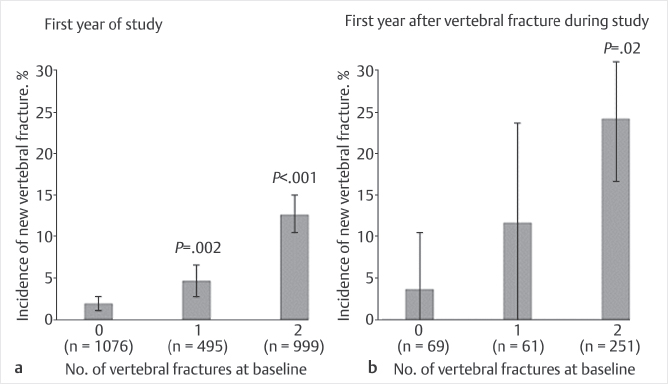
Fig. 23.1 (a, b) Incidence of vertebral fracture by number of baseline vertebral fractures. New compression fractures happened more in previous multilevel fractures at 1-year follow-up.
Summary
Vertebral augmentation, such as vertebroplasty and kyphoplasty has been introduced as effective treatment options for vertebral compression fracture. Unfortunately, there are many multiple level fractures in both osteoporotic and metastatic compression fractures. There are also still some questions about the maximum number of levels that should undergo vertebral augmentation. Current guidelines indicate that complications of vertebral augmentation may be amplified when more than three vertebral levels are treated concurrently but this has not been reflected in numerous clinical trials, and some researchers have found that complications such as anemia and new compression fracture did not increase with multiple levels of augmentation. They also suggested that treating all the fractures at once might decrease the patients’ morbidity. In conclusion although the number of compression fracture levels to treat with vertebral augmentation should be based on a meticulous analysis of each individual’s circumstances and many levels can be treated in an attempt to decrease patient morbidity, a generally agreed upon maximum number of levels is three per augmentation session.
Keywords: complications, levels, multiple compression fractures, vertebral augmentation
Vertebral compression fractures (VCFs) related to osteoporosis are very common in the elderly.1,2 In recent years, minimally invasive percutaneous cement augmentation techniques, such as vertebroplasty and kyphoplasty, have been introduced as effective treatment options.2–8 These techniques have demonstrated excellent clinical outcomes, restoring the collapsed body height and reducing pain both in the short- and long-term.2,4 However, one of the difficulties of vertebral augmentation techniques is the treatment of multiple fractures.3 In both osteoporosis and metastasis, it is common to find multiple fractures, and about 20 to 47% of the patients with a previously diagnosed compression fracture develop new ones.5–7,9 Consequently, some authors suggest the prophylactic augmentation of decalcified vertebrae as a method to prevent subsequent fractures that may increase overall mortality.8,10,11 Additionally, almost 4% of the fractures are a consequence of neoplastic disease, which can be sampled during the vertebral augmentation procedure via vertebral biopsy.12–14 Pathological fractures due to malignant tumors of the vertebrae also have been found to be adequately treated with vertebroplasty, which can produce sufficient pain control and a better quality of life.15,16
From the retrospective analysis of cancer patients, most compression fractures occurred at the thoracolumbar junction, with T11, T12, L1, and L2 accounting for 69.4% of all treated levels. The distribution of compression fractures by type of cancer show that 88.2% of documented metastatic compression fractures and 71% of all compression fractures had multiple myeloma, breast cancer, or lung cancer. Unlike osteoporotic compression fractures, in cancer patients there was a fairly even distribution of all compression fractures and metastatic compression fractures between the two sexes.17
In a study with postmenopausal Japanese-American women, Ross et al18 found a fivefold increase in the risk of a new vertebral fracture when a single vertebral fracture was present at baseline. This risk increased to 12-fold when there were two or more fractures at baseline. Lindsay et al19 in a multicenter study involving 2,725 postmenopausal women with a mean age of 74 years found a cumulative incidence of 6.6% new fractures in the first year. Overall, 19.2% of the women with a confirmed incidental fracture had a second fracture within one year; 11.5% of the women with one previous fracture sustained a second fracture, whereas 24% of the women with two or more prevalent fractures at baseline had a new fracture within a year following the first observed fracture (▶Fig. 23.1).
