Fig. 4.1 Lateral conventional radiograph of the thoracic spine shows a wedge-type vertebral compression fracture of the T7 vertebral body (black arrow).
Summary
Certain painful spine conditions justify a more prompt approach to imaging evaluation and the most common of these conditions is a painful vertebral compression fracture. Although some fractures heal and are not painful, others are persistently very painful and cause a substantial amount of discomfort and debilitation. Due to the significant increase in morbidity and permanent loss of function, appropriate management of vertebral compression fractures (VCFs) is critically important. VCFs typically involve the anterior column and cause pain with transition from one position to another. In patients with profound osteoporosis VCFs can occur with very little force and the presence of one or more fractures progressively and dramatically increases the risk of sustaining additional VCFs. The signs and symptoms of fractures or back pain due to tumor or infections are called red flag conditions and must be recognized early to ensure prompt and appropriate treatment. Additionally the typical presentation of an osteoporotic VCF should be known to facilitate prompt fracture diagnosis. The patients usually present with transitional pain when moving from one position to another and reliable physical examination signs of a painful VCF include pain with closed fist percussion and pain when lying supine.
Keywords: vertebral compression fracture, physical examination, osteoporosis, closed-fist percussion, post-procedure management
It is known that the majority of spine pain is benign and will improve fairly rapidly. For this reason, most guidelines on the treatment of back pain generally recommend avoiding advanced imaging to reduce unnecessary expenditures and patient exposure to ionizing radiation. However, certain conditions justify more rapid utilization of advanced imaging and early treatment. The most prevalent of these conditions is compression fractures of the spine. These fractures occur when the bone is not of sufficient strength to handle the axial load applied to the vertebral body. The most common causes of loss of vertebral strength are osteoporosis and neoplasms involving the spine. Other conditions including infection of the vertebrae and high-velocity trauma can also predispose to vertebral fractures by weakening the vertebral body or by overwhelming the vertebral strength by force, respectively.
The incidence of VCFs has been rising over the last few decades, due to the rising age of our population. Many VCFs are asymptomatic and heal only to be identified incidentally on imaging studies. However, many of these fractures can cause severe pain and often become chronically painful, leading to substantial disability.1 In addition, the presence of multiple fractures, occurring over the course of months or years, may lead to hyperkyphosis with secondary decrease in pulmonary function, abdominal distention with early satiety leading to malnutrition, as well as increased mortality.2–5 For these reasons, diagnosis of VCFs, along with appropriate management, can improve health outcomes.
Compression fractures of the thoracolumbar spine typically result from a flexion-type injury. This results in a fracture of the anterior column (involving the anterior vertebral body and anterior longitudinal ligament), most commonly with a wedge-type appearance (▶Fig. 4.1). The primary symptom of a compression fracture is pain in the area of the fracture and pain with movement or transition from one position to another. Neurologic deficits are very unusual in patients with osteoporotic VCFs. The transitional pain usually manifests itself when patients go from a sitting to standing position or from a lying to sitting position and VCF-related pain also often causes difficulty with standing and walking.6
As mentioned earlier, these fractures occur when the compressive strength of the vertebral body is insufficient to tolerate the axial load applied to the vertebral body. In patients with osteoporosis or severe osteoporosis, even minor trauma such as a vigorous cough or sneeze, or even turning over in bed can cause a fracture. In fact, it has been reported that approximately 30% of vertebral fractures in severely osteoporotic patients occur when the patient is in bed.7,8 It has been hypothesized that the load in these cases results from paraspinal muscle contraction.9–11 In patients with only moderate weakening of the vertebral body usually from osteoporosis, fractures typically occur with activities such as lifting, pulling, stepping down from an elevated height, or falling. In the absence of osteoporosis, a severe axial load is typically required for fracture, typically as a result of a motor vehicle collision or a fall from substantial height. When compression fractures occur in patients younger than 55 years, or in an isolated vertebral body where fractures are uncommon (L5 or above T5), neoplastic involvement must be ruled out.12
Fig. 4.1 Lateral conventional radiograph of the thoracic spine shows a wedge-type vertebral compression fracture of the T7 vertebral body (black arrow).
