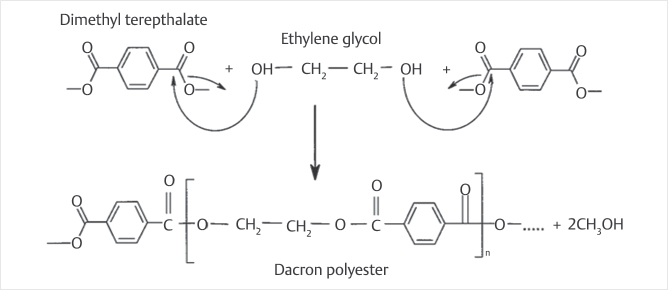
Fig. 7.1 Polymerization of Dacron polyester via a condensation reaction of dimethyl terephthalate and ethylene glycol. Note that methanol is released as a byproduct of the reaction.9
Summary
Bone cement or polymethyl methacrylate (PMMA) is the primary stabilizing material used for treating painful vertebral compression fractures (VCFs). The PMMAs available are acrylic polymers comprised of different components that can be manipulated to maximize its utility in minimally invasive spine interventions. In addition to PMMA, there is also another cement type comprised of self-hardening calcium phosphate cements (CPCs) that have been used to treat VCFs. Unlike PMMA that hardens by a polymerization process converting methylmethacrylate (MMA) monomers to PMMA, CPCs dissolve with water into a paste that hardens at body temperature into hydroxyapatite (HA). The advantage of CPCs are that they are biocompatible and are resorbed over time but the disadvantages compared to PMMA is that they are difficult to inject, are weaker than PMMA, and are often too brittle to be used in high stress areas. Fill materials also include a glass ceramic tri-resin polymer that is hydrophilic, has lower exothermic temperatures, and mimics the mechanical properties of bone. While the hydrophilic properties result in a greater amount of interdigitation into the bone and less material injected, it tends to extravasate more easily than the hydrophobic cements. Cement properties can be tailored to the appropriate use by varying the cement ingredients and can have other added components such as antibiotics and other radiopacifying agents. The future of bone cements is likely with the addition of bioactive materials such as bioactive glass, bone morphogenic protein, platelet rich plasma, stem cells, and various growth factors to promote the osteogenic activity of the native bone and to improve the strength of the cement and its degree of bony incorporation.
Keywords: bone cement, polymethyl methacrylate, vertebral augmentation, osteogenic, calcium phosphate cement, vertebroplasty, kyphoplasty
Advances in image-guided therapy for vertebral fractures and other bone-related disorders have made acrylic bone cement an integral part of the interventional tool kit. This chapter focuses on the chemistry of bone cement polymerization and the properties of components in PMMA based polymers, the most commonly used bone cements in interventional procedures such as percutaneous vertebroplasty (PVP) or vertebral augmentation. The effects of altering the concentration of the components such as MMA monomers, PMMA beads, benzoyl peroxide (BPO) activator, N,N-dimethyl-p-toluidine (DMPT) initiator, and radiopacifiers on the setting time, viscosity, polymerization temperature, and compressive strength of the cement are also considered. This information allows us to manipulate bone cement characteristics for specific applications and maximize the clinical potential of image-guided interventions. Most commercial cement kits used by radiologists were originally designed for joint replacement surgery, not vertebral fracture therapy. Novel applications such as VP require modifications of standard bone–cement mixtures—adjustments that can be made only by understanding the underlying chemical and material properties of these compounds. Our discussion will focus on the theoretical and practical aspects of polymerization chemistry, the basis for most bone cement solidification.
There are two main types of bone cements: polymers and self-hardening CPCs. Both types are fillers that stabilize joint implants or fractures, but neither is adhesive. Polymers are most commonly used because of their proven track record of safety and efficacy. They are based on the polymerization of MMA monomers to polymethyl methacrylate (PMMA), a compound better known by the name Plexiglas. Unlike polymers, the first CPCs were developed in the late 1980s to remineralize early dental carries and were approved by the Food and Drug Administration for repairing cranial defects in 1996 as cavity void fillers.
The CPCs are potentially an ideal filling material for VP and balloon kyphoplasty (BKP) applications. CPCs function by a completely different chemical mechanism based on the solubility of reactants and products. Despite the large number of calcium phosphate (CaP) combinations in different CPC systems, the setting chemistry is similar and involves dissolution and reprecipitation. Based on the nature of the end hydration product, which depends on the pH of the cement paste, Ca PO4 cements can be divided into two categories: apatite (HA) or calcium-deficient hydroxyapatite [CDHA], formed at pH > 4.2) and brushite (dicalcium phosphate dehydrate [DCPD]). Due to the short setting time, low mechanical strength, and inferior injection characteristics, brushite cements only have limited clinical applications. When tetracalcium phosphate and dicalcium phosphate are mixed with water into a paste, HA (the major mineral found in normal teeth) is rapidly formed and precipitates out of the solution, forming a hard mass at body temperature.1,2 HA is a biocompatible material believed to be gradually replaced in vivo by new bone with no loss of volume.3,4 On the downside, the cement is difficult to inject against high backpressure, and the bone resorption properties may actually cause long-term weakening in patients with osteoporosis. Additionally, it may be weaker than polymer cement5 and too brittle to be used for load-bearing applications. Because there are no long-term data for CPC technology, this review will focus on PMMA bone cements.
The use of HA and CaP bone cements in an osteoporotic patient without the addition of anabolic parathyroid (PTH) analog medication is probably not a sound concept. The addition of systemic PTH allows bone activation and anabolic bone stimulation to integrate these cements in a way that the inert elderly osteoporotic cannot achieve otherwise.