Bed rest or inactivity as a result of pain from VCFs accelerates bone loss, which may increase the risk of additional fractures. Increased kyphosis from previous fractures also predisposes the patient to recurrent fractures. Black et al20 found that prevalent vertebral deformities from previous fractures were associated with a fivefold increase in the risk of new fractures. Moreover, the risk was higher as the number of preexisting fractures and the severity of the deformity increased. Additionally, the presence of multiple and severe VCFs was found to be a specific risk factor for sustaining femoral neck fractures.21
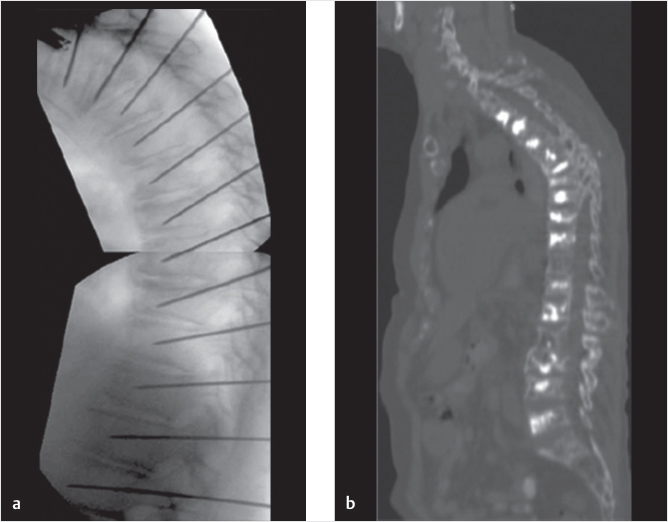
Although there is extensive information regarding the increased incidence of new vertebral fractures after an initial one, there is no firm consensus on how many levels should be treated with vertebral augmentation. Some authors have suggested that the augmentation of one vertebra can increase the probability of new fractures in the adjacent ones; thus, prophylactic augmentation of decalcified vertebrae should be considered.8,10 Moreover, there are cases with multiple compression fractures, and as many as 16 levels of augmentations in a single patient have been reported (▶Fig. 23.2).22 However, there are still some questions about the number of levels that should undergo vertebral augmentation. Should all the compressed levels be treated with augmentation? If not, which level(s) should be chosen to perform the vertebral augmentation? Finally, in the case of a single-level compression, is it better to perform an additional augmentation to the adjacent decalcified vertebrae?
Fig. 23.1 (a, b) Incidence of vertebral fracture by number of baseline vertebral fractures. New compression fractures happened more in previous multilevel fractures at 1-year follow-up.
Fig. 23.2 (a, b) Multilevel vertebral augmentation. As many as 16 levels were treated with vertebral augmentation.
First of all, attention must be centered in the accurate diagnosis of the compressed fracture level that is contributing to the recent pain escalation. Lyritis et al23 attempted to determine the clinical outcomes based on the initial radiographic appearance of the vertebral fractures. In their study, patients with an obvious wedge fracture had severe, sharp pain, which gradually decreased within 4 to 8 weeks (▶Fig. 23.3). Conversely, patients with minimal superior end-plate discontinuity tended to have a gradual progression to complete collapse of the vertebral body and had dull, less severe, and recurrent pain. Conclusively, before considering a vertebral augmentation, a thoughtful, cautious, and accurate physical examination must be performed. In the patients with a possible VCF, the key physical examination signs are the presence of severe concordant pain with palpation or percussion on the suspected fractured spinous process, deep tenderness of paravertebral muscle pain, and facet joint compression. Langdon et al24 found that closed-fist percussion had sensitivity and specificity of 87.5 and 90%, respectively, for detecting VCFs. These authors also described a supine sign test that was 81.25% sensitive and 93.33% specific for detecting VCFs when the patient was unable to lie supine without prominent discomfort. Finally, when both physical and radiographic image examinations are positive for vertebral fracture, performing vertebral augmentation at one or two levels is often enough to successfully control the acute pain.
