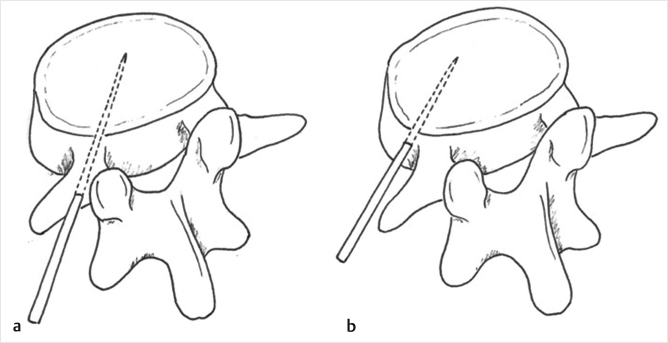
Fig. 8.1 (a, b) Vertebroplasty involves the percutaneous insertion of a needle into the vertebral body, followed by the injection of cement.
Summary
Vertebroplasty is a minimally invasive procedure that involves the injection of bone cement or other injectable fill material into vertebral compression fractures, with the aim of providing pain relief and improving functional status. Vertebroplasty is generally performed in the thoracic, lumbar, and sacral spine. Cervical vertebroplasty may also be performed but is less common. Most procedures are performed for osteoporotic vertebral compression fractures that are refractory to nonsurgical management, or for neoplasm-related fractures from metastatic disease, or multiple myeloma. Failure of nonsurgical management may be considered to have occurred when severe back pain or significantly compromised mobility persists following medical therapies, or when unacceptable adverse effects such as confusion or sedation occur with the analgesic doses required to alleviate pain. The essential equipment required for vertebroplasty includes the vertebroplasty needle system and bone cement. While multiple types of cement and osseous fill materials are commercially available, polymethyl methacrylate (PMMA) remains the most widely used. Analgesia and antibiotic prophylaxis are typically utilized for the procedure. Image guidance is vital for all vertebroplasty procedures, with fluoroscopy and/or computed tomography recommended as the imaging modalities of choice. This chapter outlines a practical guide to the procedural and the technical aspects of vertebroplasty. A description of the equipment required, fill materials utilized, considerations for performing cervical vertebroplasty, and optimal postprocedure care are discussed.
Keywords: vertebroplasty, vertebral compression fractures, bone cement, percutaneous, osteoporosis, metastasis, fluoroscopy
Vertebroplasty is a percutaneous minimally invasive, image-guided procedure that involves the injection of bone cement into a fractured vertebral body (▶Fig. 8.1). Most vertebroplasty procedures are performed for osteoporotic vertebral compression fractures (VCFs) that remain symptomatic following failure of nonsurgical management (NSM). Procedures are also performed for pathologic fractures, in particular for osteolytic metastases, multiple myeloma, or vascular tumors. Failure of NSM can be defined as persistent pain to the extent that mobility or activities of daily living are substantially compromised, or when unacceptable adverse effects, such as confusion or sedation occur due to high analgesic doses required for pain control. The goals of vertebroplasty are pain relief, improved mobility and functional status, and restoration of vertebral height and stability. Image guidance is essential for all vertebroplasty procedures, with fluoroscopy being the primary recommended method of imaging guidance due to its capacity to provide rapid image acquisition and ability to produce continuous real-time monitoring during cement injection. Vertebroplasty may also be performed using computed tomography (CT) guidance either with or without fluoroscopy or CT fluoroscopy.
This chapter will review the technical aspects of percutaneous vertebroplasty, the materials required, and suggested postprocedure care.
Vertebroplasty requires a robust understanding of spinal anatomy as viewed on fluoroscopy. In the anteroposterior (AP) projection, the vertebral body is visualized as a rectangular-shaped bone with the superior and inferior borders located adjacent to the adjacent intervertebral disks. The ovoid pedicular margins are viewed medial to the lateral margins of the vertebral body. The medial and inferior cortices of the pedicle should be noted, as these are critical landmarks for planning and maintaining a safe needle trajectory. A true AP position is obtained by aligning the spinous processes midway between the pedicles. In the true lateral projection, the end plates and posterior margin of the vertebral body are sharply defined with the ribs superimposed.1
Cement leakage outside the vertebral body can occur, although the vast majority of leaks are limited and are asymptomatic.2–4 It is important to appreciate the posterior margin of the vertebral body on the lateral view and carefully observe for posterior leakage during cement injection. Maintaining a safe margin of 3 to 5 mm from the anterior border of the vertebral body also avoids damage to key structures anterior to the vertebral body, such as the aorta, inferior vena cava, and other retroperitoneal structures. Intradiskal leakage can be visualized as the cement extends through the superior or inferior end plates of the vertebral body.