Cortoss is a glass ceramic combeite tri-resin polymer, an injectable, synthetic, nonresorbable biomaterial that mimics the mechanical properties of cortical bone.1 Cortoss has been clinically proven to match the safety and effectiveness of PMMA for VP and clinical trials with Cortoss report a low incidence of adjacent fractures,2 lower exothermic temperatures, and less monomer release than PMMA. The safety and efficacy of Cortoss has been demonstrated in three U.S. clinical investigations and multiple European studies.6,7 In patients with a first-time fracture at one level, there was a 43% reduction in adjacent-level fractures in the patient population that used Cortoss.6 Compared to PMMA, Cortoss is more hydrophilic, which enables it to coat and augment the internal structure of the vertebral body. This interdigitating characteristic resulted in a 30% reduction in material injected when compared to PMMA in a controlled study. Despite the optimal characteristics allowing the interdigitation of Cortoss within the cancellous vertebral body bone, the hydrophilic properties of the fill material make it prone to extravasation outside the vertebral body.
Before the specifics of bone cement are discussed, we will briefly review polymer chemistry. Polymers are large molecules composed of individual repeating units (monomers). Proteins are classic examples of biologic polymers composed of smaller amino acid units.
Polymerization can occur by two different mechanisms: (1) in condensation reactions, a functional group on the monomer reacts with a functional group on the growing end of the polymer, lengthening the chain and releasing an extraneous molecule (▶Fig. 7.1)8 and (2) in addition reactions, the polymer chain grows by reacting directly with the double bond of a monomer and no extraneous molecules are created (▶Fig. 7.2).
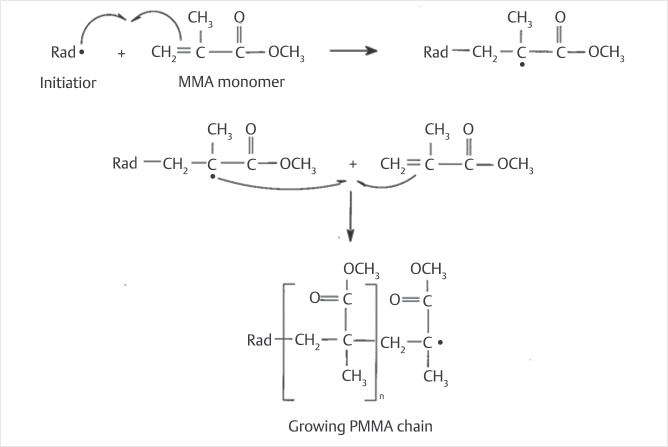
Polymerization begins by the addition mechanism in which a monomer becomes unstable by reacting with an initiator, a volatile molecule that is most commonly a radical (molecules that contain a single unpaired electron). Radicals bond with monomers, forming monomer radicals that can attack the double bond of the next monomer by the mechanism shown in ▶Fig. 7.2, propagating the polymer chain.
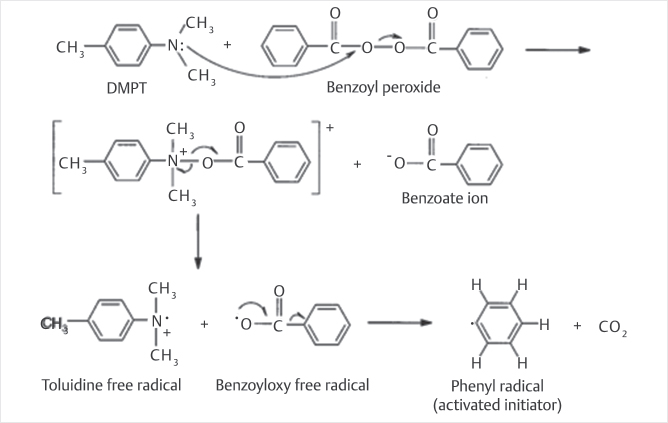
Because radicals are so transient, initiators are often added in the form of an unreactive peroxide form that is stable in solution. Radicals are formed when heat or light cleaves the peroxide molecule. For applications in which high temperatures are not practical (such as the use of bone cement in vivo), peroxide is cleaved by adding a chemical activator such as N, N-dimethyl-p-toluidine (DMPT; ▶Fig. 7.3).9
Fig. 7.1 Polymerization of Dacron polyester via a condensation reaction of dimethyl terephthalate and ethylene glycol. Note that methanol is released as a byproduct of the reaction.9
Fig. 7.2 Polymerization of polymethyl methacrylate (PMMA) by an addition reaction. Note that the methylmethacrylate (MMA) monomer reacts with a radical to form a secondary radical that can attack the double bond of another MMA monomer.
Fig. 7.3 Formation of phenyl radical by reaction of N,N-dimethyl-p-toluidine (DMPT) with the benzoyl peroxide (BPO) initiator. The phenyl radical goes on to react with methylmethacrylate (MMA) by the mechanism shown in ▶Fig. 7.2.