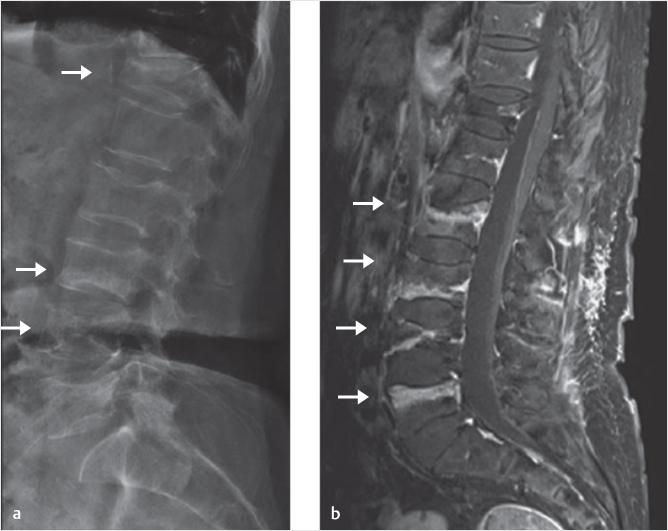
Fig. 23.4 (a, b) Hidden multiple compression fracture. MRI revealed the hidden acute fractures (arrows).
In cases with multiple compression fractures, Wang and Fahim16 concluded that the patients treated with vertebral augmentation at once had better pain control than the ones treated in two different sessions, the first to repair a portion of the fractured vertebral bodies and a second to repair the remaining fractures. The patients with two procedures remained bed bound due to the persistent pain, had an increased hospice stay, and suffered additional morbidities. Additionally, there may be hidden neoplastic lesions or fractures despite the interrogation by experienced physical examinations and conventional radiography. Bone scanning plays a role in identifying osteoporotic fractures in patients who have negative findings on plain radiographs and in identifying additional fractures at other levels. Magnetic resonance imaging (MRI) of the spine is one of the most useful tests for determining fracture age, ruling out a malignant tumor, and selecting the appropriate treatment. Park et al25 suggested that MRI with STIR sequencing exhibited a multitude of benefits in the exact identification of both acute and hidden lesions. In this study, MRI with STIR sequencing revealed that 23% of the single fracture group and 65% of the multiple fracture group had additional acute lesions that were not identified on a CT scan (▶Fig. 23.4). Therefore, as suggested in previous studies, the determination of the appropriate level is critical to achieving better clinical outcomes after vertebral augmentation. Additionally, 31 of their cases had multiple hidden lesions. They concluded that if the hidden lessons are not treated and the cement augmentation is performed at a single level only, undesirable clinical outcomes may arise as a consequence of the missed and untreated lesion(s) which may further deteriorate after the initial procedure. In neoplastic lesions bone SPECT may be comparable for differentiating malignant from benign VCFs, especially, in the case of VCFs with a complete replacement of the normal fatty marrow. This means it is possible to use bone single-photon emission tomography (SPECT) as a substitute for MRI for differentiating malignant from benign VCFs.26
Other authors and published guidelines on vertebral augmentation consider a safe practice not to perform more than three levels in a single session to avoid major complications. This is a somewhat arbitrary rule that limits amount of pulmonary flow of marrow material and nearly always provides a safe limit on the patient’s exposure to the potential hazards of the procedure especially if the operators are not extensively experienced in vertebral augmentation.27–31
Current guidelines indicate that complications of vertebral augmentation may be amplified when more than three vertebral levels are treated concurrently. There is purported increased risk of infection, bleeding, local trauma (pneumothorax, fracture of ribs, and adjacent vertebra), cement leakage (radiculopathy, canal stenosis, paralysis), pulmonary embolism, and death. Additionally, there is a theoretical increased risk of anemia, especially in elderly patients, due to the role of the vertebrae in hematopoiesis. Lee et al32 analyzed the complications of percutaneous vertebral augmentation. They reviewed the procedural complications rate per the number of levels treated and found that vertebroplasty had a significantly increased rate of complications compared with kyphoplasty in all the prospective studies included in the meta-analysis (▶Table 23.1). Additionally, the ratio of total cement leaks per number of levels treated were significantly higher for vertebroplasty, after isolating pathologic and osteoporotic fractures (▶Table 23.2).
