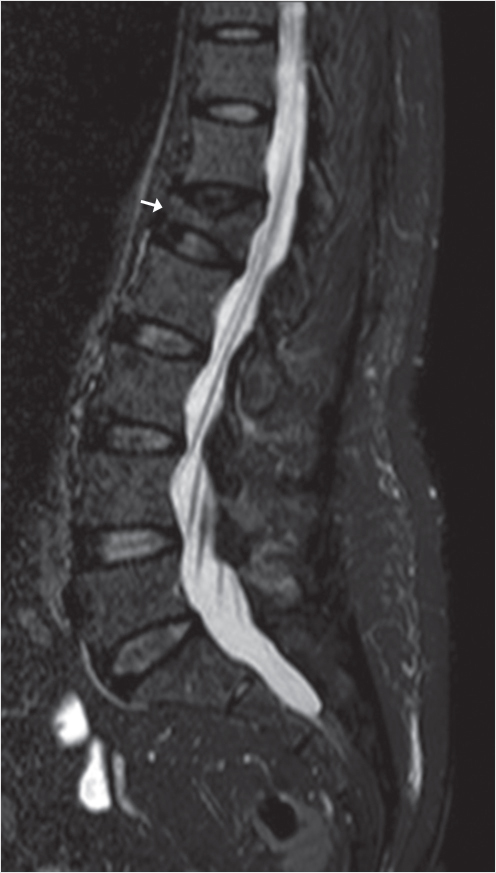
Fig. 28.1 Magnetic resonance imaging (MRI) depicting in short TI inversion recovery (STIR) sagittal sequence an L1 wedge vertebral fracture (white arrow), with no hyperintensity signal, hence no bone edema.
Summary
Vertebral compression fractures (VCFs) can be persistently painful even past the acute or subacute phase. Chronic fractures are defined as fractures older than six months. Osteonecrosis of the vertebral body is one of the more common conditions that can lead to bone resorption and loss of mechanical integrity necessitating treatment with vertebral augmentation. Chronic fractures can be treated with either vertebroplasty or kyphoplasty and numerous studies have shown this to be effective and to produce significant pain relief provided the patient’s pain is coming from the vertebral compression fracture. Although the presence of bone marrow edema tends to be predictive of pain relief after vertebral augmentation with a greater amount of bone marrow edema indicating the potential for greater pain relief, the absence of marrow edema does not mean that the patient will not improve after vertebral augmentation and patients have been shown to improve after treatment of chronic fractures irrespective of their appearance on magnetic resonance imaging (MRI).
Keywords: chronic, vertebral compression fractures, intravertebral cleft, bone marrow edema, osteonecrosis
Depending upon the duration of fractures, all vertebral fractures can be defined as acute (<6 weeks), subacute (6–24 weeks), and chronic (>24 weeks).1 The pathophysiology behind unhealed chronic, longer-lasting pain in these patients is multifactorial, including structural changes, nonunions, fibrous unions, osteoarthritis, and nerve irritation that results in chronic radiculopathy or complex regional pain syndrome.2 In the early era of vertebral augmentation, treating older fractures was controversial; however, numerous literature publications have proven efficacy of cement injection in these unhealed fractures as well.3–6 According to international reporting standards both painful chronic traumatic fracture with nonunion or internal cystic changes and painful fractures associated with osteonecrosis are included in the indications of vertebral augmentation.7,8
Preoperative imaging evaluation is a pre-requisite in chronic cases as well. Radiographs of the spine in anteroposterior and lateral projections can provide initial information concerning the number and the extent of vertebral collapse, but defining the levels of treatment by standard radiographs is inaccurate in both acute and chronic lesions.2,9 Similarly, in chronic vertebral fractures the usefulness of scintigraphy is controversial.2 On the other hand, MRI is governed by high sensitivity for bone marrow edema indicating osseous activity at the fracture site, irrespective of the fracture’s age. Timing of the fracture (acute or chronic) should not be confused with the presence of bone edema in short TI inversion recovery (STIR) sequence of MR examination. Both acute and unhealed chronic fractures can show bone edema (illustrated as increased signal intensity on the STIR sequence) as a sign of bone marrow activity. MRI with STIR and T1-weighted sequences should be used to verify the fracture’s age and healing status (acute vs. chronic, incompletely healed vs. consolidated) (▶Fig. 28.1).8 Tanigawa et al reported that the improvement after vertebral augmentation is related to the bone edema pattern illustrated in the pretherapeutic MRI (▶Fig. 28.2). Specifically according to this study patients with an extensive bone marrow edema pattern involving more than 50% of the vertebral body reported significantly greater clinical improvement than those without this pattern10 (▶Fig. 28.3).