Table 7.1 Components of commercially available cement mixtures1
Powder |
• PMMA beads • Benzoyl peroxide (BPO) • Radiopacifier |
Liquid |
• MMA monomers • Activator (DMPT) • Hydroquinone 15–75 ppm |
Abbreviations: DMPT, N,N-dimethyl-p-toluidine; MMA, methylmethacrylate; PMMA, polymethyl methacrylate. |
Bone cements polymerize by radical-initiated addition reactions. Most commercially available cements have two separate components (▶Table 7.1): a powder containing prepolymerized beads of PMMA (or PMMA/styrene copolymer) and a liquid containing MMA monomer. The BPO initiator is incorporated into the powder and the chemical activator (i.e., DMPT) is incorporated into the liquid, so peroxide cleavage and polymerization begin only when the two are mixed. To prevent spontaneous polymerization during storage, the easily oxidized molecule hydroquinone is also added to the liquid. The DMPT cleaves BPO initiator at room temperature, forming a phenyl radical (▶Fig. 7.3) that attacks the double bond of the MMA monomer by the mechanism shown in ▶Fig. 7.2. The growing polymer chains encapsulate the PMMA beads within a solid matrix.
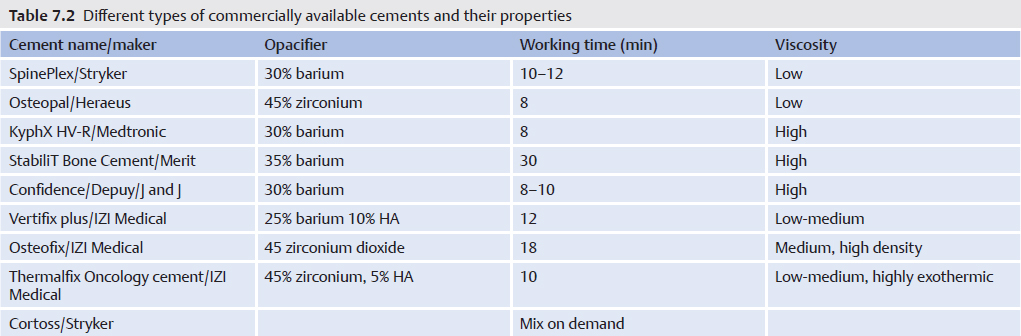
Cement is made radiopaque by adding barium sulfate or zirconium dioxide compounds to the powder (▶Table 7.2).
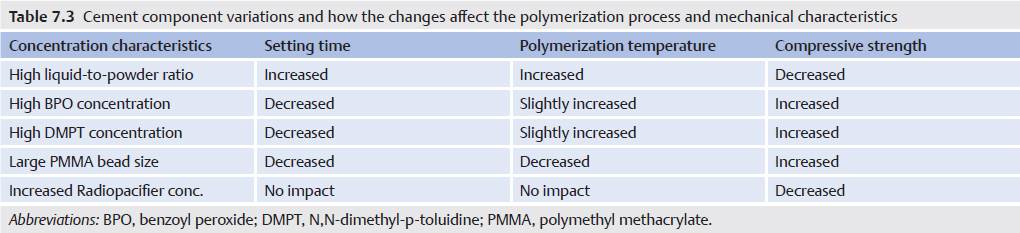
To design cements with predictable intraoperative and postoperative behavior, we must understand how cement formulation affects the polymerization and material properties of the solid. Like any heterogeneous mixture, the characteristics of the whole differ markedly from those of its components. For example, one cannot calculate a priori the porosity and strength of building mortar based solely on the properties of its various pebbles and finely ground minerals. These individual particles form a complex intermolecular network whose characteristics can be identified only empirically. The effect of each component on the setting time, polymerization temperature, and material properties of bone cement is detailed in the following sections.
Polymerization temperature and setting time can be studied by altering liquid-to-powder (L/P) ratios. Clinically, these are key properties to control. Predictable setting time is critical intraoperatively to prevent solidification before completion of the procedure. High polymerization temperatures are known to cause tissue necrosis and hinder the efficacy of joint prostheses.1 In spite of adverse effects of cement heat in some situations, highly exothermic cements can be preferentially used in a patient with malignant disease and pathologic compression fractures to achieve local tumor kill. Exofix is a cement that polymerizes to 88°C and was designed specifically for this purpose. Early research showed that greater L/P ratios produce higher peak temperatures but increase setting time. One hypothesis was that, at high L/P ratios, an abundance of monomers react exothermically, increasing the peak polymerization temperature. However, the high L/P ratio also decreases the relative concentration of the initiator (a component of the powder), so the monomers are activated slowly, increasing setting time.10,11 Clearly, studies that vary monomer-topolymer ratios independently of other cement components are needed (▶Table 7.3).
Altering the BPO-to-DMPT ratio has a significant effect on setting time, polymerization temperature, and strength (▶Table 7.3). Unfortunately, strength and setting time are inversely related. Adjusting BPO and DMPT concentrations to maximize setting time reduces overall strength.9,12
The rate of radical formation is dependent on the concentrations of the activator (i.e., DMPT) and peroxide. Faster radical formation activates more monomers that act as nucleation sites for polymer chain growth. This has a number of downstream effects. First, this will speed up the overall polymerization process, decreasing setting time. Second, more nucleation sites imply that more individual polymer chains will form simultaneously. This will reduce the average molecular weight of each polymer chain and affect overall strength and tensile properties of the cement.
To determine the proper initiator/activator (i.e., BPO-to-DMPT) ratio, a system that uses two liquid solutions was developed. Use of two-part liquid solutions rather than conventional liquid/powder cements allows for better mixing and consistency among experimental samples and reduces porosity caused by the trapping of air while mixing liquid/powder cements. These air pockets act as fracture initiation sites that compromise the strength of the cement. Both parts contained dissolved PMMA powder and MMA monomers in a 4:5 ratio. BPO was added to the first solution and DMPT to the second. Samples with varying concentrations of BPO and DMPT were prepared for comparative testing.
