bcshguidelines.com/. Accessed May 1, 2018
[57] Mulligan M, Chirindel A, Karchevsky M. Characterizing and predicting pathologic spine fractures in myeloma patients with FDG PET/CT and MR imaging. Cancer Invest 2011;29(5):370–376
[58] Singh A, Tetreault L, Kalsi-Ryan S, Nouri A, Fehlings MG. Global prevalence and incidence of traumatic spinal cord injury. Clin Epidemiol 2014;6: 309–331
[59] Hu R, Mustard CA, Burns C. Epidemiology of incident spinal fracture in a complete population. Spine 1996;21(4):492–499
[60] Gertzbein SD, Khoury D, Bullington A, St John TA, Larson AI. Thoracic and lumbar fractures associated with skiing and snowboarding injuries according to the AO comprehensive classification. Am J Sports Med 2012;40(8): 1750–1754
[61] Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S. A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 1994;3(4):184–201
[62] Kraemer WJ, Schemitsch EH, Lever J, McBroom RJ, McKee MD, Waddell JP. Functional outcome of thoracolumbar burst fractures without neurological deficit. J Orthop Trauma 1996;10(8):541–544
[63] Knop C, Blauth M, Bühren V, et al. Surgical treatment of injuries of the thoracolumbar transition. 1: epidemiology Unfallchirurg 1999;102(12):924–935
[64] Benson DR, Burkus JK, Montesano PX, Sutherland TB, McLain RF. Unstable thoracolumbar and lumbar burst fractures treated with the AO fixateur interne. J Spinal Disord 1992;5(3):335–343
[65] McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am 1993;75(2):162–167
[66] Maynard FM Jr, Bracken MB, Creasey G, et al; American Spinal Injury Association. International Standards for Neurological and Functional Classification of Spinal Cord Injury. Spinal Cord 1997;35(5):266–274
[67] Watson-Jones R. The results of postural reduction of fractures of the spine. J Bone Joint Surg 1938;20:567–586
[68] Nicoll EA. Fractures of the dorso-lumbar spine. J Bone Joint Surg Br 1949;31B(3):376–394
[69] Holdsworth F. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg 1963;45:6
[70] Holdsworth F. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Am 1970;52(8):1534–1551
[71] Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord 1992;5(4):383–389, discussion 397
[72] White AA III, Johnson RM, Panjabi MM, Southwick WO. Biomechanical analysis of clinical stability in the cervical spine. Clin Orthop Relat Res 1975(109):85–96
[73] Allen BL Jr, Ferguson RL, Lehmann TR, O’Brien RP. A mechanistic classification of closed, indirect fractures and dislocations of the lower cervical spine. Spine 1982;7(1):1–27
[74] Denis F. Updated classification of thoracolumbar fractures. Orthopaedic Transactions 1982;6:8–9
[75] Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 1983;8(8):817–831
[76] McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of one hundred consecutive cases and a new classification. J Bone Joint Surg Am 1983;65(4): 461–473
[77] Gomleksiz C, Egemen E, Senturk S, et al. Thoracolumbar fractures: a review of classifications and surgical methods. J Spine 2015;4:250
[78] Vaccaro AR, Oner C, Kepler CK, et al; AOSpine Spinal Cord Injury & Trauma Knowledge Forum. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine 2013;38(23):2028–2037
[79] Lee JY, Vaccaro AR, Lim MR, et al. Thoracolumbar injury classification and severity score: a new paradigm for the treatment of thoracolumbar spine trauma. J Orthop Sci 2005;10(6):671–675
[80] Kepler CK, Vaccaro AR, Schroeder GD, et al. The Thoracolumbar AOSpine Injury Score. Global Spine J 2016;6(4):329–334
[81] West C, Roosendaal S, Bot J, Smithuis F. Spine Injury—TLICS Classification: Thoraco-Lumbar Injury Classification and Severity. http://www.radiologyas-sistant.nl/en
[82] Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 1993;8(9): 1137–1148
[83] Delmas PD, van de Langerijt L, Watts NB, et al; IMPACT Study Group. Underdiagnosis of vertebral fractures is a worldwide problem: the IMPACT study. J Bone Miner Res 2005;20(4):557–563
[84] Heuck AF, Block J, Glueer CC, Steiger P, Genant HK. Mild versus definite osteoporosis: comparison of bone densitometry techniques using different statistical models. J Bone Miner Res 1989;4(6):891–900
[85] Storm T, Thamsborg G, Steiniche T, Genant HK, Sørensen OH. Effect of intermittent cyclical etidronate therapy on bone mass and fracture rate in women with postmenopausal osteoporosis. N Engl J Med 1990;322(18):1265–1271