Fig. 8.1 (a, b) Vertebroplasty involves the percutaneous insertion of a needle into the vertebral body, followed by the injection of cement.
Many forms of vertebroplasty needles are commercially available. Typically, needles are hollow, straight, and range from 10 to 15 gauge in caliber. Smaller systems may be necessary in small pedicles or in the upper thoracic or cervical spine. Needle tips are available in diamond-shaped, single-beveled, or multibeveled designs. The diamond-tip needle configuration provides optimal ease of needle penetration into cortical bone. Beveled needles have superior control and maneuverability, and are useful for changing the needle direction according to which direction the bevel is oriented. Curved needle systems have been recently developed that possess the ability to arc up to 90 degrees, allowing access to sites that are difficult to reach with straight needles. Polymethyl methacrylate (PMMA) remains the most common bone cement utilized.5 The majority of vertebroplasty procedures are performed using fluoroscopic guidance. The procedure room should include equipment for patient monitoring, including electrocardiography, blood pressure and pulse oximetry, and cardiopulmonary resuscitation equipment. Patients commonly receive local anesthesia and moderate conscious sedation, as well as prophylactic antibiotics prior to the procedure. Preprocedural imaging should be available to ensure treatment of the correct vertebral levels. In the rare event of symptomatic complications during the procedure, it is important to have rapid availability of CT and magnetic resonance imaging (MRI) facilities. Modern fluoroscopic units may also have on-table cone beam CT functionality that can be useful in large or obese patients where fluoroscopic landmarks may be difficult to identify or where intraprocedural complications are suspected.
Analgesia is necessary for all vertebroplasty procedures. For the majority of patients, this is achieved by using a combination of local anesthetics (e.g., lidocaine and bupivacaine) and moderate conscious sedation (e.g., intravenous fentanyl and midazolam). The skin, subcutaneous tissues, and periosteum along the needle tract and at the bone entry point should be thoroughly infiltrated with local anesthetic to minimize pain. Some mild discomfort may be expected as the needle traverses periosteum during the initial cortical penetration. Additional discomfort may occur when the PMMA is injected; in these cases, additional intravenous analgesics may be required. The advantage of conscious sedation is it allows feedback from the patient, such as worsening pain or neurologic dysfunction, which may alert the operator to potential complications. However, general anesthesia may be required in some cases, such as in those with severe pain, high doses of opioid analgesia, or those at risk of cardiopulmonary complications from prone positioning. All cases require continuous monitoring of blood pressure, heart rate, and oxygen saturations. Patient monitoring and sedation are performed by the proceduralists, anesthesiologists, anesthetic nurses, or other certified nursing personnel. For patients with significant preprocedure cardiac or respiratory disease, evaluation by an anesthesiologist may be required to determine the requirements for additional monitored anesthesia care. In all patients, fasting from food and drink is required for at least 4 to 6 hours prior to the procedure.
Thoracic and lumbar vertebroplasty is typically performed with the patient in the prone position. However, it is acceptable to allow the patient freedom to place themself in a prone oblique position to improve their comfort during the procedure. This may introduce approximately 10 to 15 degrees of obliquity. Cushion support should be applied under the upper chest and pelvis (▶Fig. 8.2). This promotes patient comfort, allows clear access to the spine, reduces kyphosis, and maximizes extension of the fractured vertebral segments, which may widen and allow cement penetration.6 The patient’s arms should be placed toward the head to keep them out of the path of the fluoroscope beam. Analgesia should be considered prior to positioning the patient, as transfer from the bed to operating table may be painful. Particular care should be taken when positioning those who are elderly or have advanced osteoporosis or myelomatous infiltration, as transfer may result in new vertebral or rib fractures.
While no clear data currently support or opposes prevertebroplasty administration of antibiotics in nonimmunocompromized patients,7 there are reports of postprocedure spinal infections that are rendered difficult to treat due to the use of PMMA cement.8,9 Prophylactic antibiotics are thus commonly used. Typical regimens include intravenous doses of cefazolin (1–2 g), or clindamycin (600 mg) in patients with penicillin allergy and gentamycin (80–160 mg). Infection risk is further minimized by following standard operating room guidelines for sterile skin preparation, draping, and operator scrubbing.