Fig. 28.1 Magnetic resonance imaging (MRI) depicting in short TI inversion recovery (STIR) sagittal sequence an L1 wedge vertebral fracture (white arrow), with no hyperintensity signal, hence no bone edema.
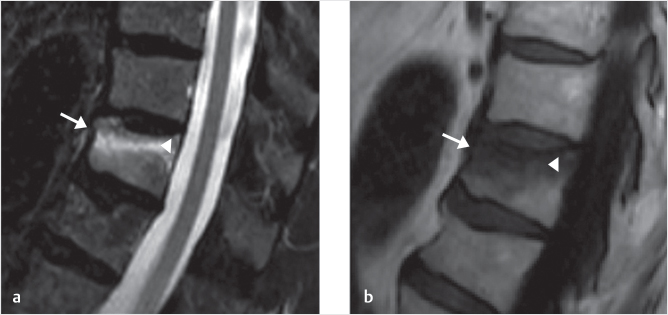
Fig. 28.2 Sagittal magnetic resonance (MR) image of vertebral body with short TI inversion recovery (STIR) (a) and T1W (b) sagittal sequences of a patient with T11 wedge fracture (white arrow in a and b). The vertebral edema (high in STIR and low signal in T1 as is indicated by white arrowheads in both images) extends through less than 50% of the vertebral body.
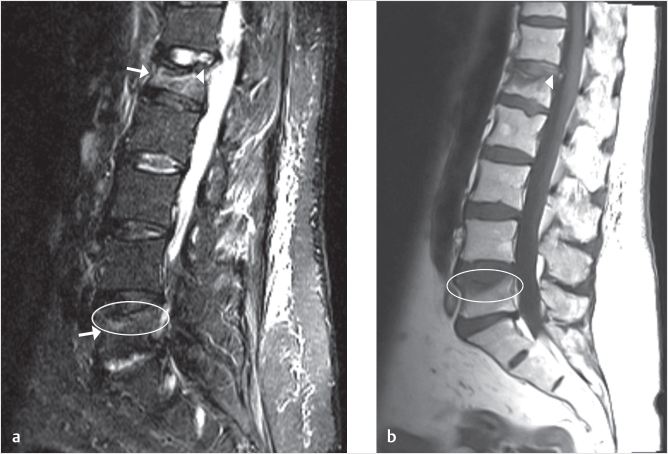
Fig. 28.3 Sagittal magnetic resonance imaging (MRI) of a patient consulting for low back pain. On short TI inversion recovery (STIR) there are two fractures of the upper end plate, one in L1 and one in L5 (white arrows in a). The L1 fracture has bone edema in more than 50% of the vertebral body (high signal in STIR and low in T1 as indicated by the white arrowheads in a and b) and may be clinically more painful than the L5 fracture, which has less than 50% bone edema (white ovals in a and b).