Although BPO and DMPT concentrations had profound effects on setting time, the impact on polymerization temperature is unclear. Increasing the concentration of BPO from 0.5 g per 100-mL MMA to 2.75 g per 100-mL MMA (at a constant DMPT concentration of 0.2 mL per 100-mL MMA) decreased setting time from 28.30 (± 3.34) to 9.26 minutes (± 0.97). Similarly, increasing DMPT concentration from 0.2 mL per 100-mL MMA to 4.9 mL per 100-mL MMA (at a constant BPO concentration of 0.5 g per 100-mL MMA) decreased setting time from 28.20 (± 3.34) to 5.50 minutes (± 0.17). No statistically significant changes in polymerization temperature were observed in these experiments.
Pascual et al13 reported conflicting results with use of the more conventional liquid/powder cement mix. Although boosting BPO concentration from 0.75 to 2.0% decreased setting time by 20%, polymerization temperature increased an average of 3 to 6°C. When DMPT was doubled from 1.0 to 2.0% and BPO increased from 0.75 to 2.0%, temperatures increased an average of 10°C.
Mechanical properties were also strongly related to BPO and DMPT concentrations. As the concentrations of BPO and DMPT increased, the mechanical strength of the cement cores also increased. Cements with the lowest concentrations of BPO (0.5 g per 100-mL MMA) and DMPT (0.2 mL per 100-mL MMA) were significantly weaker than other cements. At every BPO concentration, peak strength occurred at a DMPT concentration of 1.4 mL per 100-mL MMA. The maximum value (105–110 MPa) was achieved at a BPO-to-DMPT ratio of approximately 1:1. In a measure of durability, compounds containing 2.0 g BPO and 1.4 mL DMPT withstood more cycles of stress loading before structural failure than samples containing 2.0 g BPO and 4.9 mL DMPT.12 Optimizing the BPO-to-DMPT ratio for cement strength decreases setting time and may increase polymerization temperature.
Radiopacifiers such as barium sulfate and zirconium dioxide are present in standard bone cement mixes at low concentrations. Additional opacifiers are often added for interventional procedures such as VP, in which visibility is key. These heavy metals interrupt the polymerizing matrix and produce pores that can act as fracture initiation sites, diminishing overall cement strength with an unclear effect on polymerization temperature and setting time.14,15 Adding 10% barium sulfate to Simplex P cement decreased tensile strength and fracture toughness by 10%. As the percentage of barium in samples of Cranioplastic cement increased from 0 to 12.5%, tensile strength decreased 10%, strain to failure (ability to compress before being destroyed) decreased by one-third, and the Young modulus (stress/strain, a measure of stiffness) increased 20%.15
The effect of metal radiopacifiers on cement fatigue is less clear. Dynamic fatigue refers to the behavior of materials under repeated loads over time and is measured by applying a cyclic load with constant amplitude and measuring the number of cycles until failure.16 This is an important property for cement used in procedures such as VP in which vertebral bodies will be subjected to repeated loading and unloading of forces over a period of years. Although a number of studies have shown that barium decreases fatigue strength17 and increases crack growth rate,18 others report lower rates of fatigue crack growth with radiopaque cement.19 This discrepancy may be caused by the fact that the latter study was performed in water to simulate an in vivo environment, whereas the other studies tested cement samples in air.
Clinicians can enhance the structural integrity of radiopacified cement in a number of ways. First, there are indications that zirconium is superior to barium structurally and may be the agent of choice.15,20 Second, homogeneity of mixed cement is key; failure to disperse barium particles evenly leads to fracture formation.21 Third, new cross-linking agents and preparation methods that enhance cement strength have been reported.15,22 Incorporating these concepts into cement formulations will minimize any loss of strength or durability from radiopacifiers.
The average diameter and size distribution of PMMA beads play an important role in the cure properties of bone cement. Aside from its structural role as a component of the cement matrix, PMMA beads serve as a heat sink—dissipating energy released by the exothermic polymerization of MMA monomers. Samples containing PMMA particles with larger mean diameters and widespread distributions of particle size had lower peak polymerization temperatures and longer setting times.13,23 As particle diameter increased from 33 to 65 m and size range spread from 10 to 60 m to 10 to 140 m, peak polymerization temperature decreased from approximately 88 to 62°C and setting time doubled to 10 minutes.13
Structurally, bead size and distribution has less impact. Although an increase from 33 to 55 m did cause compressive strength to increase from 128 to 149 MPa with 1% DMPT and from 103 to 152 MPa with 2% DMPT, other parameters including elastic modulus and tensile strength were unaffected.16 Creep resistance, a measure of the ability to withstand a load, increased when larger PMMA particles were used and when larger MMA/styrene copolymer beads were substituted for PMMA beads.24 For this reason, many brands of commercial cement contain a large percentage of MMA/styrene copolymer in cement powder.
Therefore, use of PMMA beads with a larger mean diameter and wider size distribution has a number of beneficial effects. Unlike the BPO-to-DMPT ratio, proper bead size allows maximization of setting time and decrease of polymerization temperature without diminished cement strength.
Aside from intrinsic factors related to composition, extrinsic factors such as mixing method have a large impact on cement properties. Depending on mixing technique, air may become trapped in the cement mixture, increasing porosity. Air weakens the cement and provides an interface for fractures and cracks to develop. Although the two-solution cement discussed earlier is effective at decreasing porosity, almost all commercially available cement requires mixing powder and liquid. For these situations, vacuum mixing devices have been shown to reduce porosity by more than 44% compared with mixing with a bowl and spatula. Centrifugation may also be an effective method for limiting porosity. Cement cores manufactured by centrifuging the powder/monomer mixture had increased fatigue life with greater consistency among different samples than cores created with use of the bowl and spatula mixing technique.25 Consistent preparation methods will ensure uniform results and prevent uneven mixtures with variable mechanical properties.