Fig. 8.2 Setup of the procedure room for a vertebral augmentation procedure. Note the cushion supports prepared on the procedural table for prone positioning.
The vertebroplasty needle is advanced via a small incision, through the skin and subcutaneous tissues and into the target vertebra. It is critical to maintain a needle trajectory that is lateral to the medial cortex and superior to the inferior cortex of the pedicle prior to entry of the needle into the posterior portion of the vertebral body. This prevents passage of the needle into the spinal canal or neural foramen, lowering the risk of spinal cord, cauda equina, or nerve root injury. Ideally, the final needle position should be at the midline of the vertebral body or tumoral target.
In thoracic and lumbar vertebroplasty, the needle may be placed via a transpedicular or parapedicular approach (▶Fig. 8.3). A transpedicular approach involves advancing the needle from the posterior surface of the pedicle, through the entire length of the pedicle, and into the vertebral body. This long intraosseous pathway protects the postganglionic nerve roots and surrounding soft tissues. This approach also provides a clear anatomic landmark for the operator that allows access from the skin into the vertebral body. However, the pedicle configuration can limit the ability to achieve an optimal final needle tip position. The parapedicular approach may permit a more medial placement of the needle tip, and is particularly useful when treating anatomically smaller pedicles, such as in the thoracic spine. The needle is directed along the lateral surface of the pedicle, penetrating the vertebral body at its junction with the pedicle.
Vertebroplasty can be performed with placement of bilateral needles or a single unilateral needle.10 The aim in either approach is the midline spread of cement across the vertebral body from the superior to the inferior end plate. A single needle is often sufficient to achieve this. If the midline position is difficult to achieve due to anatomic constraints, a second needle may be placed on the contralateral side. When performing vertebroplasty, there is little difference in the clinical outcomes achieved with unipedicular versus bipedicular approaches and there are advantages to each approach.11 The primary benefits of a unipedicular approach include reduced procedure time, elimination of the risks associated with placement of a second needle, and lower rates of cement leakage.12 The main advantage of a bipedicular approach is the capacity to inject a greater cement volume.13,14
Vertebroplasty is typically performed using fluoroscopy. Advantages of fluoroscopic guidance include real-time needle positioning and adjustment, and the capacity for continuous monitoring during cement injection. The use of biplane fluoroscopy (two perpendicular image detectors used simultaneously) permits swift alternation between imaging planes without the necessity to move equipment or realign the projection. Alternatively, a single C-arm may be used with views obtained in both the AP and lateral views by simply rotating the C-arm. The goal with both types of fluoroscopic units is to keep the procedure time to a minimum, to adequately visualize the progress and results of the procedure, and to keep the radiation dose as low as possible. For either transpedicular or parapedicular approach, there are multiple image guidance strategies, typically an AP view, or a “down-the-barrel” (end-on) view. The latter technique uses ipsilateral oblique rotation of the image intensifier to place the fluoroscopy beam, pedicle, and needle tract parallel to each other. CT may be used as an adjunctive tool. This cross-sectional imaging modality has superior contrast resolution, and is thus useful for the detection of small cement leaks and, with CT fluoroscopy, allows for continuous real-time monitoring of needle and cement placement.15,16
The following description assumes the use of fluoroscopy for image guidance:
• Rotate the image detector to a true AP position by aligning the spinous process in the midline between the pedicles.
• Center the pedicles within the superior one half of the vertebral body or overlying a compressed vertebral body by adjusting the craniocaudal angulation. Use the lateral fluoroscopic view to assist in determining the correct craniocaudal adjustment required.
• For the end-on view, rotate the image detector approximately 20 to 30 degrees ipsilateral to the target pedicle, so that the medial cortex of the pedicle is at the middle third of the vertebral body. The vertebra adopts the “scottie dog” formation. Place the needle “end on” to the image detector, matching its angulation such that it appears as a dot.
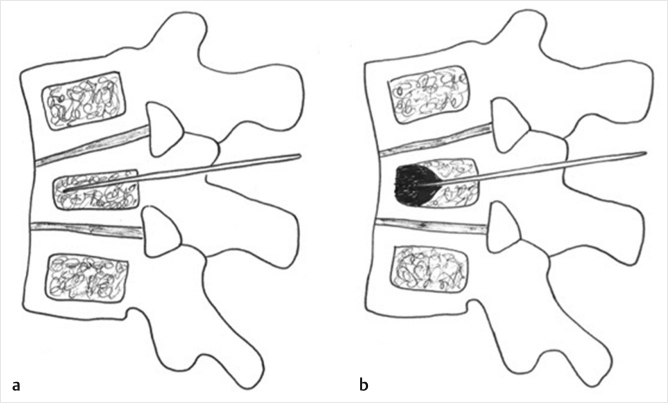
Fig. 8.3 Transpedicular and parapedicular approaches to the vertebral body. (a) The transpedicular approach takes the needle from the posterior surface of the pedicle, through the pedicle’s length, and into the vertebral body. (b) The parapedicular advances the needle along the lateral surface of the pedicle, and penetrates the vertebral body at its junction with the pedicle. This approach may achieve a more medial position of the needle.
