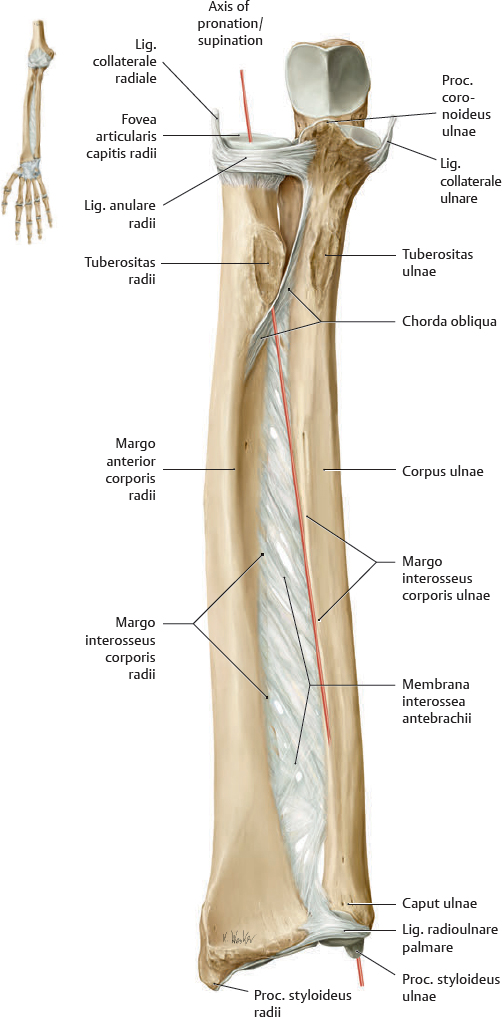
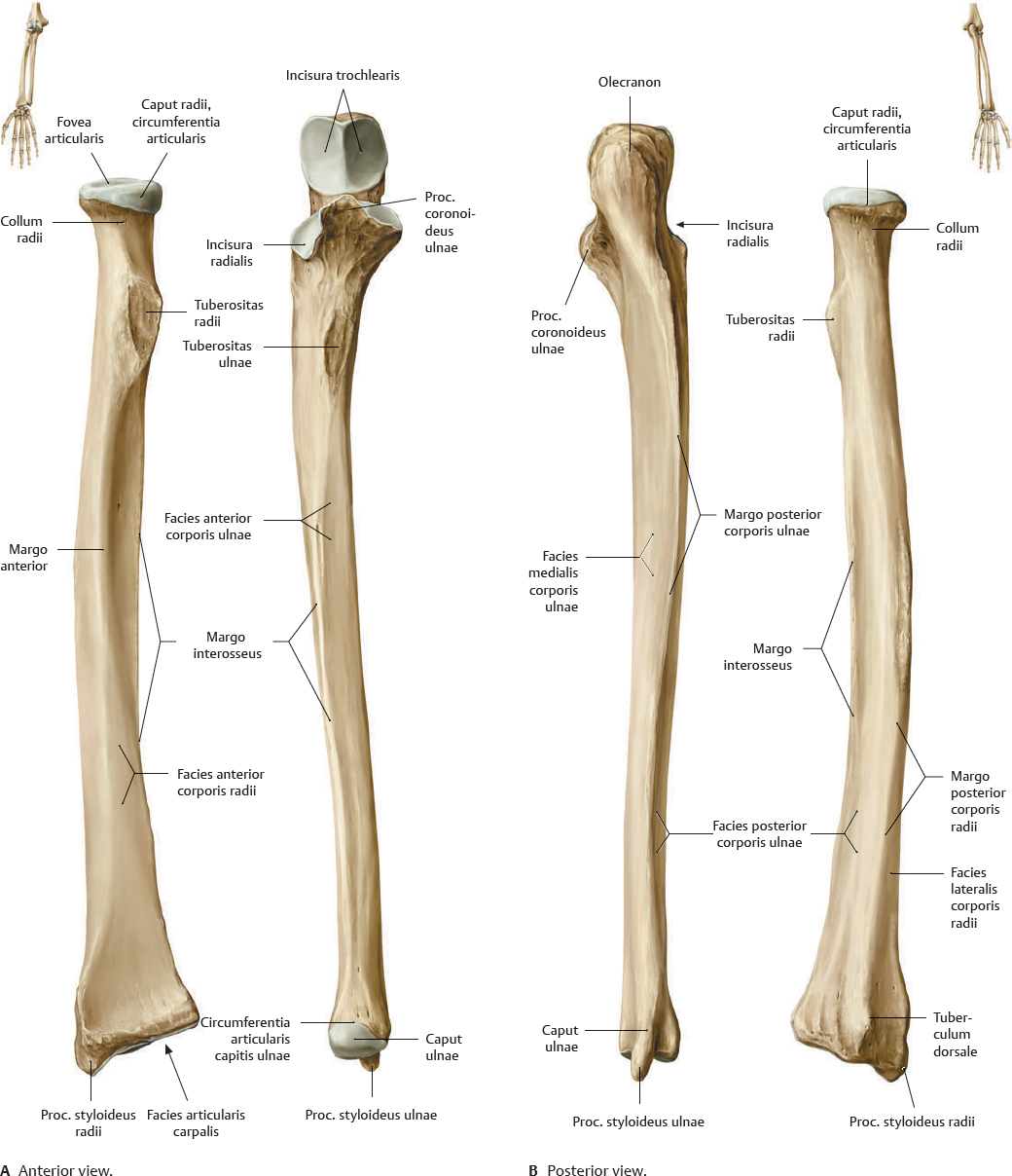
Fig. 26.1 Radius and ulna
Right forearm.
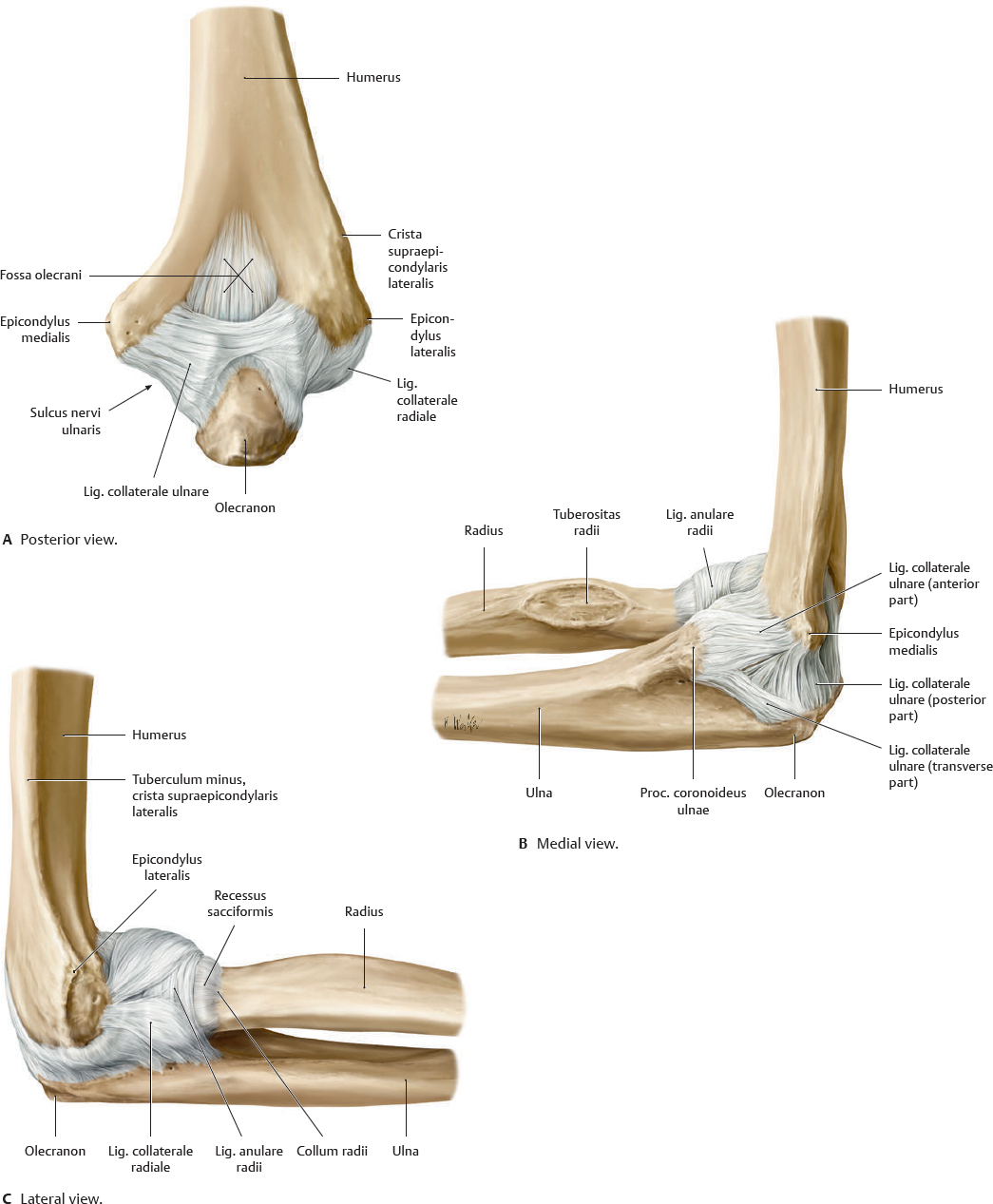
Fig. 26.2 Articulatio cubiti
Right limb. The elbow (cubitus) consists of three joints between the humerus, ulna, and radius: the artt. humeroulnaris, humeroradialis, and art. radioulnaris proximalis.
Assessing elbow injuries
The fat pads between the membrana fibrosa and membrana synovialis are part of the normal anatomy of the art. cubiti. The anterior pad is most readily seen on a sagittal MRI while the posterior pad is often hidden within the bony fossa (see Figs. 26.3 and 29.11). With an effusion of the joint space, the inferior edge of the anterior pad appears concave as it gets pushed