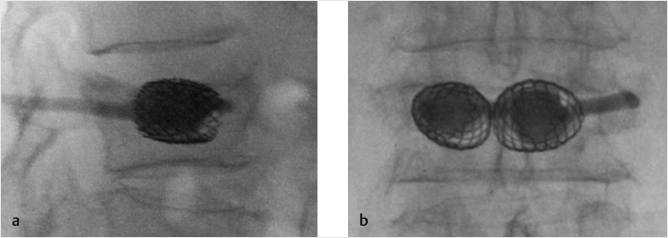
Fig. 12.1 (a) Lateral and (b) posteroanterior fluoroscopy views post implantation and cement injection of vertebral body stents.
Summary
Implant augmentation was developed after vertebroplasty and balloon kyphoplasty and is indicated when improvement of the post-fracture kyphotic angle is a primary treatment goal. Correction of the kyphotic angle and having optimal stabilization of the vertebral body is associated with a decreased rate of additional fractures and greater improvement of pain. The indications and contraindications for vertebral body implants are similar to those for vertebroplasty and balloon kyphoplasty and implants are indicated for fractures associated with trauma, osteoporosis, and neoplasia. The currently used vertebral implants used to treat fractures include the vertebral body stent, the SpineJack, Osseofix, VerteLift, and the Kiva implant. Vertebral implants are typically placed through larger diameter systems so the size of the pedicle should be considered when placing the implant via a transpedicular approach or the physician may opt to use an extrapedicular approach. Implant augmentation is typically slightly more complex than the precursor forms of vertebral augmentation and all of the implants are placed bilaterally except for the Kiva implant which is placed through unilateral access. The main advantages of implant augmentation over vertebroplasty and balloon kyphoplasty include better reduction of the compressed vertebral body, better pain improvement, and less adjacent or additional vertebral compression fractures. Additional investigation into the cost-effectiveness of implant augmentation will need to be done as well as additional development of smaller implants for use in the upper thoracic and cervical spine.
Keywords: implant augmentation, vertebral body stenting, SpineJack, Kiva, Osseofix, VerteLift
Apart from pain and mobility impairment, vertebral compression fractures (VCFs) result in deformities that in the long term can cause potential systemic complications as well as increased chance of future vertebral fractures of either the adjacent vertebral segments or other vertebral bodies.
One of the indications for use of intraosseous implants is the attempt to correct the kyphotic angle. Mechanical effects of kyphosis include decreased thoracic and abdominal space, anterior shift of the craniothoracic center of gravity, and a compensatory counterkyphotic stance with subsequent clinical consequences such as decreased appetite with resultant nutritional impact, frailty, increased future VCF risk, and secondary chronic back pain due to constant paraspinal muscular contraction.1–4 With current evidence, it is clear that percutaneous vertebroplasty and balloon kyphoplasty (BKP) are more efficient than conservative therapy for the management of painful fractures, prolonging survival, and preventing morbidity in these patients.1 Use of vertebral implants, combined with cement injection, is intended to provide analgesic and stabilizing effects along with kyphotic angle correction and vertebral height restoration. Correction of the kyphotic angle may be associated with optimal spinal alignment, paraspinal muscle relaxation, a more upright posture, and reduced pain along with a significantly higher improvement in function and quality of life.4,5
Another potential use of the intraosseous implants is to provide stabilization of the fracture along with the improved sagittal alignment to optimize and decrease the stress on the adjacent vertebral bodies. The prospect of stabilizing the vertebral body by using vertebroplasty or even kyphoplasty might be associated with a higher risk of refracture due to the less optimal restoration of the vertebral height.1,6 In fractures where simple augmentation is contraindicated, the use of an alternative material with different mechanical properties than polymethyl methacrylate (PMMA) can have an additive effect to normalize the spinal compression forces.
The purpose of this chapter is to describe the most commonly used vertebral implants and the implantation procedures associated with placing these implants. The advantages and disadvantages of different products will be addressed.