• Plan the trocar trajectory. For the transpedicular approach, target the lateral margin of the pedicle, with an entry position at the 2 to 3 o’clock position of the right pedicle or at the 9 to 10 o’clock position of the left pedicle. For the parapedicular approach, the optimal entry position is just lateral to the transpedicular approach position. Preliminary planning of the needle trajectory and prediction of the ultimate route (▶Fig. 8.4) allow operators to make alterations as the needle is advanced.
• Anesthetize the skin, subcutaneous tissues, and periosteum along the expected needle tract and bone entry point with subcutaneous lidocaine or bupivacaine via a 22-gauge needle.
• Make a small cutaneous incision, with the skin entry point decided based on preprocedural imaging and the approach being utilized. Advance the chosen needle to the periosteum.
• During the advancement of the needle to the bone surface, small corrections in the craniocaudal angulation can be made using a lateral view. In the parapedicular approach, the point at which bone is encountered (the junction of the pedicle with the vertebral body) will be more anterior on the lateral view.
• In the bone, advance the needle by gently tapping the handle of the needle with a mallet. The posterior wall of the vertebral body may be detected with a slight change to the “tapping” sound that occurs when advancing the needle with the mallet.17 In soft osteoporotic bone, the needle may pass through with relative ease, with only light mallet strikes.
• If the end-on view was used initially, the needle should be kept as a dot during the initial placement through the pedicle. The needle should remain lateral to the medial cortex of the pedicle until it has navigated through the whole pedicle on the lateral view.
• After traversing the pedicle, if a diamond-tipped needle has been used, it may be replaced with a straight bevel-tipped needle or a curved needle, for improved maneuverability. Using the lateral projection, the needle is advanced further, to the anterior one-third of the vertebral body, and as close to midline as possible or in the anterior portion of the lateral one-third of the vertebral body if a bilateral approach is planned. Confirm final positioning of the needle in both lateral and AP views prior to cement injection. The spinal canal has been cleared if the needle is anterior to the posterior margin of the verte-bral body.
Several types of injectable bone cements are commercially available, including PMMA, composite glass ceramics, and calcium phosphate cements. These differ in terms of cost, polymerization times, biocompatibility, and radio-opacity. PMMA remains the most widely used cement for the treatment of osteoporotic and neoplastic VCFs. Key advantages of PMMA include good radio-opacity and low cost.18 The PMMA cement is prepared by mixing a polymer powder and liquid monomer, resulting in liquid paste.19 The polymerization of PMMA is an exothermic reaction, resulting in increasing thickness of the cement and increased cement temperature of up to 70 to 120°C. This may produce a local thermal cytotoxic effect on neoplastic cells.18 Newer cement materials include composite and calcium phosphate cements. Composite cements do not cause the exothermic reaction of PMMA, and hence avoid potential risks of high cement temperatures and cytotoxic effects. As such, they may be less useful for the treatment of osseous metastases.18 Composite cements have improved biocompatibility, yet have low viscosity that can lead to increased risk of leaks, and a rapid setting time that may lead to the needle staying cemented in the vertebra.20 Calcium phosphate cements have superior biocompatibility, and stimulate new bone formation due to precipitation of crystals from the cement’s injectable form. These cements, however, have longer setting times, higher cost, and lower radio-opacity, and are often less resistant to compression.18,20