superiorly by the intra-articular fluid. This causes the pad to resemble the shape of a ship's sail, thus creating a characteristic “sail sign.” The alignment of the prominences in the elbow also aids in the identification of fractures and dislocations.

Subluxation of the caput radii (nursemaid's elbow)
A common and painful injury of small children occurs when the arm is jerked upward with the forearm pronated, tearing the lig. anulare from its loose attachment on the collum radii. As the immature caput radii slips out of the socket, the ligament may become trapped between the caput radii and the capitulum humeri. Supinating the forearm and flexing the elbow usually returns the caput radii to the normal position.

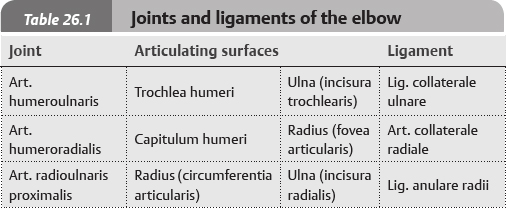
 The artt. radioulnares proximales and distales function together to enable pronation and supination movements of the hand. The joints are functionally linked by the membrana interossea antebrachii. The axis for pronation and supination runs obliquely from the center of the capitulum humeri through the center of the fovea articularis capitis radii down to the proc. styloideus ulnae.
The artt. radioulnares proximales and distales function together to enable pronation and supination movements of the hand. The joints are functionally linked by the membrana interossea antebrachii. The axis for pronation and supination runs obliquely from the center of the capitulum humeri through the center of the fovea articularis capitis radii down to the proc. styloideus ulnae.