Vertebral body osteonecrosis is characterized by cellular death and bone resorption that result in mechanical insufficiency and vertebral collapse (▶Fig. 28.4). It can be idiopathic or secondary to trauma, cytotoxicity, and genetic factors.11–13 The process of osteonecrosis and subsequent rapid collapse of a vertebral body has been given the eponymous name Kummell disease after the German surgeon Hermann Kummell who first described this condition in 1891. The pathognomonic sign of vertebral osteonecrosis is the intravertebral vacuum sign that may contain gas, fluid, or both.13 MRI cannot easily distinguish between gas and compact bone, as both appear as low signal intensity areas. In case of suspicion of a gas pocket, CT imaging can easily detect the osteonecrotic gas cavity (▶Fig. 28.5). The literature examination of vertebral osteonecrosis is limited and inconsistent with substantial overlap with cases of nonunion, fibrous union, and pseudoarthrosis.14 The most common reported risk factors include low bone density and the use of glucocorticoids but many factors may work in combination. Recently, vertebral osteonecrosis was classified into four stages based upon radiological findings and sagittal alignment:13
• 0: Theoretical phase.
• 1: Early phase.
• 2: Instability phase.
• 3: Fixed deformity phase.
According to this classification proposed by Formica et al, stage 1 is managed with nonsurgical management (NSM) as opposed to stages 2 and 3 which require different therapeutic approaches according to local and global sagittal alignment.13 It is evident that the treatment of vertebral osteonecrosis should be adjusted according to symptoms and disability, neurological status, comorbidities, and surgical risk.
A chronic fracture can affect a whole spine segment by creating a degenerative cascade phenomenon which implicates all adjacent structures. This includes disk degeneration and herniation, facet osteoarthritis, nerve irritation associated with foraminal stenosis, muscle atrophy, ligament strain and sprain, Baastrup disease, scoliosis, and spinal stenosis. These secondary effects from the initial deformity can also be pain generators, thus creating a situation with complex pain symptoms. Augmentation techniques aim to provide structural support by forming an intraosseous cast and as such can help the pain and the structural deformity associated with the fracture. In order therefore to have a clinically successful treatment it is very important to differentiate the pain associated with the nonhealing fracture from the pain related to the secondary pathology. Treating a complex pain syndrome, although outside of the scope of this book, is as critical as treating the painful fracture itself and in most cases multiple treatments will work in a complementary manner.
Fig. 28.4 L3 vertebral fracture in short TI inversion recovery (STIR) sagittal sequence illustrating a fluid-filled cleft (black arrow), just below the superior end plate. The edema (high signal in STIR as indicated by white oval) extends through the middle third to the anterior third of the vertebral body. Notice the bone marrow edema, which is characterized by its high intensity on STIR, has a lower signal than the fluid seen in the cleft (black arrow).
Numerous studies in the literature have proven the safety and efficacy of different vertebral augmentation techniques in the treatment of painful chronic fractures and vertebral osteonecrosis.15–23 Vertebroplasty has been reported to be an effective therapeutic technique for these cases but has also been reported to have an increased risk cement leakage and recurrent kyphosis.15–18 Balloon kyphoplasty has been similarly reported to be an effective technique for symptomatic chronic and osteonecrotic vertebrae with no reports of increased cement leakage or recurrent kyphosis.19,20 Comparative studies between these two techniques for vertebral osteonecrosis report similar clinical and radiological results as well as similar incidence of cement leakage.21,22 Recently, vertebral implants have been used with promising results for the treatment of vertebral osteonecrosis specifically an intravertebral expandable jack consisting of a central screw and of two deployable plates. This jack device known as the SpineJack has been applied in 19 patients with significant pain reduction and no complications.23
Studies have also reported the effectiveness of the treatment of chronic VCFs even with imaging findings showing no bone marrow edema or evidence of an unhealed fracture.2 Brown et al studied the outcomes of vertebroplasty in patients with chronic VCFs of more than 1 year old.2 They reported on 45 patients and recorded the imaging findings, changes in pain, and improvements in mobility up to 28 months and found that two-thirds of the patients did not have marrow edema on their preprocedural MRI examination. This preprocedure MRI exam results were correlated with the procedure outcomes and it was found that all of the 15 patients that had edema on their preprocedure MRI examination received clinical benefit with 40% of these patients achieving complete pain relief and the remainder experiencing substantial clinical improvement. Of the patients with no marrow edema 17% had complete resolution of pain, 63% were improved, and 20% were unchanged. None of these patients had worsening of their symptoms, and mobility was improved in 57%. Overall they found that 87% of the patients with VCFs older than 1 year received clinical benefit from vertebroplasty irrespective of the preprocedure MRI findings, and although all of the patients with bone marrow edema had clinical benefit, no direct correlation was seen between symptom resolution and the presence of edema on preprocedural MRI. They went on to conclude that the absence of abnormal marrow signal does not definitively predict the outcome of vertebroplasty in chronic fractures.2
Fig. 28.5 Thoracic spine imaging showing a hypointense area in T7 and T10 vertebral bodies (black arrows in a) as noted on the T1-weighted sagittal magnetic resonance (MR) image. The decreased signal in the T7 vertebral body remains hypointense on the T2-weighted image (white arrows in a and b). This area of decreased T1 and T2 signal was shown to be an air-filled cleft on a CT exam (area within the white circle in c). Four vertebral levels were augmented, to treat the two fractures, as well as to augment the osteoporotic vertebral bodies in between. The augmentation (white arrows in d) is best seen on the post-treatment CT.