Although early vertebral augmentation procedures focused on the complete fill of the vertebral body, it is now evident that somewhat smaller volumes may restore the biomechanical properties of the vertebral body appropriately. Moreover, the volume of cement injected into the vertebral body is directly related to the stiffness and strength that is achieved.33 Therefore, a lesser amount of approximately 15 to 25% volume fraction may be adequate to restore the stiffness of the vertebral body to its prefractured level. Additionally, if the vertebral body is filled preferentially on one side the stiffness of the nonaugmented side may be lower than the augmented side, which might lead to an imbalance of stress on the vertebral body in the unilaterally filled vertebral body. However, when cement crosses the midline, stiffness of both sides increase comparatively and biomechanical balance is thus achieved.34 For this reason, a significant number of clinicians tend to hesitate to perform multiple vertebral augmentation, especially if the cement fill per vertebral bodies is relatively replete.
In order to decrease the complications such as anemia after multilevel vertebral vertebroplasty and kyphoplasty, some clinicians reduced the amount of cement injected. There are two approaches for the cement filling, a bipedicular approach that requires the cannulation of both sides of the vertebral body for cement injection and the unipedicular technique that accesses one side to inject the polymethylmethacrylate (PMMA).35,36 The latter theoretically reduces the risks involved with cannulation by 50% and also potentially reduces procedure time and radiation exposure. The PMMA is cytotoxic due to its chemical and thermal effects during polymerization, and the temperature during polymerization is high enough to produce coagulation of tumoral cells. Therefore, care should be taken when deciding the amount of cement. There should be enough to fill the center of the vertebral body and have the cement extend from superior end plate to the inferior end plate. In regard to fill material, PMMA has been used successfully, and almost exclusively, for vertebroplasty and kyphoplasty. The advantages of this product are that: (1) surgeons and proceduralists are familiar with it, (2) it is easy to handle, (3) radiopaque materials can be added to it, (4) it provides the necessary strength and stiffness to be durable, and (5) it is inexpensive. Conversely, the disadvantages are that: (1) it has no osteoinductive properties, (2) high polymerization temperatures can occasionally result in damage to surrounding tissues, (3) unreacted monomer has systemic cardiopulmonary side effects, and (4) it is not remodeled by creeping substitution over time. Although several investigators have reported promising results of vertebral augmentation with the use of biodegradable products, such as calcium phosphate, hydroxyapatite, or coral granules in vitro, there is insufficient evidence in clinical practice for the use of most of these alternative fill materials.37
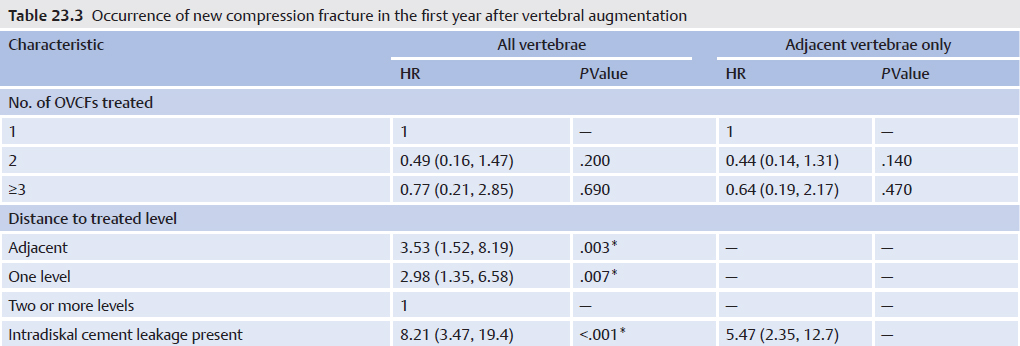