Fig. 26.9 Rotation of articulatio radioulnaris distalis
Right forearm, distal view of articular surfaces of radius and ulna. The dorsal and palmar radioulnar ligaments stabilize the art. radioulnaris distalis.
Radius fracture
Falls onto the outstretched arm often result in fractures of the distal radius. In a Colles’ fracture, the distal fragment is tilted dorsally.

Fig. 26.10 Anterior muscles of the forearm: Dissection
Right forearm, anterior view. Muscle origins are shown in red, insertions in blue.
Fig. 26.11 Posterior muscles of the forearm: Dissection
Right forearm, posterior view. Muscle origins are shown in red, insertions in blue.
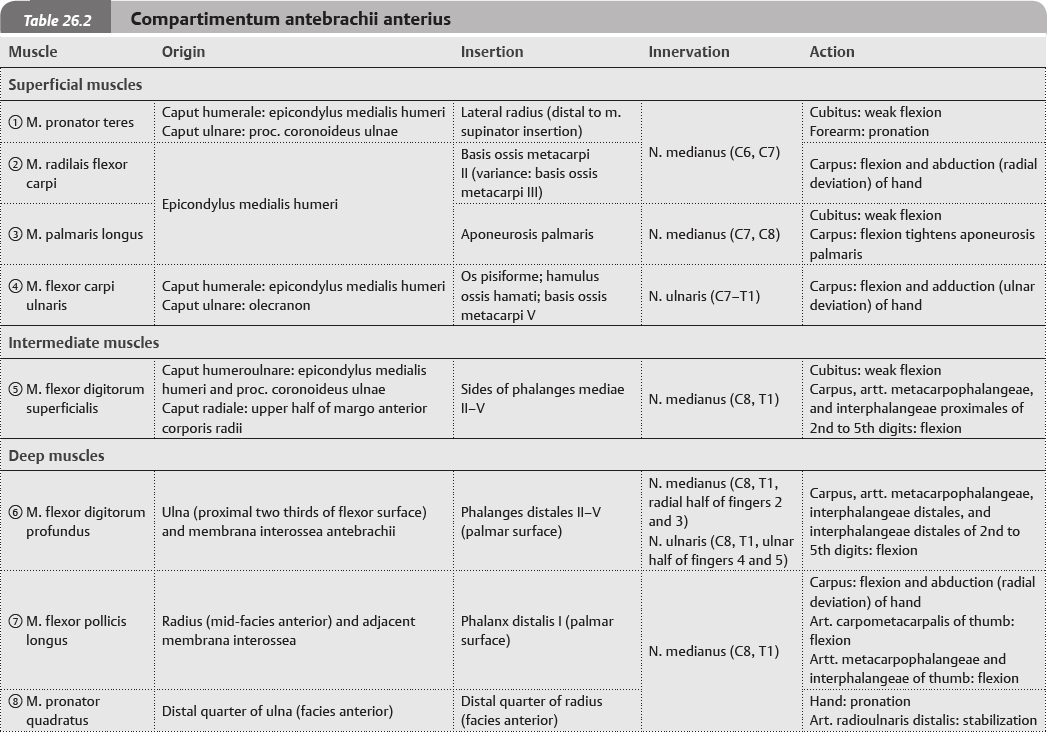
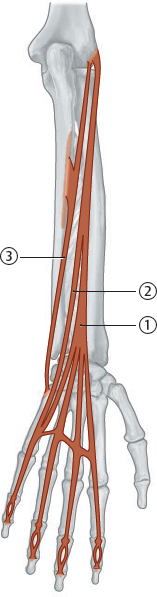
Fig. 26.13 Compartimentum antebrachii anterius: Superficial and intermediate muscles
Right forearm, anterior view.