In a study to analyze and compare the outcomes of vertebroplasty with unipedicular and bipedicular kyphoplasty for the treatment of VCFs, Bozkurt et al examined the changes in pain, function, and height restoration rates in 296 patients.24 There were 433 fractures treated with vertebral augmentation, with an average fracture age of 23.4 months from the onset of symptoms to the time of treatment. In this patient population with the mean fracture age of nearly 2 years, the mean height restoration was slightly over 24% in the vertebroplasty group and 37% in the bilateral kyphoplasty group, with pain and functional scores improving in all of the groups. In this patient population with chronic VCFs, the authors concluded that both vertebroplasty and kyphoplasty were effective in providing pain relief and improvement in functional capacity and showed a substantial amount of restoration in vertebral body height.24
In conclusion, vertebral augmentation techniques including vertebroplasty, balloon kyphoplasty, and vertebral implants can be considered safe and efficacious techniques for the treatment of symptomatic chronic vertebral fractures. The diagnostic criteria for the treatment of chronic vertebral fractures are no different than the criteria for treatment of acute or subacute fractures with the patient presenting with substantial pain and/or functional debilitation and the presence of a vertebral fracture by imaging that corresponds with the pain generator on physical exam. The goals for the treatment of all fractures regardless of acuity are pain reduction and improvement of functional capacity and quality of life by restoring the vertebral body stability and correcting structural spine deformities with the least invasive technique available.
[1] Rad AE, Kallmes DF. Correlation between preoperative pain duration and percutaneous vertebroplasty outcome. AJNR Am J Neuroradiol 2011;32(10):1842–1845
[2] Brown DB, Glaiberman CB, Gilula LA, Shimony JS. Correlation between preprocedural MRI findings and clinical outcomes in the treatment of chronic symptomatic vertebral compression fractures with percutaneous vertebroplasty. AJR Am J Roentgenol 2005;184(6):1951–1955
[3] Kaufmann TJ, Jensen ME, Schweickert PA, Marx WF, Kallmes DF. Age of fracture and clinical outcomes of percutaneous vertebroplasty. AJNR Am J Neuroradiol 2001;22(10):1860–1863
[4] Brown DB, Gilula LA, Sehgal M, Shimony JS. Treatment of chronic symptomatic vertebral compression fractures with percutaneous vertebroplasty. AJR Am J Roentgenol 2004;182(2):319–322
[5] Maynard AS, Jensen ME, Schweickert PA, Marx WF, Short JG, Kallmes DF. Value of bone scan imaging in predicting pain relief from percutaneous vertebroplasty in osteoporotic vertebral fractures. AJNR Am J Neuroradiol 2000;21(10):1807–1812
[6] Jensen ME, Dion JE. Percutaneous vertebroplasty in the treatment of osteoporotic compression fractures. Neuroimaging Clin N Am 2000;10(3):547–568
[7] Baerlocher MO, Saad WE, Dariushnia S, Barr JD, McGraw JK, Nikolic B; Society of Interventional Radiology Standards of Practice Committee. Quality improvement guidelines for percutaneous vertebroplasty. J Vasc Interv Radiol 2014;25(2):165–170