Antibiotics are sometimes added to the cement powder before injection to minimize infection.26,27 These additives, like barium sulfate and zirconium dioxide, can affect the mechanical properties of the bone cement. Research has shown that adding various types of antibiotics to bone cement, in quantities less than 2 g per standard packet of bone cement, does not adversely affect some of the cement’s mechanical properties (compressive or diametrical tensile strengths), although quantities exceeding 2 g did weaken them.28,29 These findings were substantiated by another report that showed the addition of 0.5 g of erythromycin and 0.24 g of colistin to Simplex P was not detrimental to the cement’s fatigue properties.30
As with other additives, the addition of antibiotics to the cement has produced conflicting results. In one study, the addition of 2 g of powdered gentamicin, oxacillin, or cefazolin to 60 g of Simplex P or Palacos produced no statistically significant difference in terms of short-term (<40 days) compressive and tensile strengths compared with the cement without powdered antibiotics.31 However, another study found a significant decrease in mechanical strength between cements mixed with 250 or 500 mg of gentamicin in 6.25 or 12.5 mL of water and cements without aqueous antibiotics.29 Although these reports showed no deleterious mechanical effects from the addition of powdered antibiotics, provided the quantity was less than 2 g, other investigators have reported that compression strength was compromised by the addition of 2 g of antibiotics (gentamicin or Keflin) per 60 g of Simplex P.32
One alternative, already used by some physicians performing VP or kyphoplasty, is the intravenous administration of antibiotics before vertebral augmentation,33 which avoids the risk of potential changes to the cement’s properties.
Thermal necrosis of surrounding nerves was previously postulated as a mechanism of pain relief in VP. Research in laboratory animals indicates that thermal necrosis of bone tissue occurs when temperatures surpass 50°C for more than 1 minute.34
Deramond et al35 measured temperatures at the anterior cortices, centers, and spinal canals of cadaveric vertebral bodies after bipedicular injections of Simplex P or Orthocomp (bisphenol glycidyl dimethacrylate/bisphenol ethoxy dimethacrylate/triethylene glycol dimethacrylate, a matrix composite cement reinforced with glass-ceramic), both of which were prepared according to the manufacturer’s specifications. They found that, at the central location, Simplex P injection was associated with significantly higher temperatures and with temperatures exceeding 50°C for significantly longer times (61.8°C) than Orthocomp injection (51.2°C).35 However, measurements at the anterior cortex and spinal canal locations showed no significant difference between the two cements. In fact, at the latter location, the temperature of cement did not exceed 41°C in either cement. The authors hypothesized that, given their results, it was unlikely the pain relief from VP was caused by intraosseous neural tissue damage.35
There is also additional evidence that pain relief from vertebral augmentation is provided by the reestablishment of the mechanical stability of the vertebral body rather than by any neurolysis of intravertebral nerves. In a kyphoplasty study with information from the Swiss registry, cement volume was a significant predictor for pain relief and the only operator modifiable variable.36 This study showed a clear dose–outcome relationship between cement filling volumes and pain relief and the authors recommended a minimum of 4.5 mL of PMMA to achieve durable pain relief.
The Investigational Device Exemption trial comparing Cortoss versus PMMA had nearly superimposable graphs showing the mean Visual Analog Scale (VAS) pain reduction for Cortoss and PMMA.6,7 Given that Cortoss has little to no exothermic reaction, it is very likely that all or most of the pain relief is caused by reestablished mechanical stability of the vertebral body.
In unpublished data from a patient cohort treated by vertebral augmentation with corticocancellous allograft bone, the mean VAS pain reduction scores decreased from 43 to 22 after osseous augmentation with allograft bone only. The amount of allograft bone injected per patient averaged 8.6 mL. This resulted in not only a pain decrease presumed to be from the increased mechanical stability but also a functional increase with the Oswestry Disability Index decreasing from 40 to 21.37
Conventional PMMA cements cannot adhere to existing bone,38 but this disadvantage may not be as pertinent for VP as for arthroplasty. Because the cement is injected directly into the bone, and not used as an adhesive agent as in arthroplasty, cement loosening may not cause any noticeable problems. Results of one study indicated that, at long-term follow-up (average, 1.3 years) after VP with PMMA cements, the vertebrae were stable with respect to compression and the degree of kyphosis.39 Only 1 of 20 vertebral levels showed signs of cement compression; the remaining 19 showed no change in cement morphology.40 Another follow-up study (48 months after the procedure) showed no progression of vertebral deformity after VP.38 However, if the cement loosens to such a degree that it compromises the structural integrity of the vertebral body, refracture of the vertebral body can occur around the injected cement.40
Although research has shown that PMMA cements cannot induce new bone formation,38 some new bone cements show promise not only in terms of bone growth but also in terms of improved physical and mechanical properties, which could be beneficial for PVP. One recently developed cement consists of bioactive glass beads and a novel organic matrix of PMMA, which resulted in new bone formation around the beads and a significant increase in bending strength compared with PMMA cement without the beads.40 Curing time and polymerization temperatures were not reported. Adding a glass-ceramic powder and bisphenol-a-glycidyl methacrylate (bis-GMA) resin to a PMMA-based cement has produced a bioactive acrylic bone cement that bonds directly to the bone after 4 to 8 weeks in vivo and has faster hardening times, lower curing temperatures, and significantly better physical properties.41 In one study, investigators measured the stiffness and strength of fresh cadaveric thoracic and lumbar vertebrae injected with BoneSource (an HA bioactive bone cement) or Cranioplastic (a PMMA-based product) and then mechanically compressed.42 The vertebrae injected with Cranioplastic had significantly greater strength compared with strength in the prefractured state, whereas those injected with BoneSource regained initial strength. However, both Cranioplastic and BoneSource resulted in a lower stiffness in all vertebrae compared with initial measurements.42 A similar comparison of Simplex P and BoneSource showed that both cements resulted in significantly less stiffness than in the precompressed states.5 However, Simplex P injections resulted in significantly greater strength compared with prefracture measurements, whereas BoneSource restored the vertebrae to their initial strength.41 Despite these findings, in vitro studies comparing HA cements and PMMA products should be conducted to determine which is more suitable for use in VP as the HA cement can show osteoconversion in the porous portions of the cement at the bone or bone–cartilaginous junction without inflammatory activity and absence of a fibrous capsule surrounding the cement.43 This may lead to a stronger bond to the native bone and increased durability over time.