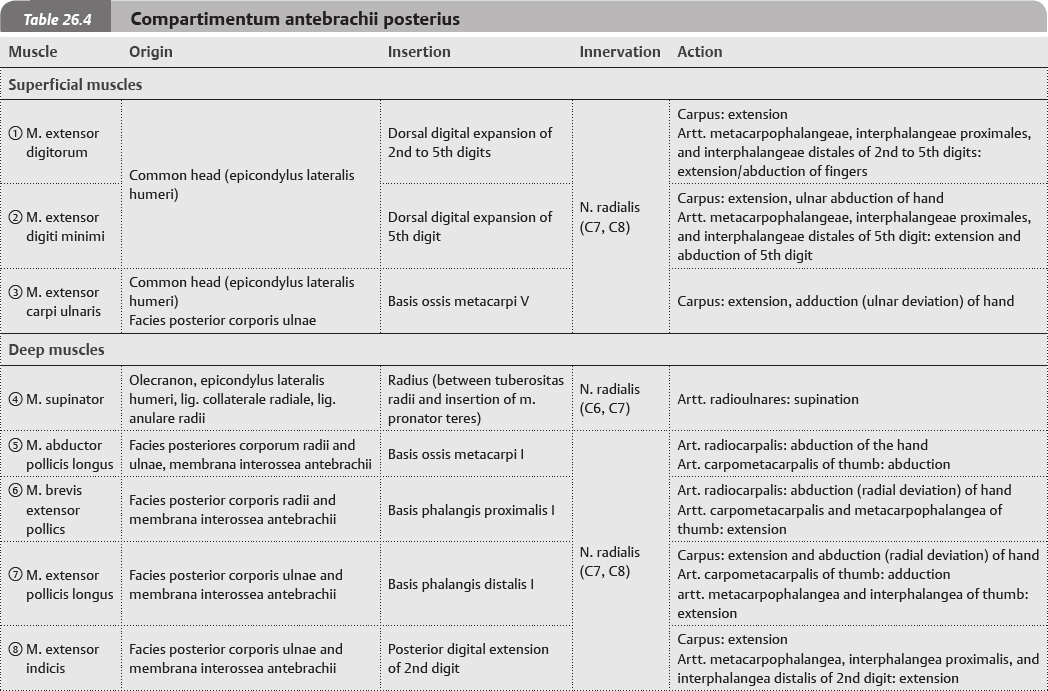
Fig. 26.15 Compartimentum antebrachii posterius: Radialis muscles
Right forearm, posterior view, schematic.
Lateral epicondylitis
Lateral epicondylitis, or tennis elbow, involves the extensor muscles and tendons of the forearm that attach on the epicondylus lateralis humeri. The tendon most commonly involved is that of the m. radialis brevis extensor carpi, a muscle that helps stabilize the carpus when the cubitus is extended. When the m. radialis brevis extensor carpi is weakened from overuse, microscopic tears form in the tendon where it attaches to the epicondylus lateralis. This leads to inflammation and pain. There is some evidence that the inflammation can extend back along the tendon to the periosteum of the epicondylus lateralis.
Athletes are not the only people who get tennis elbow and are actually in the minority—leading some to suggest the condition be referred to as “lateral elbow syndrome”. Workers whose activities require repetitive and vigorous use of the forearm muscles, such as common to painters, plumbers, and carpenters, are particularly prone to developing this pathology. Studies show a high incidence also among auto workers, cooks, and butchers. Common signs and symptoms of tennis elbow include pain with wrist extension against resistance, point tenderness or burning on the epicondylus lateralis, and weak grip strength. Symptoms are intensified with forearm activity.
Fig. 26.17 Compartimentum antebrachii posterius: Superficial muscles
Right forearm, posterior view, schematic.
Fig. 26.18 Compartimentum antebrachii posterius: Deep muscles
Right forearm, posterior view, schematic.



 Clinical box 26.1
Clinical box 26.1