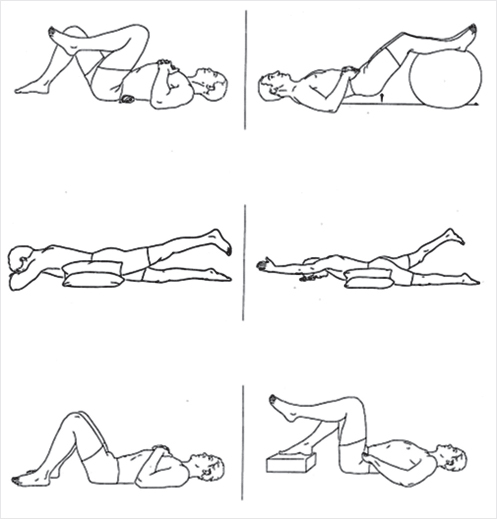
Fig. 26.1 Extension back and core strengthening exercises.
Summary
Vertebral compression fractures (VCFs) carry with them a known adverse effect on the patient’s abilities to carry out their normal activities of daily life. The morbidities associated with VCFs are well known and have been recorded in several different publications. Most of these morbidities result from immobility and prolonged periods of bed rest. The goal of vertebral augmentation and the therapy that follows is pain control and prompt return to more normal physical activity. Treatment of painful VCFs with vertebral augmentation has been shown to reduce morbidity and mortality and an appropriate rehabilitation care plan can improve the patient’s strength, posture, and balance and enhance the chances of an optimal treatment outcome. Physical exercise programs have been shown to maintain hip and spine bone mineral density and to reduce the frequency of falls. Certain rehabilitation regimens have been developed to optimize reduce falls, decrease pain from VCFs, and to reduce the chances of getting additional VCFs. These programs use a combination of weight-bearing exercise, extensor muscle strengthening, and balance training to accomplish the desired outcomes. It is important to begin the rehabilitation program as soon as possible after vertebral augmentation and a life-long adherence to an exercise program can, and has been shown to, be beneficial for increasing bone mineral density and for preventing additional VCFs.
Keywords: rehabilitation, morbidity, physical therapy, exercise program, core muscle strengthening, extensor training
VCFs due to osteoporosis are associated with pain, loss of function, impaired quality of life, and increased morbidity and mortality.1–4 Multiple studies published over the past decades have provided insight into the population-level morbidity associated with VCF in the United States.5 These include large reviews of the Nationwide Inpatient Sample, reviews of data from the Centers for Medicare and Medicaid Services, and data from the American College of Surgeons National Surgical Quality Improvement Program database.6–10 These investigations have identified significant rates of deep vein thrombosis (0.7–6.6%), pulmonary embolism (0.4–1.9%), pneumonia (3.1–13.0%), and decubitus ulcers (1.1–4.4%), regardless of treatment type. Most of these complications are in part a result of prolonged periods of bed rest. Thus, the importance of mobilizing the patient is paramount and must not be overlooked.
The goals of management with vertebroplasty and balloon kyphoplasty are pain control, prevention of spinal deformity, and functional restoration. Vertebral augmentation reduces pain without reliance on narcotics alone, allowing for early and increased mobility.11,12 It has been shown to reduce morbidity and mortality compared with conservative care.1,6 Management does not cease here, as the patient still needs to improve strength, correct posture, and enhance balance to increase independence and prevent further progression. This is accomplished through physical therapy and rehabilitation.
The protective effects of stronger back muscles on the spine has been highlighted as necessary in a guideline on the management of osteoporosis and postmenopausal women at risk for osteoporosis.13 Several studies have demonstrated that physical exercise programs maintain spine and hip bone mineral density (BMD) as well as decrease the frequency of falls.14–16 Recent consensus guidelines recommend that individuals with vertebral osteoporosis should engage in a multicomponent exercise program that includes progressive resistance training, in combination with mobility and balance training, and guidance on safe movements.15,17,18 High-risk individuals benefit from improved muscle strength in the back, legs, upper arms and core, and enhanced posture, balance, and coordination.19 Exercises for lower extremity muscles should focus on every major group around each joint. Back strengthening and postural exercises will reduce forward head posture, improve shoulder range of motion and trunk stability, and reduce vertebral fractures over time.20 Elbow extensor strength also facilitates transfers by moving the body with their arms and is related to reduced risk of nursing home admission after hip fracture.21
If an exercise program is to be prescribed for patients with spinal osteoporosis, a cautious approach is recommended. Regular weight-bearing exercise (e.g., walking 30–40 minutes per session, plus back and posture exercises for a few minutes, 3–4 days per week) should be advocated throughout life.20,22–24 Extension or isometric back and abdominal strengthening exercises seem most appropriate.25 ▶Fig. 26.1 demonstrates these exercises.