Vertebral implants for fracture treatment include stents, jacks, polyether ether ketone (PEEK) cages, and fracture reduction systems. Indications for implants include osteoporotic or traumatic fractures as well as primary or metastatic neoplastic spine disease.6,7 The contraindications are similar to those for standard vertebral augmentation techniques, including asymptomatic fractures, pain relief with conservative therapy, local or systemic infection, severe coagulopathy, and severe cardiorespiratory disease.6,7
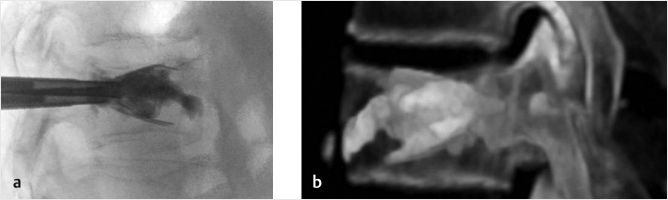
Vertebral body stenting (VBS): VBS is a minimally invasive percutaneous technique during which an expandable cobalt–chromium device is deployed inside the vertebral body (▶Fig. 12.1). The stent access kit includes guidewires, trocars, and working sleeves, drill and blunt plungers, vertebral body balloons and inflation system, vertebral body catheters and stents, as well as cement and a cement delivery system. The balloons and stents are available in three sizes; size selection is based on the preoperative planning via computed tomography scan. Usually, the stents are nonretrievable once expanded.
Fig. 12.1 (a) Lateral and (b) posteroanterior fluoroscopy views post implantation and cement injection of vertebral body stents.
SpineJack: The concept of SpineJack is to achieve a superoinferior restoration of the vertebral body including cortical rings and end plates. The expansion of the implant is progressive and can be maintained until the cement is injected (▶Fig. 12.2). Additionally, in order to best fit for each fracture’s shape and patient’s anatomy, it is possible to expand the implant under the most compressed portion of the VCF. The access kit for spine jack implant includes trocar, Kirschner’s wire, reamer and template, the implant introduction system, and the cement delivery system. Once Spine Jack is expanded, there is no retrieval of the implant.
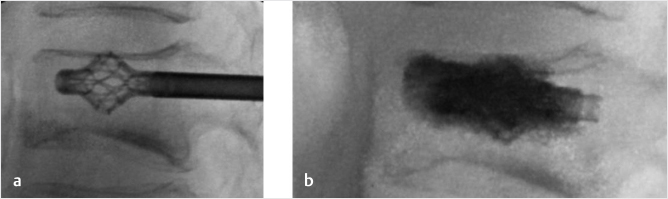
Osseofix: Osseofix (Alphatec Spine, Carlsbad, CA) is an intravertebral expandable titanium mesh cylinder (▶Fig. 12.3). During expansion, the surrounding trabecular bone is compacted and the vertebral height is partially restored and the kyphotic deformity decreased.7 The implant acts as scaffold augmenting the vertebral fracture stabilization and creating channels for subsequent cement injection. Osseofix is indicated for compression fractures at the T6–L5 levels. Once Osseofix is expanded, there is no retrieval of the implant.
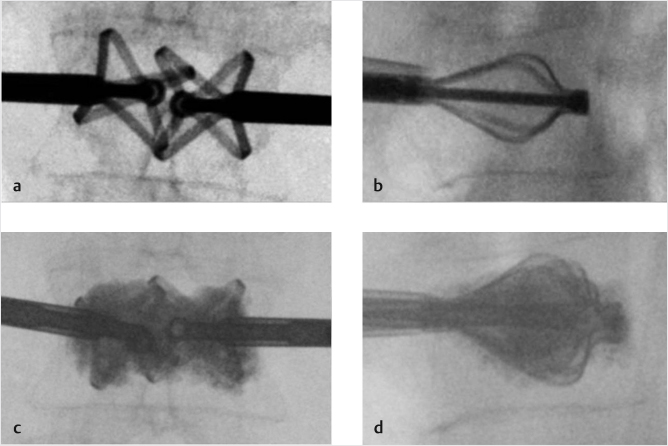
VerteLift: This is a nitinol implant of different sizes and configurations in order to fit each fracture and patient. The implant also has the feature of being able to be repositioned. This nitinol implant is composed of super-elastic struts designed for vertebral end plate support and fracture reduction, which is maintained until bone cement is injected (▶Fig. 12.4). During cement injection, the polymer flows around and through the struts interdigitating with the cancellous bone.