Nieto-Iglesias et al38 investigated the occurrence of new vertebral fractures after percutaneous vertebroplasty and reported that adjacent vertebral procedure and intradiskal cement leakage were risk factors for new fractures. Additionally, the incidence of new compression fractures tended to increase when more levels of vertebroplasty were performed (▶Table 23.3). In a prospective study containing 290 consecutive patients with 363 fractures, Yi et al found no increased risk of VCF for those patients treated with vertebral augmentation as compared to those patients treated with NSM but they did find that the additional fractures occurred sooner in patients treated with vertebral augmentation.39 This may serve to explain the impression that more fractures occur after vertebral augmentation despite clear evidence that this is not the case.40
Some particular causes of compression fracture, such as multiple myeloma, secondary osteoporosis, and metastases, where the patients have more than three painful vertebral collapses, are recommended to undergo multilevel treatment to achieve back-pain regression and to improve their quality of life. In these cases, if a mini-invasive technique is employed by a skilled operator, multilevel vertebroplasty could be feasible, safe, and successful. Hussein et al41 declared in the international myeloma working group consensus statement in 2008 that multiple augmentation procedures for multiple myeloma may be necessary and appropriate. In general, three to four vertebrae per intervention is considered reasonable and feasible during a single procedure when needed. Additionally, they recommended that vertebral augmentation for adjacent or suspicious vertebrae without fracture may be necessary. The prophylactic augmentation may be considered in cases of fracture with kyphosis in the thoracolumbar region because the stress resultant from the deformity in this region is very high.8,10 Another consideration for prophylactic augmentation is the cases when the vertebra is located between two fractured vertebrae such as T11 and L1, in which T12 requires treatment to avoid postprocedure collapse.
Wang and Fahim16 evaluated the complications after multilevel (above four levels) kyphoplasty which was performed in 19 patients to a total of 189 levels. Unexpectedly, none of the patients developed anemia after multilevel kyphoplasty, but 13 (68.4%) of the 19 patients had anemia before the procedure and continued to have anemia after the surgery. The authors concluded that there are no absolute contraindications to multilevel kyphoplasty, and they disagree with the recommended maximum number of vertebrae that may be treated at one time. Conversely, patients with untreated levels of fracture spent more days in bed, which results in increased risks of deep venous thrombosis (DVT), decubitus ulcers, atelectasis, pneumonia, loss of muscle mass, loss of bone density, and other health detriments associated with immobility. Therefore, treating all the fractures at once in the same anesthetic time, regardless of their location in the thoracic or the lumbar spine, may decrease the morbidity associated with delaying ambulation and, conversely, leaving some painful fractures untreated may increase the risk of such complications. Nonetheless, the decision should be taken case by case, according to each patient’s circumstances including the precise level, the biomechanical properties, the patient’s general conditions, premedical history, and the physician’s experience, among others.
In conclusion, the number of compression fracture levels to treat with vertebral augmentation should be based on a meticulous analysis of the individual’s circumstances and according to technical modulations. However, it is evident that complications such as anemia and new compression fractures after vertebral augmentation might not be serious and are preventable for experienced physicians.