Table 26.1 Potential risks of prescribed exercise and preventive strategies
Potential risk |
Preventive strategy |
Fall |
Focus on balance training and progressive resistance training over walking or aerobic activity Close observation or monitoring during exercise program Optimize lighting and removing excess clutter in environment Review medications that may pose an increased risk for falls |
New spinal compression fracture |
Avoid forward flexion exercises Avoid excess weight-bearing or twisting movements of the spine (e.g., yoga) Avoid sports/activities involving spinal flexion (e.g., biking, gardening/yard work) Bend knees rather than spine to pick up objects |
Pain from osteoarthritis |
Use low-impact exercises Brief loading of bones with rest periods |
Pain from old compression fracture |
Rule out new fracture or progression of deformity if present Brace during exercise Adequate analgesia or local pain-relieving techniques (e.g., massage) |
Source: Adapted from Fiatarone 2014.53 |
|
Not all types of exercise are appropriate for these patients because of the fragility of their vertebrae. Potential risks of prescribed exercise and preventive strategies are summarized in ▶Table 26.1. Exercises that place flexion forces on the vertebrae tend to cause an increased number of vertebral fractures in these patients. Excess weight and side bending exercises similarly need to be avoided. Yoga exercises have become a concern due to the extreme spinal flexions performed, including several patients in whom VCFs developed as a direct result of participating in this activity.26 Similarly, rowing, lifting weights with a flexed spine, bowling, sit-ups, house and yard work must also be avoided due to increased risk of vertebral wedge fractures.17,18 Additionally, high-impact activities and exercises that require rapid and/or loaded twisting, and explosive or abrupt actions, such as golf and racquet sports, are contraindicated for high-risk individuals.
Prolonged aerobic training, such as swimming and cycling, is beneficial to cardiovascular health but does not provide a stimulus to bone growth. Regular walking has also been shown in two meta-analyses as a single intervention having minimal or no effect on BMD in the lumbar spine.27,28 Trials have also found that prescription of fast or brisk walking programs may actually increase the rate of falls.29 The inclusion of walking training may not be a crucial feature of program design and therefore recommend that walking training be included in a program as long as it is not at the expense of balance training.30 The addition of a weighted vest would seem to add a missing component to walking as an intervention; however, a study did not find significant improvement in strength, physical function, bone turn-over, or health-related quality of life.31 Thus, despite the benefits of aerobic fitness, walking is insufficient to optimize bone health, has little or no effect on balance, and may increase risk of falls.
Studies on early postmenopausal women have shown that strength training leads to small yet significant changes in BMD. A meta-analysis of 16 trials including 699 subjects showed a 2% improvement in lumbar spine BMD in the group that exercised compared with the group that did not.14 Effects of exercise on BMD are modest, but a meta-analysis estimated that exercise reduces the 20-year risk of osteoporotic fracture in the lumbar spine by 10%.15 One study of the effect of strengthening exercises for back extensor muscles in healthy postmenopausal women demonstrated a significant increase in back extensor muscle strength and improvement of posture with reduction in kyphosis without association with BMD.32 Others depicted improvement in muscle strength and BMD of the lumbar spine in estrogen-deficient women.18,33
Subject compliance with prescribed exercise interventions presents a challenge. In 2- to 3-year controlled, randomized studies, the dropout rate was 34 to 41% in the exercise groups.29,34 Subjects who are not self-motivated may not continue with prescribed exercise programs. Sinaki et al20 looked at the long-term protective effect of stronger back muscles on the spine in 50 healthy white postmenopausal women, aged 58 to 75 years, 8 years after they had completed a 2-year randomized, controlled trial. In the trial, 27 subjects had performed progressive, resistive back-strengthening exercises for 2 years and 23 had served as controls. BMD, spine radiographs, back extensor strength, biochemical marker values, and level of physical activity were obtained for all subjects at baseline, at 2 years, and at 10 years. The difference in BMD, which was not significant between the two groups at baseline and 2-year follow-up, was significant at the 10-year follow-up. They also found that the relative risk for compression fracture was 2.7 times greater in the control group than in the back-exercise group at 10 years. This emphasizes the importance of life-long adherence to an exercise program.