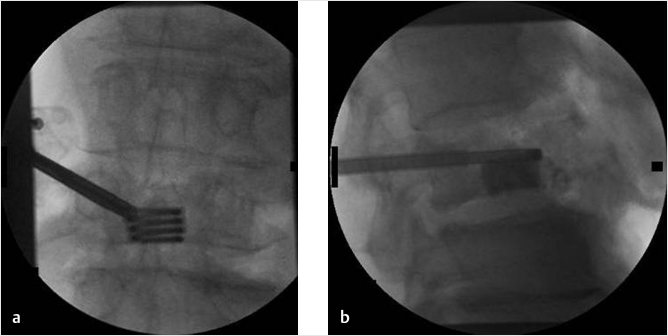
KIVA system: This is a spiraled coiled PEEK-OPTIMA implant loaded with 15% barium sulfate (▶Fig. 12.5). The implant has a distal marker and is indicated for treatment of thoracic and lumbar spinal fractures (T6–L5 levels). The access kit of the KIVA system includes needles, guide pins, a working cannula, a deployment system containing the nitinol coil, and the PEEK polymer cage as well as a cement delivery system. During the expansion of the nitinol coil, the system is retrievable and repositionable. Once the PEEK material is deployed, there is no possibility of withdrawal. The most commonly used percutaneous vertebral implants are listed in ▶Table. 12.1.
Fig. 12.2 Lateral fluoroscopy view (a) and cone beam 3D CT reconstruction (b) post implantation and cement injection of SpineJack.
Fig. 12.4 (a, b) Posteroanterior and lateral fluoroscopy views during deployment of (c, d). Posteroanterior and lateral fluoroscopy views during cement injection in VerteLift.
Fig. 12.5 (a) Posteroanterior fluoroscopy view during deployment of KIVA and (b) lateral fluoroscopy view during cement injection.
From a technical point of view, introduction of these devices is performed through working cannulas of larger diameters than the standard trocars used in vertebroplasty and therefore size of the pedicle is an important feasibility and success factor when the proceduralist chooses a transpedicular approach. In some cases, where there is a preference for the use of implants, an extrapedicular approach can be opted for. Additionally, deployment of each implant is a more complex procedure when compared to standard augmentation techniques often requiring a learning curve for optimal performance. In all cases and for all products, the patient is placed in a prone position and implantation is performed via fluoroscopic guidance.
VBS: Vertebral body stents are placed through an extra- or transpedicular approach. The trocars are inserted inside the vertebral body, thus creating a pathway for positioning of the instruments in a single step. The final position of the trocars should be such that it allows placement of the two stents symmetrically toward the midline. The trocar is exchanged for a working cannula over a wire. The drill and the blunt plunger are sequentially inserted through the working cannula in order to create space and an access channel for the stents (in the distal tip of the plunger, there are three grooves that correspond to the different stent lengths available). Following this, a vertebral body balloon catheter (selected on the basis of stent size) is inserted through the working sleeve and positioned to the anticipated stent location. After dilatation with the inflation system, the balloon catheters are retrieved and the vertebral body stent catheters are inserted and deployed.8 After catheter removal, PMMA is injected under real-time fluoroscopic control in, and around, the implant (▶Fig. 12.1). The cement preferentially fills the cavity created by the balloons and supported by the stents.8,9
SpineJack: Needles are inserted into the vertebral body via a transpedicular approach. The needles are then exchanged over a guidewire for a drill and a working cannula. The drill is used to create a channel inside the vertebral body. The working cannula is left in place after removal of the drill and a template is then used for removing residual bone fragments in the implant’s location. A cannula plug is inserted for any potential bleeding and a radiopaque marker in the cannula plug allows the operator to visualize the implant’s depth. A SpineJack implant is then inserted and cement is injected using bone fillers through the expander (▶Fig. 12.2).10
Osseofix: Targeting needles are inserted into the posterior portion of the vertebral body. This is followed by sequential exchanges over guidewires, and drill sleeves are introduced. The drill creates an access channel. The diameter of the drill corresponds to the diameter of a nonexpanded implant. The drill is then removed and the sleeve is replaced by the working cannula through which the nonexpanded implant is inserted and then subsequently expanded (the system has a stop mechanism to prevent excessive expansion). Once the implant is dilated, it cannot be percutaneously removed. Finally, cement is injected into the implant though the working cannula (▶Fig. 12.3).11,12
VerteLift: Access cannulas for the VerteLift system are inserted through the access needles and a manual drill is used to create the implant’s delivery pathway. The implants are delivered, positioned, and deployed using a multifunctional handle attached to the delivery system. After correct positioning of the implant, the delivery system is detached and injection of cement follows (▶Fig. 12.4).13
KIVA system: A standard needle is inserted into the vertebral body using a transpedicular approach. The needle is place ipsilaterally and horizontally aligned with the unfractured end plate aiming at the lateral portion of the vertebral body. A guide pin is used to exchange the needle cannula with a drilling dilator and that is then introduced into the vertebral body. The drilling dilatory is placed up to 3 to 5 mm from the anterior vertebral body all which leaves the shorter working cannula positioned just anterior to the posterior vertebral body wall. The appropriate implant deployment device is then chosen for either a right-sided or a left-sided insertion and the nitinol wire is then inserted into the vertebral body by twisting the blue knob on the side of the deployment device. After the nitinol wire is placed, the PEEK implant is inserted into the vertebral body over the coiled wire by twisting the white knob on the other side of the deployment device. After the PEEK implant is delivered over the guidewire in a continuous, spiral loop, the wire is removed and the PEEK cage is filled with cement (▶Fig. 12.5).4
According to the manufacturer’s guidelines, the vast majority of vertebral implants should be placed in pairs inside the vertebral body through a bilateral access. The KIVA system is the only implant, according to the manufacturer’s guidelines, that is designed to be placed via a unilateral transpedicular approach. Pua et al have proposed the “central stentoplasty” approach inserting the Osseofix titanium mesh cage system into vertebral bodies using cone-beam CT guidance.15 Unilateral approaches receive less radiation dose and operation time, being similarly effective in alleviating the back pain, but a unilateral approach may be less effective at reducing the vertebral fracture and reestablishing the prefracture vertebral height. There is a paucity of data; however, comparing unilateral and bilateral approaches for implant placement and additional randomized controlled trials would be needed to assess for safety, efficacy, biomechanical stability, and adverse events related to unilateral and bilateral approaches.