[1] Farrokhi MR, Alibai E, Maghami Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J Neurosurg Spine 2011;14(5):561–569
[2] Genev IK, Tobin MK, Zaidi SP, Khan SR, Amirouche FML, Mehta AI. Spinal compression fracture management: a review of current treatment strategies and possible future avenues. Global Spine J 2017;7(1):71–82
[3] Watts NB. Is percutaneous vertebral augmentation (vertebroplasty) effective treatment for painful vertebral fractures? Am J Med 2003;114(4):326–328
[4] Li L, Ren J, Liu J, et al. Wang X, Liu Z, Sun T. Results of vertebral augmentation treatment for patients of painful osteoporotic vertebral compression fractures; A meta-analysis of eight randomized controlled trials. PLoS One 2015;10(9):e0138126
[5] Longo UG, Loppini M, Denaro L, Maffulli N, Denaro V. Osteoporotic vertebral fractures: current concepts of conservative care. Br Med Bull 2012;102:171–189
[6] Hsieh MK, Chen LH, Chen WJ. Current concepts of percutaneous balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: evidence-based review. Biomed J 2013;36(4):154–161
[7] Taylor RS, Taylor RJ, Fritzell P. Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a comparative systematic review of efficacy and safety. Spine 2006;31(23):2747–2755
[8] Chiang CK, Wang YH, Yang CY, Yang BD, Wang JL. Prophylactic vertebroplasty may reduce the risk of adjacent intact vertebra from fatigue injury: an ex vivo biomechanical study. Spine 2009;34(4):356–364
[9] Beall DP, Chambers MF, Thomas SM, et al. Prospective and multicenter evaluation of outcomes for quality of life and activities of daily living for balloon kyphoplasty in the treatment of vertebral compression fractures: the EVOLVE trial. J Neurosurg 2018;0:1–11
[10] Kulcsár Z, Marosfoi M, Berentei Z, Veres R, Nyáry I, Szikora I. [Frequency of adjacent vertebral fractures following percutaneous vertebroplasty] Orv Hetil 2009;150(37):1744–1748
[11] Ong KL, Beall DP, Frohbergh M, Lau E, Hirsch J. Were VCF patients at higher risk of mortality following the 2009 publication of the vertebroplasty “sham” trials? Osteoporos Int 2017;doi:10.1007/s00198-017-4281-z
[12] Saracen A, Kotwica Z. Treatment of multiple osteoporotic vertebral compression fractures by percutaneous cement augmentation. Int Orthop 2014;38(11):2309–2312
[13] Tseng YY, Yang TC, Tu PH, Lo YL, Yang ST. Repeated and multiple new vertebral compression fractures after percutaneous transpedicular vertebroplasty. Spine 2009;34(18):1917–1922
[14] Cosar M, Sasani M, Oktenoglu T, et al. The major complications of transpedicular vertebroplasty. J Neurosurg Spine 2009;11(5):607–613
[15] Kotwica Z, Saracen A. Early and long-term outcomes of vertebroplasty for single osteoporotic fractures. Neurol Neurochir Pol 2011;45(5):431–435
[16] Wang AC, Fahim DK. Safety and efficacy of balloon kyphoplasty at 4 or more levels in a single anesthetic session. J Neurosurg Spine 2018;28(4):372–378
[17] Jha RM, Hirsch AE, Yoo AJ, Ozonoff A, Growney M, Hirsch JA. Palliation of compression fractures in cancer patients by vertebral augmentation: a retrospective analysis. J Neurointerv Surg 2010;2(3):221–228
[18] Ross PD, Davis JW, Epstein RS, Wasnich RD. Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med 1991;114(11):919–923
[19] Lindsay R, Silverman SL, Cooper C, et al. Risk of new vertebral fracture in the year following a fracture. JAMA 2001;285(3):320–323
[20] Black DM, Arden NK, Palermo L, Pearson J, Cummings SR; Study of Osteoporotic Fractures Research Group. Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. J Bone Miner Res 1999;14(5):821–828
[21] Kinoshita T, Ebara S, Kamimura M, et al. Nontraumatic lumbar vertebral compression fracture as a risk factor for femoral neck fractures in involutional osteoporotic patients. J Bone Miner Metab 1999;17(3):201–205