The consensus seems to be that an exercise regimen is most beneficial if osteoporosis has been caused by a lack of physical activity.35 The concurrent decline in bone and muscle mass with aging is compounded with inactivity after a VCF.36 Likewise, there are varying degrees of fat infiltration and paraspinal muscle atrophy in other degenerative lumbar diseases.37–40 Thus, exercise is an integral part of both nonsurgical and postinterventional treatments for osteoporotic VCFs.
The rehabilitation process following a VCF is sequential from the acute to the subacute phase followed by long-term care.41 During the acute stage, evidence shows that the patient should be mobilized out of bed as soon as possible.42,43 The clinician may begin with educating the patient on the correct positions to maintain in bed. Patients can begin doing exercises of the limbs that don’t require any mobilization to avoid rigidity and to reduce the muscular atrophy. Next, focus on gradually advancing to sitting on the edge of the bed, transferring, and ultimately different degrees of weight-bearing either in a chair or standing with or without aid of a walker. Further advancement is done through ambulation with either one- or two-person assistance or with different assistive devices. This stage is where the use of a brace may be beneficial. During the 2 months after the acute vertebral fracture, exercises should avoid intensive muscular strengthening and instead focus on relaxing exercises, maintaining mobility of the major joints, and breathing exercises. More intensive rehabilitation can start generally during 8 to 12 weeks from the acute event depending on patient’s level of pain and their imaging findings. The rehabilitation program includes back-extensor muscle exercises, which decrease the kyphotic posture that can predispose to back pain and to a higher risk of falls with subsequent fractures,44 and proprioceptive training to improve patient balance.45 The re-conditioning phase starts with removal of the vertebral brace, resumption of normal activities, and with the establishment of life-long regular weight-bearing exercise.46
Rehabilitation after vertebral augmentation for compression fractures should be employed to improve the patient’s strength and to reduce their pain, as well as to establish an optimized routine care habit. Data shows that 41 to 67% of new vertebral fractures occur at level adjacent to the augmented vertebra.47–50 Subsequent VCFs in patients affected by osteoporosis may not be a complication of the procedure itself but rather is part of the natural history. Physical therapy not only aids in patient recovery from the vertebral fracture, but also helps in deterring the long-term progression of the disease.
In a retrospective study that looked specifically at rehabilitation following vertebroplasty, a reduced incidence of vertebral refracture rate was demonstrated.51 Analysis of the refracture data showed that 75% of patients in the vertebroplasty group had a refracture within 12 months compared with 35% of patients in the vertebroplasty plus rehabilitation program. The median time before refracture also differed significantly between vertebroplasty only and vertebroplasty plus rehab groups with time to refracture of 4.5 months and 20.4 months, respectively.
Another study involved a single center that performed a prospective randomized control trial looking at the clinical benefit of a 2-year systematic exercise program following vertebroplasty.52 Systematic back muscle exercises resulted in a significant advantage in both the Oswestry Disability Index (ODI) as well as the visual analogue scale (VAS). The first significant difference was discovered 6 months postoperatively using the ODI. From then on, the clinical outcomes between the two groups were observed to gradually separate with the patients on the exercise program doing progressively better. There were increasingly significant differences of both VAS and ODI at 1 and 2-year follow-ups. These findings suggested that short-term clinical outcomes are not only maintained but enhanced in the long-term by adherence to a supplementary physical therapy intervention. By adopting systematic back muscle exercise, patients enjoyed a more favorable daily life and tended to have fewer problems while sitting and walking and had less back pain. Although it is time consuming, a systematic back muscle exercise program should be recognized as an important therapy for patients after vertebral augmentation.