Implants aim to provide long-term vertebral height restoration and correction of kyphosis, as well as additional support compared to standard augmentation. In selected cases of extreme fractures, implants can work as anchors, thus providing extra support against shearing forces, where the risk of cement failure is higher. Thus far, there are no completed and published clinical studies proving the concept of structural support superiority to standard cement or evidence of superiority of one device over the other. Despite this, preliminary data available at the time of this writing from the 151-patient randomized placebo-controlled SAKOS trial comparing the SpineJack to the KyphX Xpander Inflatable Bone Tamp suggest that both SpineJack and BKP had comparable effects on function improvement and QOL, but SpineJack appears to be significantly better than BKP for pain relief, VB height restoration, and in decreasing the rate of adjacent fractures.20
Most biomechanical and other clinical comparative studies versus standard augmentation techniques thus far report noninferiority of spine implants with a reduced volume of injected cement.14 In addition to optimal fracture repair, Noriega et al reported that restoration of the previous spinal alignment at the fractured segment seems to be a crucial factor for the maintenance of normal disk diffusion.16 In another study comparing an early version of vertebral stents with BKP, Werner et al reported that vertebral body stents are associated with significantly higher pressures during balloon inflation and more material-related complications. This was a relatively small study with only 100 fractures assessed, but the results showed no clear beneficial effect of the stent over that of traditional BKP.17
The disadvantage of all implants is their higher initial cost when compared to that of standard vertebral augmentation techniques. The smaller proportion of VCF patients who are treated with implants can cost up to 70% of the total budget for vertebral augmentation.6,7,18 At the moment, there is no study reporting cost-effectiveness of vertebral implants over standard techniques, so the final determination as to the relative cost-effectiveness is uncertain. Cost-effectiveness assessments are essential as it has been shown that despite an initially higher cost, BKP was found to be more cost-effective than vertebroplasty within 2 years in a U.S. study by Ong et al and within 4 years in a European study by Lange et al.21,22
Cost-effectiveness is determined by many factors including quality of treatment effect, so a greater benefit provided to the patient could give rise to greater cost-effectiveness over time relative to technologies with a lower initial cost. Other disadvantages of vertebral implant include the aspect that it is somewhat more invasive, the implants are irretrievable, and there is an absence of adapted material for implantation in the cervical and upper thoracic spine and in the sacrum.18
Depending on the product used, the injection of the cement should be done according to the manufacturer’s guidelines; in the first 2 hours, vital signs and neurological evaluations mainly of the extremities should be routinely monitored.19 A CT scan can be used to evaluate the anatomic outcome of the fracture treatment including the vertebral reduction, kyphotic angle correction and any potential cement leakage, device migration/fracture, or any spinal canal compromise or bony retropulsion. If the patient has persistent significant pain after vertebral augmentation, MRI can be used for additional assessment.19
[1] Filippiadis DK, Marcia S, Masala S, Deschamps F, Kelekis A. Percutaneous vertebroplasty and kyphoplasty: current status, new developments and old controversies. Cardiovasc Intervent Radiol 2017;40(12):1815–1823
[2] Schlaich C, Minne HW, Bruckner T, et al. Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int 1998;8(3):261–267