Simplex P and Orthocomp were studied with respect to their ability to restore strength and stiffness of the vertebral body.44 After initial measurements of strength and stiffness were made, mechanical compression was applied to osteoporotic cadaveric vertebral bodies posterior to the anterior wall.45 Vertebrae were then injected with Simplex P or Orthocomp and retested to determine their augmented strength and stiffness. Injection with Simplex P or Orthocomp significantly increased vertebral body strength compared with the initial measurements. Initial vertebral body stiffness was restored by using Orthocomp, but vertebral bodies augmented with Simplex P were significantly less stiff than in their precrush condition.46
Similar studies have compared a PMMA cement (Palacos E-Flow) to a CaP experimental brushite cement (EBC) with respect to strength and stiffness.44 Osteoporotic vertebral bodies harvested from cadavers were measured, axially compressed, injected with either Palacos E-Flow or EBC, and then retested for strength and stiffness. Injections of PMMA and EBC increased the average stiffness (in osteoporotic vertebrae only) by 174% (range, 10–159%) and 120% (range, 108 −131%), respectively, and the average strength by 195% (range, 26–254%) and 113% (range, 104–126%), respectively. The study also showed that the cements’ augmenting effects were proportional to the degree of filling, although the correlation was weak.47
Novel work is underway with cements containing bone morphogenic protein (BMP), a protein that belongs to the transforming growth factor (TGF) superfamily and found in bone matrix.48 It is believed that BMP serves as a growth factor for adult articular cartilage matrix repair and synthesis. Although no work specific to PVP has been conducted, studies using BMP-impregnated cement implanted into bone have shown new bone or callus formation in a dose-dependent manner.48–50 Additional research is required to determine what effect, if any, BMP has on the physical properties of the bone cement and its application in PVP.
PMMA bone cements usually lack sufficient osteoinductivity. Therefore, various bioactive osteogenic agents can be added in order to promote new bone formation. The incorporation of bioactive materials has been shown to improve the biological performance of CPCs by promoting bone metabolism. Because they are porous, CPCs can be used as carrier agents for stem cells and growth factors. These growth factors can include bone morphogenetic proteins (BMPs), basic fibroblast growth factor (bFGF), and vascular endothelial growth factor (VEGF). The growth factors may be mixed with CPC components alone, or can be encapsulated within microspheres of chitosan, gelatin, or hyaluronic acid before incorporation into the CPC for best preservation of their bioactivity. Plasmids or small interfering RNAs (siRNAs) may also be incorporated into CPCs to achieve gene delivery to cells at the injection area. Recently, platelet-rich plasma (PRP), mesenchymal stem cells of umbilical origin, and autologous bone marrow concentrate have been used together with CPCs as autologous bone substitutes. Systemic subcutaneous or inhaled PTH in pulsed delivery mode has been shown in animals to augment CPC integration.
The percutaneous treatment of bone-related disorders is a fast-growing field within interventional radiology. We are beginning to expand beyond VP, performing cementoplasty of fractures and metastatic lesions in sites ranging from the acetabulum to the scapula.51
Many of these indications could take advantage of bone cements with specific attributes. Whereas cement mixtures with very high polymerization temperatures are useful for painful pelvic metastases to maximize necrosis of the tumor, treatment of vertebral or other weight-bearing fractures may, conversely, require cements that can withstand greater stress and fatigue. For procedures that have limited access or require a specific needle size, the cement viscosity and setting time are key characteristics. The theoretical principles and practical data discussed earlier identify numerous ways to perfect PMMA bone cement for different indications.
Modifying cement characteristics is only the first step toward improving patient health. Research is needed to determine which material properties are clinically relevant for each procedure. Bone cement strength may not be critical for most procedures, compared to other characteristics such as setting time and polymerization temperature. In fact, arguments could be made that weaker cements may be more beneficial for procedures such as VP. These questions would best be answered by studies and nationwide registries correlating cement formulation with long-term clinical outcomes. This would lead to the establishment of guidelines describing the safest and most effective formulations of bone cement for specific types of procedures.