Physical therapy and rehabilitation are indispensable to patients as part of routine anti-osteoporosis care, following a VCF, as well as postvertebral augmentation. Guidelines agree that regular weight-bearing and back-extensor exercises are optimal to increase strength and improve posture, and balance training is important to reduce falls. A cautious approach is required in high-risk individuals, and certain exercises such as flexion against resistance should be avoided. Walking programs and aerobic activities do not provide the same benefit as weight-bearing workouts and may increase the risk of falls especially in otherwise sedentary patients. Mobilization is key to prevent the morbidity and mortality associated with prolonged bed rest, and improved mobility is commonly the scenario for any patient after undergoing vertebral augmentation for a painful VCF. Physical therapy programs do not end with hospital discharge or with the completion of inpatient rehabilitation as benefits from regular exercise appear to increase over time and should be considered a life-long prescription.
[1] Edidin AA, Ong KL, Lau E, Kurtz SM. Morbidity and mortality after vertebral fractures: comparison of vertebral augmentation and nonoperative management in the medicare population. Spine 2015;40(15):1228–1241
[2] Edidin AA, Ong KL, Lau E, Kurtz SM. Life expectancy following diagnosis of a vertebral compression fracture. Osteoporos Int 2013;24(2):451–458
[3] Demers-Lavelle E, Cheney R, Lavelle W. Mortality prediction in a vertebral compression fracture population: the ASA physical status score versus the Charlson Comorbidity Index. Int J Spine Surg 2015;Cci:1–8
[4] Schlaich C, Minne HW, Bruckner T, et al. Reduced pulmonary function in patients with spinal osteoporotic fractures. Osteoporos Int 1998;8(3):261–267
[5] Goldstein CL, Chutkan NB, Choma TJ, Orr RD. Management of the elderly with vertebral compression fractures. Neurosurgery 2015;77(4, Suppl 4): S33–S45
[6] Chen AT, Cohen DB, Skolasky RL. Impact of nonoperative treatment, vertebroplasty, and kyphoplasty on survival and morbidity after vertebral compression fracture in the medicare population. J Bone Joint Surg Am 2013;95(19): 1729–1736
[7] McCullough BJ, Comstock BA, Deyo RA, Kreuter W, Jarvik JG. Major medical outcomes with spinal augmentation vs conservative therapy. JAMA Intern Med 2013;173(16):1514–1521
[8] Toy JO, Basques BA, Grauer JN. Morbidity, mortality, and readmission after vertebral augmentation: analysis of 850 patients from the American College of Surgeons National Surgical Quality Improvement Program database. Spine 2014;39(23):1943–1949
[9] Goz V, Errico TJ, Weinreb JH, et al. Vertebroplasty and kyphoplasty: national outcomes and trends in utilization from 2005 through 2010. Spine J 2015;15(5):959–965
[10] Zampini JM, White AP, McGuire KJ. Comparison of 5766 vertebral compression fractures treated with or without kyphoplasty. Clin Orthop Relat Res 2010;468(7):1773–1780
[11] Ledlie JT, Renfro M. Balloon kyphoplasty: one-year outcomes in vertebral body height restoration, chronic pain, and activity levels. J Neurosurg 2003;98(1, Suppl):36–42
[12] Klazen CAH, Lohle PNM, de Vries J, et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet 2010;376(9746):1085–1092
[13] Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2016. Endocr Pract 2016;22(Suppl 4):1–42
[14] Kelley GA, Kelley KS, Tran ZV. Exercise and lumbar spine bone mineral density in postmenopausal women: a meta-analysis of individual patient data. J Gerontol A Biol Sci Med Sci 2002;57(9):M599–M604