[8] Tsoumakidou G, Too CW, Koch G, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol 2017;40(3):331–342
[9] Stallmeyer MJB, Zoarski GH, Obuchowski AM. Optimizing patient selection in percutaneous vertebroplasty. J Vasc Interv Radiol 2003;14(6):683–696
[10] Tanigawa N, Komemushi A, Kariya S, et al. Percutaneous vertebroplasty: relationship between vertebral body bone marrow edema pattern on MR images and initial clinical response. Radiology 2006;239(1):195–200
[11] Shah KN, Racine J, Jones LC, Aaron RK. Pathophysiology and risk factors for osteonecrosis. Curr Rev Musculoskelet Med 2015;8(3):201–209
[12] Lafforgue P. Pathophysiology and natural history of avascular necrosis of bone. Joint Bone Spine 2006;73(5):500–507
[13] Formica M, Zanirato A, Cavagnaro L, et al. Vertebral body osteonecrosis: proposal of a treatment-oriented classification system. Eur Spine J 2018;27(Suppl 2): 190–197
[14] Formica M, Zanirato A, Cavagnaro L, et al. What is the current evidence on vertebral body osteonecrosis?: a systematic review of the literature. Asian Spine J 2018;12(3):586–599
[15] Hirsch JA, Reddy AS, Linfante I, Rachlin JR. Pseudo-Kümmel’s disease: a unique application for vertebroplasty. Pain Physician 2003;6(2):207–211
[16] Kim DY, Lee SH, Jang JS, Chung SK, Lee HY. Intravertebral vacuum phenomenon in osteoporotic compression fracture: report of 67 cases with quantitative evaluation of intravertebral instability. J Neurosurg 2004;100(1, Suppl Spine):24–31
[17] Cho SM, Heo DH, Cho YJ. Spontaneous migration of a polymethylmethacrylate mass after vertebroplasty in osteoporotic lumbar compression fracture with avascular osteonecrosis: a case report. Joint Bone Spine 2011;78(1):98–99
[18] Fang X, Yu F, Fu S, Song H. Intravertebral clefts in osteoporotic compression fractures of the spine: incidence, characteristics, and therapeutic efficacy. Int J Clin Exp Med 2015;8(9):16960–16968
[19] Huang Y, Peng M, He S, Tang X, Dai M, Tang C. Clinical efficacy of percutaneous kyphoplasty at the hyperextension position for the treatment of osteoporotic Kummell disease. Clin Spine Surg 2016;29(4):161–166
[20] Chen GD, Lu Q, Wang GL, et al. Percutaneous kyphoplasty for Kummell disease with severe spinal canal stenosis. Pain Physician 2015;18(6):E1021–E1028
[21] Zhang GQ, Gao YZ, Chen SL, Ding S, Gao K, Wang HQ. Comparison of percutaneous vertebroplasty and percutaneous kyphoplasty for the management of Kümmell’s disease: a retrospective study. Indian J Orthop 2015;49(6):577–582
[22] Wu AM, Ni WF, Weng W, Chi YL, Xu HZ, Wang XY. Outcomes of percutaneous kyphoplasty in patients with intravertebral vacuum cleft. Acta Orthop Belg 2012;78(6):790–795
[23] Premat K, Vande Perre S, Cormier É, et al. Vertebral augmentation with the SpineJack in chronic vertebral compression fractures with major kyphosis. Eur Radiol 2018;28(12):4985–4991
[24] Bozkurt M, Kahilogullari G, Ozdemir M, et al. Comparative analysis of vertebroplasty and kyphoplasty for osteoporotic vertebral compression fractures. Asian Spine J 2014;8(1):27–34