Preparation of the cement takes place after needle(s) placement. When ready for injection, the consistency of PMMA cement should be similar to toothpaste with a matte appearance. A “shiny” or glossy appearance of the cement mixture indicates that it is too liquid for use. A “drip” test may be performed, whereby the cement should ball up at the end of the needle and not drip downward.21 Automated mixing systems improve mixing consistency and can be used if available. Depending on the ambient temperature and specific PMMA formulation, working time varies from 10 to 20 minutes. Numerous delivery systems for the cement are available. These vary from 1-mL syringes with a spatula and mixing bowl to self-contained delivery devices. Injectors with long flexible delivery tubing have an advantage of minimizing operator exposure to radiation.22
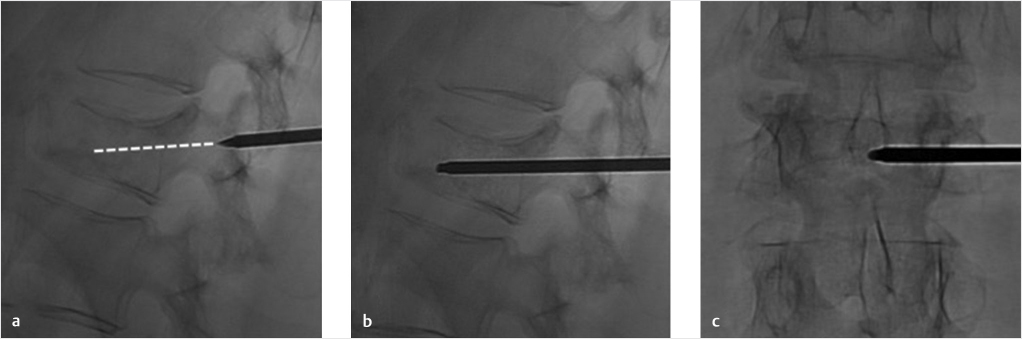
Fig. 8.4 Needle trajectory for a unilateral transpedicular approach in the lumbar spine. (a) Lateral fluoroscopic image of the vertebral body prior to vertebroplasty. The entire needle trajectory is extrapolated during initial transpedicular access to achieve optimal final needle position (dotted line). (b) The needle is advanced into the vertebral body. (c) Anteroposterior fluoroscopic image showing final needle position at midline.
• The needle stylet is removed, and delivery system is connected and the cement is injected at a slow pace to avoid overpressurizing the delivery device with subsequent extravasation.
• Continuous monitoring with lateral and AP fluoroscopy is vital during cement injection, to ensure that the cement remains inside the vertebra and to rapidly identify leaks (▶Fig. 8.5). The risk of cement leakage is greater at the beginning of injection, when the cement is least viscous. New pain reported by the patient should prompt a pause in the procedure and the acquisition of additional imaging views. If cement is observed to pass into a vein, injection should be ceased for 1 to 2 minutes to allow the cement to solidify. The needle position can be adjusted slightly, then the cement may be reinjected to see if it is redirected safely within the vertebral body.23 Larger leaks may necessitate placing additional needles or rarely even abandoning the procedure.
• Suggested endpoints for cement injection include passage of cement beyond the marrow space, and/or cement reaching the posterior wall of the vertebral body on the lateral view. At the end of injection, cement should ideally form a column extending across midline to the contralateral pedicle and from end plate to end plate (▶Fig. 8.6).
• Care should be taken to avoid leaving a “tail” of cement upon concluding cement injection. This can be avoided by reinserting the needle stylet to deliver the residual portion of cement within the hollow cannula and leaving the needle in place for 1 to 2 minutes before removing it. The stylet may also be removed and reinserted to ensure that the cement is not backing up into the cannula. Finally, when withdrawing the needle, a gentle rocking and rotating motion may be employed to ensure the cement within the cannula separates at the cannula tip.
The optimal volume of cement to inject remains is enough to alleviate pain as well as to restore the strength of the vertebral body and its stiffness. Based on the results of an in vitro biomechanical study, Mathis and Wong recommend aiming for 50 to 70% filling of the residual vertebral body volume.24 Recent positive results from the VAPOUR (vertebroplasty for acute painful osteoporotic fractures) randomized controlled trial achieved with large volumes of cement (average 7.5 mL) have also supported larger-volume injections.3 Much smaller volumes of cement have been shown to reduce pain similar to larger volumes and have inherently lower risk of cement extravasation, but more recent recommendations are to fill the vertebral body up to 15 to 25% of the native uncompressed amount.25,26,38 In general, the goal should be maximum cement delivery with careful visual inspection to ensure injection is ceased well prior to complications occurring.
Fig. 8.5 Lateral fluoroscopic image showing minor diskal cement leakage (white arrow) following a vertebral augmentation procedure. Note that no posterior cement leakage has occurred.
Fig. 8.6 Anteroposterior fluoroscopic image of the thoracic spine following vertebroplasty. Note that the injected cement forms a column extending across the midline.