[15] Kelley GA, Kelley KS. Efficacy of resistance exercise on lumbar spine and femoral neck bone mineral density in premenopausal women: a meta-analysis of individual patient data. J Womens Health (Larchmt) 2004;13(3):293–300
[16] Varahra A, Rodrigues IB, MacDermid JC, Bryant D, Birmingham T. Exercise to improve functional outcomes in persons with osteoporosis: a systematic review and meta-analysis. Osteoporos Int 2018;29(2):265–286
[17] Beck BR, Daly RM, Singh MAF, Taaffe DR. Exercise and Sports Science Australia (ESSA) position statement on exercise prescription for the prevention and management of osteoporosis. J Sci Med Sport 2017;20(5):438–445
[18] Nikander R, Sievänen H, Heinonen A, Daly RM, Uusi-Rasi K, Kannus P. Targeted exercise against osteoporosis: a systematic review and meta-analysis for optimising bone strength throughout life. BMC Med 2010;8(1):47
[19] de Kam D, Smulders E, Weerdesteyn V, Smits-Engelsman BCM. Exercise interventions to reduce fall-related fractures and their risk factors in individuals with low bone density: a systematic review of randomized controlled trials. Osteoporos Int 2009;20(12):2111–2125
[20] Sinaki M, Itoi E, Wahner HW, et al. Stronger back muscles reduce the incidence of vertebral fractures: a prospective 10 year follow-up of postmenopausal women. Bone 2002;30(6):836–841
[21] Singh NA, Quine S, Clemson LM, et al. Effects of high-intensity progressive resistance training and targeted multidisciplinary treatment of frailty on mortality and nursing home admissions after hip fracture: a randomized controlled trial. J Am Med Dir Assoc 2012;13(1):24–30
[22] Sinaki M, Wahner HW, Offord KP, Hodgson SF. Efficacy of nonloading exercises in prevention of vertebral bone loss in postmenopausal women: a controlled trial. Mayo Clin Proc 1989;64(7):762–769
[23] Sinaki M. Critical appraisal of physical rehabilitation measures after osteoporotic vertebral fracture. Osteoporos Int 2003;14(9):773–779
[24] Sinaki M. Musculoskeletal challenges of osteoporosis. Aging (Milano) 1998;10(3):249–262
[25] Sinaki M, Mikkelsen BA. Postmenopausal spinal osteoporosis: flexion versus extension exercises. Arch Phys Med Rehabil 1984;65(10):593–596
[26] Sinaki M. Yoga spinal flexion positions and vertebral compression fracture in osteopenia or osteoporosis of spine: case series. Pain Pract 2013;13(1):68–75
[27] Ma D, Wu L, He Z. Effects of walking on the preservation of bone mineral density in perimenopausal and postmenopausal women: a systematic review and meta-analysis. Menopause 2013;20(11):1216–1226
[28] Martyn-St James M, Carroll S. Meta-analysis of walking for preservation of bone mineral density in postmenopausal women. Bone 2008;43(3):521–531
[29] Ebrahim S, Thompson PW, Baskaran V, Evans K. Randomized placebo-controlled trial of brisk walking in the prevention of postmenopausal osteoporosis. Age Ageing 1997;26(4):253–260
[30] Sherrington C, Tiedemann A, Fairhall N, Close JCT, Lord SR. Exercise to prevent falls in older adults: an updated meta-analysis and best practice recommendations. N S W Public Health Bull 2011;22(3–4):78–83
[31] Greendale GA, Salem GJ, Young JT, et al. A randomized trial of weighted vest use in ambulatory older adults: strength, performance, and quality of life outcomes. J Am Geriatr Soc 2000;48(3):305–311
[32] Mika A, Unnithan VB, Mika P. Differences in thoracic kyphosis and in back muscle strength in women with bone loss due to osteoporosis. Spine 2005;30(2):241–246
[33] Nelson ME, Fiatarone MA, Morganti CM, Trice I, Greenberg RA, Evans WJ. Effects of high-intensity strength training on multiple risk factors for osteoporotic fractures: a randomized controlled trial. JAMA 1994;272(24): 1909–1914