Like any procedure, percutaneous treatments of bone disease such as VP are not immune to complications. Most problems are caused by the extravasation of bone cement into the spinal canal and venous system. Bone cement preparation may be one source of the problem. Cement that is too fluid or has a long setting time, for example, is more likely to escape its site of injection. By understanding the principles described in this review, these pitfalls can be avoided. Just as practitioners must understand the mechanism of action before prescribing a drug, interventional radiologists must have intimate knowledge of bone cement before injecting a compound that can be potentially fatal when used incorrectly.
• When it comes to cement injection into a vertebral body, see it like an embolization of a venous space with a liquid polymer.
• You can always do more; you can never do less.
• This is civil engineering; think of the load distribution.
• If your little voice tells you to stop the injection, stop.
• Optimistic happy patients do better.
[1] Fukase Y, Eanes ED, Takagi S, Chow LC, Brown WE. Setting reactions and compressive strengths of calcium phosphate cements. J Dent Res 1990; 69(12):1852–1856
[2] Liu C, Shen W, Gu Y, Hu L. Mechanism of the hardening process for a hydroxyapatite cement. J Biomed Mater Res 1997;35(1):75–80
[3] Ishikawa K, Takagi S, Chow LC, Suzuki K. Reaction of calcium phosphate cements with different amounts of tetracalcium phosphate and dicalcium phosphate anhydrous. J Biomed Mater Res 1999;46(4):504–510
[4] Lim THL, Brebach GT, Renner SM, et al. Biomechanical evaluation of an injectable calcium phosphate cement for vertebroplasty. Spine 2002;27(12): 1297–1302
[5] Belkoff SM, Mathis JM, Jasper LE. Ex vivo biomechanical comparison of hydroxyapatite and polymethylmethacrylate cements for use with vertebroplasty. AJNR Am J Neuroradiol 2002;23(10):1647–1651
[6] Bae H, Hatten HP Jr, Linovitz R, et al. A prospective randomized FDA-IDE trial comparing Cortoss with PMMA for vertebroplasty: a comparative effectiveness research study with 24-month follow-up. Spine 2012;37(7):544–550
[7] Palussière J, Berge J, Gangi A, et al. Clinical results of an open prospective study of a bis-GMA composite in percutaneous vertebral augmentation. Eur Spine J 2005;14(10):982–991, 18, 2016
[8] Wade LG. Synthetic polymers. In: Wade LG, ed. Organic Chemistry. 3rd ed. Princeton, NJ: Prentice Hall; 1995:1231–1246
[9] Hasenwinkel JM, Lautenschlager EP, Wixson RL, Gilbert JL. A novel high-viscosity, two-solution acrylic bone cement: effect of chemical composition on properties. J Biomed Mater Res 1999;47(1):36–45
[10] Turner RC, Atkins PE, Ackley MA, Park JB. Molecular and macroscopic properties of PMMA bone cement: free-radical generation and temperature change versus mixing ratio. J Biomed Mater Res 1981;15(3):425–432
[11] Pascual B, Gurruchaga M, Ginebra MP, Gil FJ, Planell JA, Goñi I. Influence of the modification of P/L ratio on a new formulation of acrylic bone cement. Biomaterials 1999;20(5):465–474
[12] Hasenwinkel JM, Lautenschlager EP, Wixson RL, Gilbert JL. Effect of initiation chemistry on the fracture toughness, fatigue strength, and residual monomer content of a novel high-viscosity, two-solution acrylic bone cement. J Biomed Mater Res 2002;59(3):411–421
[13] Pascual B, Vázquez B, Gurruchaga M, et al. New aspects of the effect of size and size distribution on the setting parameters and mechanical properties of acrylic bone cements. Biomaterials 1996;17(5):509–516
[14] Topoleski LD, Ducheyne P, Cuckler JM. A fractographic analysis of in vivo poly(methyl methacrylate) bone cement failure mechanisms. J Biomed Mater Res 1990;24(2):135–154
[15] De S, Vazquez B. The effect of cross-linking agents on acrylic bone cements containing radiopacifiers. Biomaterials 2001;22(15):2177–2181
[16] Soltesz U, Richter H. Mechanical behavior of selected ceramics. In: Ducheyne PD, Hastings GH, eds. Metal and Ceramic Biomaterials. Vol. II: Strength and Surface. Boca Raton, FL: CRC Press; 1984
[17] Baleani M, Cristofolini L, Minari C, Toni A. Fatigue strength of PMMA bone cement mixed with gentamicin and barium sulphate vs pure PMMA. Proc Inst Mech Eng H 2003;217(1):9–12
[18] Owen AB, Beaumont PW. Fracture behaviour of commercial surgical acrylic bone cements. J Biomed Eng 1979;1(4):277–280
[19] Molino LN, Topoleski LDT. Effect of BaSO4 on the fatigue crack propagation rate of PMMA bone cement. J Biomed Mater Res 1996;31(1):131–137
[20] Rudigier J, Draenert K, Gruenert A, Ritter G. Effects of adding x-ray contrast materials to bone cements. Akt Traumatol 1977;7:35–48
[21] Bhambri SK, Gilbertson LN. Micromechanisms of fatigue crack initiation and propagation in bone cements. J Biomed Mater Res 1995;29(2):233–237
[22] Kim HY, Yasuda HK. Improvement of fatigue properties of poly (methyl methacrylate) bone cement by means of plasma surface treatment of fillers. J Biomed Mater Res 1999;48(2):135–142