[22] Erdem E, Samant R, Malak SF, et al. Vertebral augmentation in the treatment of pathologic compression fractures in 792 patients with multiple myeloma. Leukemia 2013;27(12):2391–2393
[23] Lyritis GP, Mayasis B, Tsakalakos N, et al. The natural history of the osteoporotic vertebral fracture. Clin Rheumatol 1989;8(Suppl 2):66–69
[24] Langdon J, Way A, Heaton S, Bernard J, Molloy S. Vertebral compression fractures: new clinical signs to aid diagnosis. Ann R Coll Surg Engl 2010;92:163–166
[25] Park SY, Lee SH, Suh SW, Park JH, Kim TG. Usefulness of MRI in determining the appropriate level of cement augmentation for acute osteoporotic vertebral compression fractures. J Spinal Disord Tech 2013;26(3):E80–E85
[26] Tokuda O, Harada Y, Ueda T, Ohishi Y, Matsunaga N. Malignant versus benign vertebral compression fractures: can we use bone SPECT as a substitute for MR imaging? Nucl Med Commun 2011;32(3):192–198
[27] Anselmetti GC, Bonaldi G, Carpeggiani P, Manfrè L, Masala S, Muto M. Vertebral augmentation: 7 years experience. Acta Neurochir Suppl (Wien) 2011;108:147–161
[28] Gangi A, Guth S, Imbert JP, Marin H, Dietemann JL. Percutaneous vertebroplasty: indications, technique, and results. Radiographics 2003;23(2):e10
[29] Kallmes DF, Jensen ME. Percutaneous vertebroplasty. Radiology 2003;229(1):27–36
[30] McGraw JK, Cardella J, Barr JD, et al; Society of Interventional Radiology Standards of Practice Committee. Society of Interventional Radiology quality improvement guidelines for percutaneous vertebroplasty. J Vasc Interv Radiol 2003;14(9 Pt 2):S311–S315
[31] Peh WC, Gilula LA. Percutaneous vertebroplasty: indications, contraindications, and technique. Br J Radiol 2003;76(901):69–75
[32] Lee MJ, Dumonski M, Cahill P, Stanley T, Park D, Singh K. Percutaneous treatment of vertebral compression fractures: a meta-analysis of complications. Spine 2009;34(11):1228–1232
[33] Nieuwenhuijse MJ, Putter H, van Erkel AR, Dijkstra PD. New vertebral fractures after percutaneous vertebroplasty for painful osteoporotic vertebral compression fractures: a clustered analysis and the relevance of intradiskal cement leakage. Radiology 2013;266(3):862–870
[34] Jacobson RE, Palea O, Granville M. Progression of vertebral compression fractures after previous vertebral augmentation: technical reasons for recurrent fractures in a previously treated vertebra. Cureus 2017;9(10):e1776
[35] Lee DG, Park CK, Park CJ, Lee DC, Hwang JH. Analysis of Risk Factors Causing New Symptomatic Vertebral Compression Fractures After Percutaneous Vertebroplasty for Painful Osteoporotic Vertebral Compression Fractures: A 4-year Follow-up. J Spinal Disord Tech 2015;28(10):E578–E583
[36] Rao RD, Singrakhia MD. Painful osteoporotic vertebral fracture. Pathogenesis, evaluation, and roles of vertebroplasty and kyphoplasty in its management. J Bone Joint Surg Am 2003;85(10):2010–2022
[37] Yuan WH, Hsu HC, Lai KL. Vertebroplasty and balloon kyphoplasty versus conservative treatment for osteoporotic vertebral compression fractures: A meta-analysis. Medicine (Baltimore) 2016;95(31):e4491
[38] Nieto-Iglesias C, Andrés-Nieto I, Peces-García E, et al. Vertebroplasty and kyphoplasty: techniques, complications, and troubleshooting. Tech Reg Anesth Pain Manage 2014;18:40–48
[39] Yi X, Lu H, Tian F, et al. Recompression in new levels after percutaneous vertebroplasty and kyphoplasty compared with conservative treatment. Arch Orthop Trauma Surg 2014;134(1):21–30
[40] Papanastassiou ID, Phillips FM, Van Meirhaeghe J, et al. Comparing effects of kyphoplasty, vertebroplasty, and non-surgical management in a systematic review of randomized and non-randomized controlled studies. Eur Spine J 2012;21(9):1826–1843
[41] Hussein MA, Vrionis FD, Allison R, et al; International Myeloma Working Group. The role of vertebral augmentation in multiple myeloma: International Myeloma Working Group Consensus Statement. Leukemia 2008;22(8): 1479–1484