[34] Sinaki M, Wahner HW, Bergstralh EJ, et al. Three-year controlled, randomized trial of the effect of dose-specified loading and strengthening exercises on bone mineral density of spine and femur in nonathletic, physically active women. Bone 1996;19(3):233–244
[35] Giangregorio LM, McGill S, Wark JD, et al. Too fit to fracture: outcomes of a Delphi consensus process on physical activity and exercise recommendations for adults with osteoporosis with or without vertebral fractures. Osteoporos Int 2015;26(3):891–910
[36] Li Q, Sun J, Cui X, Jiang Z, Li T. Analysis of correlation between degeneration of lower lumbar paraspinal muscles and spinopelvic alignment in patients with osteoporotic vertebral compression fracture. J Back Musculoskeletal Rehabil 2017;30(6):1209–1214
[37] Ranson CA, Burnett AF, Kerslake R, Batt ME, O’Sullivan PB. An investigation into the use of MR imaging to determine the functional cross sectional area of lumbar paraspinal muscles. Eur Spine J 2006;15(6):764–773
[38] Mengiardi B, Schmid MR, Boos N, et al. Fat content of lumbar paraspinal muscles in patients with chronic low back pain and in asymptomatic volunteers: quantification with MR spectroscopy. Radiology 2006;240(3): 786–792
[39] Lee JC, Cha J-G, Kim Y, Kim Y-I, Shin B-J. Quantitative analysis of back muscle degeneration in the patients with the degenerative lumbar flat back using a digital image analysis: comparison with the normal controls. Spine 2008;33(3):318–325
[40] Hyun S-J, Bae C-W, Lee S-H, Rhim S-C. Fatty degeneration of paraspinal muscle in patients with the degenerative lumbar kyphosis. J Spinal Disord Tech 2013;1
[41] Pratelli E, Cinotti I, Pasquetti P. Rehabilitation in osteoporotic vertebral fractures. Clin Cases Miner Bone Metab 2010;7(1):45–47
[42] Rapado A. General management of vertebral fractures. Bone 1996; 18(3, Suppl):191S–196S
[43] Bonner FJ Jr, Sinaki M, Grabois M, et al. Health professional’s guide to rehabilitation of the patient with osteoporosis. Osteoporos Int 2003; 14(0, Suppl 2):S1–S22
[44] Itoi E, Sinaki M. Effect of back-strengthening exercise on posture in healthy women 49 to 65 years of age. Mayo Clin Proc 1994;69(11):1054–1059
[45] Sinaki M, Lynn SG. Reducing the risk of falls through proprioceptive dynamic posture training in osteoporotic women with kyphotic posturing: a randomized pilot study. Am J Phys Med Rehabil 2002;81(4):241–246
[46] Malmros B, Mortensen L, Jensen MB, Charles P. Positive effects of physiotherapy on chronic pain and performance in osteoporosis. Osteoporos Int 1998;8(3):215–221
[47] Sun G, Tang H, Li M, Liu X, Jin P, Li L. Analysis of risk factors of subsequent fractures after vertebroplasty. Eur Spine J 2014;23(6):1339–1345
[48] Trout AT, Kallmes DF, Kaufmann TJ. New fractures after vertebroplasty: adjacent fractures occur significantly sooner. AJNR Am J Neuroradiol 2006;27(1):217–223
[49] Hey HW, Tan JH, Tan CS, Tan HM, Lau PH, Hee HT. Subsequent vertebral fractures post cement augmentation of the thoracolumbar spine: does it correlate with level-specific bone mineral density scores? Spine 2015;40(24): 1903–1909
[50] Lindsay R, Cooper C, Hanley DA, Barton I, Broy SB, Flowers K. Risk of new vertebral fracture. 2017;285(3):1–4
[51] Huntoon EA, Schmidt CK, Sinaki M. Significantly fewer refractures after vertebroplasty in patients who engage in back-extensor-strengthening exercises. Mayo Clin Proc 2008;83(1):54–57
[52] Chen B-L, Zhong Y, Huang Y-L, et al. Systematic back muscle exercise after percutaneous vertebroplasty for spinal osteoporotic compression fracture patients: a randomized controlled trial. Clin Rehabil 2012;26(6): 483–492
[53] Fiatarone Singh MA. Exercise and bone health. In: Holick MF, Neeves JW, eds. Nutrition and Bone Health. 2nd ed. New York: Humana Press; 2014