Most vertebroplasty procedures are performed in the thoracic and lumbar spine. Cervical vertebroplasty is technically different due to the small size of target pedicles and vertebral bodies, and the anterior approach to the vertebral body. It is recommended that these procedures be undertaken by somewhat more experienced practitioners and, similar to thoracic or lumbar vertebroplasty, imaging guidance for cervical vertebroplasty may be with either fluoroscopy or CT.27
The precise approach for needle insertion in the cervical spine varies depending on the vertebral level. Procedures performed for C1 and C2 may use a direct transoral approach although a posterolateral approach to the C2 vertebral body has been reported.27,28,39 As only a thin layer of tissue (pharyngeal constrictor muscles, pharyngobasilar fascia, and anterior longitudinal ligament) separates the posterior oropharynx from the upper cervical spine, this approach provides a direct route that avoids adjacent neurovascular structures.27–29 After general anesthesia is provided, the patient is positioned supine on the fluoroscopy table and an oropharyngeal retractor is placed to expose the oropharynx. A large gauge (i.e., smaller diameter) needle is inserted through the posterior pharyngeal wall to gain access to the vertebral body.28
Below the level of C2, either anterolateral or posterior transpedicular approach may be used.27 In the anterolateral approach, the needle trajectory must avoid the carotid sheath complex. The carotid artery should be located by palpation and manually retracted laterally by the operator’s fingers. CT may also be used to visualize the carotid sheath and contents. The needle path ascends from below the angle of the mandible, and advances between the carotid complex, thyroid gland, and esophagus on the patient’s right side. A small guide needle may be useful for confirming safe placement that avoids the carotid complex.30 When the posterior transpedicular approach is used for the cervical spine, the operator should confirm that pedicles are large enough for access. Care is taken to avoid the vertebral artery, located lateral to the pedicle.
The needles are removed once sufficient filling of the vertebral body has occurred. Manual pressure is immediately applied to the needle entry sites for enough time to promote hemostasis and prevent hematoma formation in the soft tissues. A sterile dressing is then applied. Transfer to the stretcher using log roll maneuvers or manual-assisted transfer can occur directly after the procedure, except in the case of vertebral cleft. In these cases, the patient should remain prone on the procedure table for 5 to 10 minutes to allow the cement to further polymerize in the expanded vertebral body.
Vital signs should be performed at regular intervals over the first few hours postprocedure, along with neurologic examinations. In recovery, the patient should remain flat and supine for the first hour, followed by a further 30 minutes to 1 hour with the head of the bed inclined approximately 30 degrees. Following this, patients can begin supervised mobilization when their symptoms become tolerable and the effects of the anesthesia have waned. Initial postprocedure pain at the procedure site may occur and can be relieved with administration of acetaminophen or ketorolac, depending on renal function or ice. The patient is usually able to discriminate any new procedure-related pain, which typically relieves with simple analgesia over the next 24 to 72 hours. Assessment of the patient shortly after vertebroplasty commonly reveals improvement in fracture-related back pain. Persistent severe pain, new severe pain of a different character, or signs of spinal canal stenosis should prompt imaging with CT to exclude complications such as hematoma or cement leakage into neural foramina or spinal canal.
Most vertebroplasty procedures are performed on an outpatient basis, with the patient discharged later the same day following a satisfactory period of observation. More infirm patients may require overnight observation in the hospital. It is recommended to maintain bed rest and minimal activity for the first 24 hours. Regular diet and medications may be resumed on the same day. The patient is counseled to notify the appropriate medical professionals in the case of worsening pain or new pain, swelling, difficulty in walking, sensory changes in the hips and legs, or altered bowel or bladder function. Cross-sectional imaging should be performed in the event of these symptoms occurring, and surgical consult may be considered.
Tenderness may occur at the procedural site for 24 to 48 hours. Pain in the hours following vertebroplasty is typically procedure related. Delayed pain, either at the procedure or in a different location, should raise suspicion of new fracture. Up to one-third of patients will suffer a repeat fracture within 1 to 3 years, most occurring at adjacent vertebral levels.31,32 However, a small percentage (0.6–2.4%) may suffer refracture at a vertebral level previously treated with vertebroplasty.33,34 It should be noted that for up to one-third of patients, bone marrow edema is a normal MRI finding for up to 6 months postvertebroplasty.35 Thus, caution should be taken when interpreting marrow edema at a previously treated level, as it may not indicate a new acute fracture.