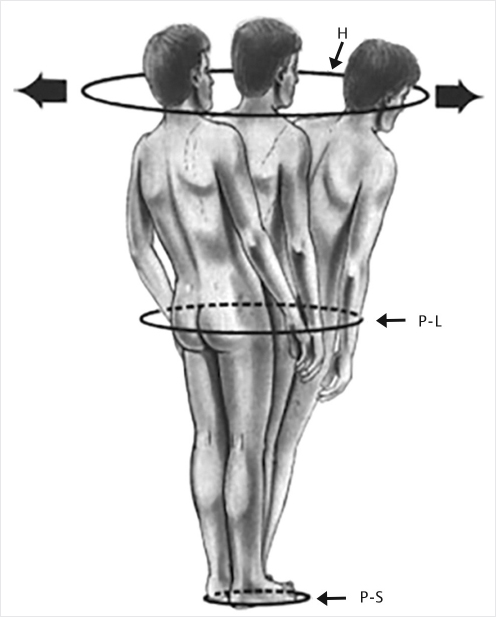
Fig. 4.2 The cone of economy. The figure outlines the “stable” zone surrounding the individual that is conical in shape from the feet to the head. Deviation from the center within the zone results in greater muscular effort and energy expenditure to maintain an upright posture. Deviation of the body outside the cone results in falling or requiring support. H, head; P-L, pelvic level; P-S, polygon of sustentation.
VCFs are not always painful and are commonly detected only incidentally on imaging for other reasons. On occasion, multiple compression fractures can result in a kyphotic deformity, which impacts the sagittal balance of the patient, causing them to fall outside of the cone of economy (▶Fig. 4.2).13 When this occurs, patients experience fatigue and pain resulting from biomechanical stresses and paraspinal spasm as a result of the increased work required to maintain an erect posture.14
Table 4.1 Risk factors of vertebral compression fractures16–19
Modifiable |
Nonmodifiable |
Osteoporosis |
History of prior compression fracture |
Smoking (tobacco use) |
Age (>55 y) |
Alcohol consumption |
Female gender |
Inadequate physical activity |
Race (Caucasian, Asian) |
Low body weight |
History of fractures in adulthood |
Impaired eyesight |
History of compression fractures in first-degree relative |
Frailty |
Dementia |
Dietary calcium deficiency |
Susceptibility to falling |
Dietary vitamin D deficiency |
|
Estrogen deficiency |
|
Early menopause |
|
Bilateral salpingo-oophorectomy |
|
Postmenopausal amenorrhea for more than 1 y |
|
Certain health conditions increase the risk of VCF. Osteoporosis is the biggest risk factor. In fact, if bone mineral density is decreased by 2 standard deviations, then fracture risk is increased by four to six times.15 Of the remaining risk factors, many are also risk factors for osteoporosis. Certain risk factors represent activities and behaviors that the patient has control over and are therefore modifiable (▶Table 4.1). These include alcohol consumption, smoking, estrogen deficiency, frailty, low body weight, insufficient physical activity, dietary calcium deficiency, and dietary vitamin D deficiency. Nonmodifiable risk factors (▶Table 4.1) include advanced age, race (Caucasian or Asian), female gender, susceptibility of falling, history of fractures in adulthood, first-generation family history of fractures, and previous steroid treatment.16–19
Certain other historical features are also predictive of new compression fractures. The biggest is a history of prior compression fracture, which has been shown to result in a fivefold increase in the risk of a new compression fracture.20,21 In addition, patients with a history of two prior compression fractures have shown a 12-fold increase in fracture risk and patients with three or more vertebral fractures have a 75-fold increased risk of additional vertebral fractures.19–21 These new fractures are most likely to be adjacent to or near the prior fractures and are most common in the mid-thoracic or thoracolumbar area.22
Primary care physicians are frequently taught in training to identify “red flag” conditions to assess the need for advanced imaging in patients presenting with back pain. There have been a number of studies looking at these red flags23–33 in patients with back pain. While these findings are similar to risk factors for osteoporotic compression fractures, the presence or absence of certain factors has been used to direct care. The most common red flags associated with compression fracture are the following: advanced age (>70), female gender, night pain, low bone mineral density, recent weight loss, immunosuppression, chronic steroid use, and history of trauma.