[86] Watts NB, Harris ST, Genant HK, et al. Intermittent cyclical etidronate treatment of postmenopausal osteoporosis. N Engl J Med 1990;323(2):73–79
[87] Wu CY, Li J, Jergas M, Genant HK. Comparison of semiquantitative and quantitative techniques for the assessment of prevalent and incident vertebral fractures. Osteoporos Int 1995;5(5):354–370
[88] Palombaro KM. Effects of walking-only interventions on bone mineral density at various skeletal sites: a meta-analysis. J Geriatr Phys Ther 2005;28(3):102–107
[89] Brown CJ, Friedkin RJ, Inouye SK. Prevalence and outcomes of low mobility in hospitalized older patients. J Am Geriatr Soc 2004;52(8):1263–1270
[90] Creditor MC. Hazards of hospitalization of the elderly. Ann Intern Med 1993;118(3):219–223
[91] Hoenig HM, Rubenstein LZ. Hospital-associated deconditioning and dysfunction. J Am Geriatr Soc 1991;39(2):220–222
[92] Harper CM, Lyles YM. Physiology and complications of bed rest. J Am Geriatr Soc 1988;36(11):1047–1054
[93] Krüger A, Zettl R, Ziring E, Mann D, Schnabel M, Ruchholtz S. Kyphoplasty for the treatment of incomplete osteoporotic burst fractures. Eur Spine J 2010;19(6):893–900
[94] Schuster JM, Grady MS. Medical management and adjuvant therapies in spinal metastatic disease. Neurosurg Focus 2001;11(6):e3
[95] Genev IK, Tobin MK, Zaidi SP, Khan SR, Amirouche FML, Mehta AI. Spinal compression fracture management: a review of current treatment strategies and possible future avenues. Global Spine J 2017;7(1):71–82
[96] Berenson J, Pflugmacher R, Jarzem P, et al; Cancer Patient Fracture Evaluation (CAFE) Investigators. Balloon kyphoplasty versus non-surgical fracture management for treatment of painful vertebral body compression fractures in patients with cancer: a multicentre, randomised controlled trial. Lancet Oncol 2011;12(3):225–235
[97] Astur N, Avanzi O. Balloon kyphoplasty in the treatment of neoplastic spne lesions: a systematic review. Global Spine J 2019;9(3):348–356
[98] Svedbom A, Alvares L, Cooper C, Marsh D, Ström O. Balloon kyphoplasty compared to vertebroplasty and nonsurgical management in patients hospitalised with acute osteoporotic vertebral compression fracture: a UK cost-effectiveness analysis. Osteoporos Int 2013;24(1): 355–367
[99] Garfin SR, Reilley MA. Minimally invasive treatment of osteoporotic vertebral body compression fractures. Spine J 2002;2(1):76–80
[100] Edidin AA, Ong KL, Lau E, Kurtz SM. Mortality risk for operated and nonoperated vertebral fracture patients in the medicare population. J Bone Miner Res 2011;26(7):1617–1626
[101] Siris ES, Adler R, Bilezikian J, et al. The clinical diagnosis of osteoporosis: a position statement from the National Bone Health Alliance Working Group. Osteoporos Int 2014;25(5):1439–1443
[102] Edidin AA, Ong KL, Lau E, Kurtz SM. Life expectancy following diagnosis of a vertebral compression fracture. Osteoporos Int 2013;24(2):451–458
[103] Weycker D, Li X, Barron R, Bornheimer R, Chandler D. Hospitalizations for osteoporosis-related fractures: economic costs and clinical outcomes. Bone Rep 2016;5:186–191
[104] Budhia S, Mikyas Y, Tang M, Badamgarav E. Osteoporotic fractures: a systematic review of U.S. healthcare costs and resource utilization. Pharmacoeconomics 2012;30(2):147–170
[105] Office of the Surgeon General. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: Office of the Surgeon General (US); 2004
[106] Barlev A, Song X, Ivanov B, Setty V, Chung K. Payer costs for inpatient treatment of pathologic fracture, surgery to bone, and spinal cord compression among patients with multiple myeloma or bone metastasis secondary to prostate or breast cancer. J Manag Care Pharm 2010;16(9): 693–702
[107] The Burden of Musculoskeletal Diseases in the United States(BMUS). Paper presented at United States Bone and Joint Initiative, Rosemont, IL; 2014
[108] Siebenga J, Segers MJ, Leferink VJ, et al. Cost-effectiveness of the treatment of traumatic thoracolumbar spine fractures: nonsurgical or surgical therapy? Indian J Orthop 2007;41(4):332–336
[109] Owens DK. Interpretation of cost-effectiveness analyses. J Gen Intern Med 1998;13(10):716–717
[110] Garber AM, Phelps CE. Economic foundations of cost-effectiveness analysis. J Health Econ 1997;16(1):1–31
[111] Borse MS. Cost utility analysis of balloon kyphoplasty and vertebroplasty in the treatment of vertebral compression fractures in the United States. Theses and Dissertations: University of Toledo: Toledo, OH; 2013