Outpatient clinic follow-up should occur typically 2 to 4 weeks postprocedure. At this time, durability of the initial pain improvement, degree of patient mobility, and analgesic requirements are reviewed. The patient is assessed for signs of procedural complications. Subsequent follow-up appointments may take place as is indicated on a case-by-case basis. Management of the underlying cause of fracture is important to prevent future fractures. Optimal osteoporosis treatment should involve vitamin D and calcium supplementation, and medical management with an anabolic bone agent or other targeted therapy as indicated.36,37
Vertebroplasty is a safe and effective treatment for painful VCFs that are refractory to medical management or in patients who are severely debilitated by their vertebral fracture. Meticulous technique and accurate image visualization with fluoroscopy are important to achieve optimal outcomes. With attention to postoperative care and follow-up, the risks of complications are very low. Cervical vertebroplasty presents additional challenges, but may achieve similar success in the hands of experienced operators.
• Vertebroplasty is a minimally invasive procedure that involves the percutaneous injection of cement into a fractured vertebral body.
• Vertebroplasty procedures are performed with image guidance. Fluoroscopy is recommended as it allows continuous monitoring during needle placement and cement injection.
• The trajectory taken to direct the needle into the vertebral body may be either transpedicular or parapedicular. There are advantages to each approach.
• Numerous types of bone cement are available, but PMMA remains the most widely used.
• Most procedures are performed in the thoracic and lumbar spine. Cervical vertebroplasty is less commonly performed and requires some additional considerations such as the type of approach and the size of the needles used.
• A repeat fracture at the treated level or adjacent level can occur and can be prevented with optimal osteoporosis control.
• Most patients report improvement in back pain shortly following vertebroplasty. Delayed pain following initial improvement, or new pain of a different character, should raise suspicion of new fracture.
[1] Syed MI, Shaikh A. Vertebroplasty: a systematic approach. Pain Physician 2007;10(2):367–380
[2] Klazen CAH, Lohle PNM, de Vries J, et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet 2010;376(9746):1085–1092
[3] Clark W, Bird P, Gonski P, et al. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2016;388(10052):1408–1416
[4] Lee IJ, Choi AL, Yie MY, et al. CT evaluation of local leakage of bone cement after percutaneous kyphoplasty and vertebroplasty. Acta Radiol 2010;51(6):649–654
[5] Ploeg WT, Veldhuizen AG, The B, Sietsma MS. Percutaneous vertebroplasty as a treatment for osteoporotic vertebral compression fractures: a systematic review. Eur Spine J 2006;15(12):1749–1758
[6] Teng MM, Wei CJ, Wei LC, et al. Kyphosis correction and height restoration effects of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2003;24(9):1893–1900
[7] Moon E, Tam MDBS, Kikano RN, Karuppasamy K. Prophylactic antibiotic guidelines in modern interventional radiology practice. Semin Intervent Radiol 2010;27(4):327–337
[8] Kallmes DF, Jensen ME. Percutaneous vertebroplasty. Radiology 2003; 229(1):27–36
[9] Yu SW, Chen WJ, Lin WC, Chen YJ, Tu YK. Serious pyogenic spondylitis following vertebroplasty: a case report. Spine 2004;29(10):E209–E211
[10] Ortiz AO, Zoarski GH, Beckerman M. Kyphoplasty. Tech Vasc Interv Radiol 2002;5(4):239–249
[11] Kim AK, Jensen ME, Dion JE, Schweickert PA, Kaufmann TJ, Kallmes DF. Unilateral transpedicular percutaneous vertebroplasty: initial experience. Radiology 2002;222(3):737–741
[12] Kaufmann TJ, Trout AT, Kallmes DF. The effects of cement volume on clinical outcomes of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2006;27(9):1933–1937
[13] Zhu SY, Zhong ZM, Wu Q, Chen JT. Risk factors for bone cement leakage in percutaneous vertebroplasty: a retrospective study of four hundred and eighty five patients. Int Orthop 2016;40(6):1205–1210