[23] Lewis G, Carroll M. Rheological properties of acrylic bone cement during curing and the role of the size of the powder particles. J Biomed Mater Res 2002;63(2):191–199
[24] Treharne RW, Brown N. Factors influencing the creep behavior of poly(methyl methacrylate) cements. J Biomed Mater Res 1975;9(4):81–88
[25] James SP, Jasty M, Davies J, Piehler H, Harris WH. A fractographic investigation of PMMA bone cement focusing on the relationship between porosity reduction and increased fatigue life. J Biomed Mater Res 1992;26(5):651–662
[26] Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol 1997;18(10):1897–1904
[27] Murphy KJ, Deramond H. Percutaneous vertebroplasty in benign and malignant disease. Neuroimaging Clin N Am 2000;10(3):535–545
[28] Lautenschlager EP, Jacobs JJ, Marshall GW, Meyer PR Jr. Mechanical properties of bone cements containing large doses of antibiotic powders. J Biomed Mater Res 1976;10(6):929–938
[29] Lautenschlager EP, Marshall GW, Marks KE, Schwartz J, Nelson CL. Mechanical strength of acrylic bone cements impregnated with antibiotics. J Biomed Mater Res 1976;10(6):837–845
[30] Davies JP, O’Connor DO, Burke DW, Harris WH. Influence of antibiotic impregnation on the fatigue life of Simplex P and Palacos R acrylic bone cements, with and without centrifugation. J Biomed Mater Res 1989;23(4):379–397
[31] Marks KE, Nelson CL, Lautenschlager EP. Antibiotic-impregnated acrylic bone cement. J Bone Joint Surg Am 1976;58(3):358–364
[32] Nelson RC, Hoffman RO, Burton TA. The effect of antibiotic additions on the mechanical properties of acrylic cement. J Biomed Mater Res 1978;12(4): 473–490
[33] Amar AP, Larsen DW, Esnaashari N, Albuquerque FC, Lavine SD, Teitelbaum GP. Percutaneous transpedicular polymethylmethacrylate vertebroplasty for the treatment of spinal compression fractures. Neurosurgery 2001;49(5):1105–1114, discussion 1114–1115
[34] Eriksson RA, Albrektsson T, Magnusson B. Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand J Plast Reconstr Surg 1984;18(3):261–268
[35] Deramond H, Wright NT, Belkoff SM. Temperature elevation caused by bone cement polymerization during vertebroplasty. [Suppl] Bone 1999;25(2, Suppl): 17S–21S
[36] Röder C, Boszczyk B, Perler G, Aghayev E, Külling F, Maestretti G. Cement volume is the most important modifiable predictor for pain relief in BKP: results from SWISSspine, a nationwide registry. Eur Spine J 2013;22(10):2241–2248
[37] Vertebral augmentation with Allograft bone: a clinical trial to assess treatment efficacy and patient response to therapy. 2007. Unpublished manuscript
[38] Freeman MAR, Bradley GW, Revell PA. Observations upon the interface between bone and polymethylmethacrylate cement. J Bone Joint Surg Br 1982;64(4):489–493
[39] Kallmes DF, Jensen ME. Percutaneous vertebroplasty. Radiology 2003; 229(1):27–36
[40] Molloy S, Mathis JM, Belkoff SM. The effect of vertebral body percentage fill on mechanical behavior during percutaneous vertebroplasty. Spine 2003;28(14):1549–1554
[41] Shinzato S, Nakamura T, Kokubo T, Kitamura Y. Bioactive bone cement: effect of silane treatment on mechanical properties and osteoconductivity. J Biomed Mater Res 2001;55(3):277–284
[42] Yamamuro T, Nakamura T, Iida H, et al. Development of bioactive bone cement and its clinical applications. Biomaterials 1998;19(16):1479–1482
[43] Kokoska MS, Friedman CD, Castellano RD, Costantino PD. Experimental facial augmentation with hydroxyapatite cement. Arch Facial Plast Surg 2004;6(5):290–294
[44] Belkoff SM, Mathis JM, Jasper LE, Deramond H. An ex vivo biomechanical evaluation of a hydroxyapatite cement for use with vertebroplasty. Spine 2001;26(14):1542–1546
[45] Grados F, Depriester C, Cayrolle G, Hardy N, Deramond H, Fardellone P. Long-term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology (Oxford) 2000;39(12):1410–1414
[46] Heini PF, Berlemann U, Kaufmann M, Lippuner K, Fankhauser C, van Landuyt P. Augmentation of mechanical properties in osteoporotic vertebral bones: a biomechanical investigation of vertebroplasty efficacy with different bone cements. Eur Spine J 2001;10(2):164–171
[47] Belkoff SM, Mathis JM, Erbe EM, Fenton DC. Biomechanical evaluation of a new bone cement for use in vertebroplasty. Spine 2000;25(9):1061–1064
[48] Alam I, Asahina I, Ohmamiuda K, Enomoto S. Comparative study of biphasic calcium phosphate ceramics impregnated with rhBMP-2 as bone substitutes. J Biomed Mater Res 2001;54(1):129–138
[49] Chubinskaya S, Kuettner KE. Regulation of osteogenic proteins by chondrocytes. Int J Biochem Cell Biol 2003;35(9):1323–1340
[50] Niedhart C, Maus U, Redmann E, Schmidt-Rohlfing B, Niethard FU, Siebert CH. Stimulation of bone formation with an in situ setting tricalcium phosphate/rhBMP-2 composite in rats. J Biomed Mater Res A 2003;65(1):17–23
[51] Dehdashti AR, Martin JB, Jean B, Rüfenacht DA. PMMA cementoplasty in symptomatic metastatic lesions of the S1 vertebral body. Cardiovasc Intervent Radiol 2000;23(3):235–237