Fig. 4.3 A 76-year-old woman who had a T8 fracture 14 days before the examination. (a) Images showing the patient while trying to take a supine position, (b) lying on the left flank, (c) standing up to sit, and (d) almost seated. (Reproduced with permission of Postacchini R, Paolino M, Faraglia S, Cinotti G, Postacchini F. Assessment of patient’s pain-related behavior at physical examination may allow diagnosis of recent osteoporotic vertebral fracture. Spine J 2013;13:1126–1133.)
There are few studies evaluating patients who have a fracture and what findings are evident on physical examination. Postacchini et al34 evaluated pain-related behavior to determine if there were certain behavioral features that were prognostic of the presence of a painful compression fracture. In this study, patients with back pain were recorded on video and asked to take six consecutive positions on the examination table: to sit on the edge of the bed, to lie supine, to turn on the flank, to take the prone position, to turn again on the flank, and then to sit on the edge of the bed again. The evaluators then used six parameters to evaluate the patient’s behavior: grimacing, sighing, clenching or blocking their eyelids, gaping or strongly tightening their lips, asking for help by the examiner to take positions, and refusal, or extreme difficulty in turning to the prone position. In this study, they found that demonstration of at least two out of six pain behaviors while performing the six consecutive position changes was highly sensitive and specific for the presence of a VCF (▶Fig. 4.3).
Langdon et al35 evaluated two physical examination findings to determine if they were helpful in diagnosing the presence of an acute compression fracture. The first sign was the closed-fist percussion sign in which the examiner percusses the length of the spine while examining the patient’s face in a mirror. The test is positive when the patient complains of severe or sharp pain. In this series of 83 patients, closed-fist percussion had a sensitivity of 88% and a specificity of 90%. Additionally, Langdon et al evaluated the ability (or inability) of the patient to lie supine on the examination table. The test was positive when the patient was unable to lie on the table because of severe pain. This test showed a sensitivity of 81% and a specificity of 93%.
[1] Phillips FM. Minimally invasive treatments of osteoporotic vertebral compression fractures. Spine 2003;28(15, Suppl):S45–S53
[2] Leech JA, Dulberg C, Kellie S, Pattee L, Gay J. Relationship of lung function to severity of osteoporosis in women. Am Rev Respir Dis 1990;141(1):68–71
[3] Lyles KW, Gold DT, Shipp KM, Pieper CF, Martinez S, Mulhausen PL. Association of osteoporotic vertebral compression fractures with impaired functional status. Am J Med 1993;94(6):595–601
[4] Schlaich C, Minne HW, Bruckner T, et al. Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int 1998;8(3):261–267
[5] Leidig-Bruckner G, Minne HW, Schlaich C, et al. Clinical grading of spinal osteoporosis: quality of life components and spinal deformity in women with chronic low back pain and women with vertebral osteoporosis. J Bone Miner Res 1997;12(4):663–675
[6] Lad SP, Patil CG, Lad EM, Boakye M. Trends in pathological vertebral fractures in the United States: 1993 to 2004. J Neurosurg Spine 2007;7(3):305–310
[7] Bostrom MP, Lane JM. Future directions. Augmentation of osteoporotic vertebral bodies. Spine 1997;22(24, Suppl):38S–42S
[8] Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 2001;26(14):1511–1515
[9] Kim DH, Vaccaro AR. Osteoporotic compression fractures of the spine; current options and considerations for treatment. Spine J 2006;6(5):479–487