[14] Zhang L, Liu Z, Wang J, et al. Unipedicular versus bipedicular percutaneous vertebroplasty for osteoporotic vertebral compression fractures: a prospective randomized study. BMC Musculoskelet Disord 2015;16:145
[15] Caudana R, Renzi Brivio L, Ventura L, Aitini E, Rozzanigo U, Barai G. CT-guided percutaneous vertebroplasty: personal experience in the treatment of osteoporotic fractures and dorsolumbar metastases. Radiol Med (Torino) 2008;113(1):114–133
[16] Vogl TJ, Proschek D, Schwarz W, Mack M, Hochmuth K. CT-guided percutaneous vertebroplasty in the therapy of vertebral compression fractures. Eur Radiol 2006;16(4):797–803
[17] Jay B, Ahn SH. Vertebroplasty. Semin Intervent Radiol 2013;30(3):297–306
[18] Katsanos K, Sabharwal T, Adam A. Percutaneous cementoplasty. Semin Intervent Radiol 2010;27(2):137–147
[19] Lieberman IH, Togawa D, Kayanja MM. Vertebroplasty and kyphoplasty: filler materials. Spine J 2005;5(6, Suppl):305S–316S
[20] Pomrink GJ, DiCicco MP, Clineff TD, Erbe EM. Evaluation of the reaction kinetics of CORTOSS, a thermoset cortical bone void filler. Biomaterials 2003;24(6):1023–1031
[21] Wong W, Mathis J. Is intraosseous venography a significant safety measure in performance of vertebroplasty? J Vasc Interv Radiol 2002;13(2 Pt 1):137–138
[22] Komemushi A, Tanigawa N, Kariya S, Kojima H, Shomura Y, Sawada S. Radiation exposure to operators during vertebroplasty. J Vasc Interv Radiol 2005;16(10):1327–1332
[23] Mathis JM, Ortiz AO, Zoarski GH. Vertebroplasty versus kyphoplasty: a comparison and contrast. AJNR Am J Neuroradiol 2004;25(5):840–845
[24] Mathis JM, Wong W. Percutaneous vertebroplasty: technical considerations. J Vasc Interv Radiol 2003;14(8):953–960
[25] Kaufmann TJ, Trout AT, Kallmes DF. The effects of cement volume on clinical outcomes of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2006;27(9):1933–1937
[26] Molloy S, Riley LH III, Belkoff SM. Effect of cement volume and placement on mechanical-property restoration resulting from vertebroplasty. AJNR Am J Neuroradiol 2005;26(2):401–404
[27] Tsoumakidou G, Too CW, Koch G, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol 2017;40(3):331–342
[28] Anselmetti GC, Manca A, Montemurro F, et al. Vertebroplasty using transoral approach in painful malignant involvement of the second cervical vertebra (C2): a single-institution series of 25 patients. Pain Physician 2012;15(1):35–42
[29] Kaminsky IA, Härtl R, Sigounas D, Mlot S, Patsalides A. Transoral C2 biopsy and vertebroplasty. Interv Med Appl Sci 2013;5(2):76–80
[30] Mathis JM, Golovac S, eds. Image-Guided Spine Interventions. New York, NY: Springer; 2010
[31] Tanigawa N, Kariya S, Komemushi A, et al. Percutaneous vertebroplasty for osteoporotic compression fractures: long-term evaluation of the technical and clinical outcomes. AJR Am J Roentgenol 2011;196(6):1415–1418
[32] Chandra RV, Maingard J, Asadi H, et al. Vertebroplasty and kyphoplasty for osteoporotic vertebral fractures: what are the latest data? AJNR Am J Neuroradiol 2018;39(5):798–806
[33] Chen LH, Hsieh MK, Liao JC, et al. Repeated percutaneous vertebroplasty for refracture of cemented vertebrae. Arch Orthop Trauma Surg 2011;131(7): 927–933
[34] Gaughen JR Jr, Jensen ME, Schweickert PA, Marx WF, Kallmes DF. The therapeutic benefit of repeat percutaneous vertebroplasty at previously treated vertebral levels. AJNR Am J Neuroradiol 2002;23(10):1657–1661
[35] Dansie DM, Luetmer PH, Lane JI, Thielen KR, Wald JT, Kallmes DF. MRI findings after successful vertebroplasty. AJNR Am J Neuroradiol 2005;26(6): 1595–1600
[36] Chandra RV, Meyers PM, Hirsch JA, et al; Society of NeuroInterventional Surgery. Vertebral augmentation: report of the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. J Neurointerv Surg 2014;6(1):7–15
[37] Chandra RV, Yoo AJ, Hirsch JA. Vertebral augmentation: update on safety, efficacy, cost effectiveness and increased survival? Pain Physician 2013;16(4):309–320
[38] Martinčič D, Brojan M, Kosel F, et al. Minimum cement volume for vertebroplasty. Int Orthop 2015;39(4):727–733
[39] Sun HY, Lee JW, Kim KJ, Yeom JS, Kang HS. Percutaneous intervention of the C2 vertebral body using a CT-guided posterolateral approach. AJR Am J Roentgenol 2009;193(6):1703–1705