[3] Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR. Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporos Int 2005;16(8):1004–1010
[4] Silverman SL. The clinical consequences of vertebral compression fracture. Bone 1992;13(Suppl 2):S27–S31
[5] Kado DM, Lui LY, Ensrud KE, Fink HA, Karlamangla AS, Cummings SR; Study of Osteoporotic Fractures. Hyperkyphosis predicts mortality independent of vertebral osteoporosis in older women. Ann Intern Med 2009;150(10): 681–687
[6] Guglielmi G, Andreula C, Muto M, Gilula LA. Percutaneous vertebroplasty: indications, contraindications, technique, and complications. Acta Radiol 2005;46(3):256–268
[7] Muto M, Perrotta V, Guarnieri G, et al. Vertebroplasty and kyphoplasty: friends or foes? Radiol Med (Torino) 2008;113(8):1171–1184
[8] Heini PF, Teuscher R. Vertebral body stenting / stentoplasty. Swiss Med Wkly 2012;142:w13658
[9] Aparisi F. Vertebroplasty and kyphoplasty in vertebral osteoporotic fractures. Semin Musculoskelet Radiol 2016;20(4):382–391
[10] Sietsma MS, Hosman AJ, Verdonschot NJ, Aalsma AM, Veldhuizen AG. Biomechanical evaluation of the vertebral jack tool and the inflatable bone tamp for reduction of osteoporotic spine fractures. Spine 2009;34(18): E640–E644
[11] Ender SA, Gradl G, Ender M, Langner S, Merk HR, Kayser R. Osseofix system for percutaneous stabilization of osteoporotic and tumorous vertebral compression fractures: clinical and radiological results after 12 months. RoFo Fortschr Geb Rontgenstr Nuklearmed 2014;186(4):380–387
[12] Ender SA, Wetterau E, Ender M, Kühn JP, Merk HR, Kayser R. Percutaneous stabilization system Osseofix for treatment of osteoporotic vertebral compression fractures: clinical and radiological results after 12 months. PLoS One 2013;8(6):e65119
[13] Anselmetti GC, Manca A, Marcia S, et al. Vertebral augmentation with nitinol endoprosthesis: clinical experience in 40 patients with 1-year follow-up. Cardiovasc Intervent Radiol 2014;37(1):193–202
[14] Tutton SM, Pflugmacher R, Davidian M, Beall DP, Facchini FR, Garfin SR. KAST study: the Kiva system as a vertebral augmentation treatment—a safety and effectiveness trial: a randomized, noninferiority trial comparing the kiva system with balloon kyphoplasty in treatment of osteoporotic vertebral compression fractures. Spine 2015;40(12):865–875
[15] Pua U, Quek LH, Ng LC. Central stentoplasty: technique for unipedicular single midline vertebral body stent implantation. Cardiovasc Intervent Radiol 2014;37(3):810–814
[16] Noriega DC, Marcia S, Ardura F, Lite IS, Marras M, Saba L. Diffusion-weighted mri assessment of adjacent disc degeneration after thoracolumbar vertebral fractures. Cardiovasc Intervent Radiol 2016;39(9):1306–1314
[17] Werner CM, Osterhoff G, Schlickeiser J, et al. Vertebral body stenting versus kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a randomized trial. J Bone Joint Surg Am 2013;95(7):577–584
[18] Muto M, Marcia S, Guarnieri G, Pereira V. Assisted techniques for vertebral cementoplasty: why should we do it? Eur J Radiol 2015;84(5):783–788
[19] Tsoumakidou G, Too CW, Koch G, et al. CIRSE Guidelines on Percutaneous Vertebral Augmentation. Cardiovasc Intervent Radiol 2017;40(3):331–342
[20] U.S. National Library of Medicine; ClinicalTrials.gov. A prospective multicenter, randomized, comparative clinical study to compare the safety and effectiveness of two vertebral compression fracture (VCF) reduction techniques: the SpineJack and the KyphX Xpander Inflatable Bone Tamp. Interim clinical study report. Available at: https://clinicaltrials.gov/ct2/show/NCT02461810. Published May 1, 2018. Accessed June 17, 2018
[21] Ong KL, Lau E, Kemner JE, Kurtz SM. Two-year cost comparison of vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: are initial surgical costs misleading? Osteoporos Int 2013;24(4): 1437–1445
[22] Lange A, Kasperk C, Alvares L, Sauermann S, Braun S. Survival and cost comparison of kyphoplasty and percutaneous vertebroplasty using German claims data. Spine 2014;39(4):318–326