[10] Leblanc AD, Schneider VS, Evans HJ, Engelbretson DA, Krebs JM. Bone mineral loss and recovery after 17 weeks of bed rest. J Bone Miner Res 1990;5(8): 843–850
[11] Shen MS, Kim YH. Vertebroplasty and kyphoplasty: treatment techniques for managing osteoporotic vertebral compression fractures. Bull NYU Hosp Jt Dis 2006;64(3–4):106–113
[12] Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine 2001;26(14):1631–1638
[13] Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine 2010;35(25):2224–2231
[14] Wu SS, Lachmann E, Nagler W. Current medical, rehabilitation, and surgical management of vertebral compression fractures. J Womens Health (Larchmt) 2003;12(1):17–26
[15] Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 1996;312(7041):1254–1259
[16] Alexandru D, So W. Evaluation and management of vertebral compression fractures. Perm J 2012;16(4):46–51
[17] Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002;359(9319):1761–1767
[18] Lindsay R, Burge RT, Strauss DM. One year outcomes and costs following a vertebral fracture. Osteoporos Int 2005;16(1):78–85
[19] Meunier PJ, Delmas PD, Eastell R, et al; International Committee for Osteoporosis Clinical Guidelines. Diagnosis and management of osteoporosis in postmenopausal women: clinical guidelines. Clin Ther 1999;21(6):1025–1044
[20] Lindsay R, Silverman SL, Cooper C, et al. Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285(3):320–323
[21] Ross PD, Davis JW, Epstein RS, Wasnich RD. Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114(11):919–923
[22] Melton LJ III, Kallmes DF. Epidemiology of vertebral fractures: implications for vertebral augmentation. Acad Radiol 2006;13(5):538–545
[23] Downie A, Williams CM, Henschke N, et al. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ 2013;347:f7095
[24] Downie A, Williams CM, Henschke N, et al. Red flags to screen for malignancy and fracture in patients with low back pain. Br J Sports Med 2014;48(20):1518
[25] Enthoven WT, Geuze J, Scheele J, et al. Prevalence and “red flags” regarding specified causes of back pain in older adults presenting in general practice. Phys Ther 2016;96(3):305–312
[26] Ferrari R. Imaging studies in patients with spinal pain: practice audit evaluation of Choosing Wisely Canada recommendations. Can Fam Physician 2016;62(3):e129–e137
[27] Greene G. “Red flags”: essential factors in recognizing serious spinal pathology. Man Ther 2001;6(4):253–255
[28] Henschke N, Maher CG, Refshauge KM. A systematic review identifies five “red flags” to screen for vertebral fracture in patients with low back pain. J Clin Epidemiol 2008;61(2):110–118
[29] Henschke N, Maher CG, Refshauge KM, et al. Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain. Arthritis Rheum 2009;60(10):3072–3080
[30] Premkumar A, Godfrey W, Gottschalk MB, Boden SD. Red flags for low back pain are not always really red: a prospective evaluation of the clinical utility of commonly used screening questions for low back pain. J Bone Joint Surg Am 2018;100(5):368–374
[31] Underwood M, Buchbinder R. Red flags for back pain. BMJ 2013;347:f7432
[32] Verhagen AP, Downie A, Popal N, Maher C, Koes BW. Red flags presented in current low back pain guidelines: a review. Eur Spine J 2016;25(9): 2788–2802
[33] Williams CM, Henschke N, Maher CG, et al. Red flags to screen for vertebral fracture in patients presenting with low-back pain. Cochrane Database Syst Rev 2013(1):CD008643
[34] Postacchini R, Paolino M, Faraglia S, Cinotti G, Postacchini F. Assessment of patient’s pain-related behavior at physical examination may allow diagnosis of recent osteoporotic vertebral fracture. Spine J 2013;13(9):1126–1133
[35] Langdon J, Way A, Heaton S, Bernard J, Molloy S. Vertebral compression fractures--new clinical signs to aid diagnosis. Ann R Coll Surg Engl 2010; 92(2):163–166