Photo 30: Gunshot wound to the chest. A wound of this type would result in a hemothorax. (Photo courtesy of the Georgia Bureau of Investigation/Photo Lab.)
The lung is elastic tissue that can accommodate temporary compression. Due to its elastic nature, the lung can sustain an amazing amount of trauma. Current literature on war-related chest wounds suggests that more than 85 percent of penetrating and perforating wounds of the chest can be managed with closed-tube thoracostomy. 1 The remaining percentage of wounds would necessitate the opening of the chest in order to surgically repair damaged structures that continue to hemorrhage or leak air.
Whether chest wounds are the result of blunt or penetrating trauma, they can lead to the life-endangering complications of tension pneumothorax, hemothorax, and hemopneumothorax. These types of developing complications require prompt intervention by relieving pressure in the tension pneumothorax or draining blood in the hemothorax. Without aggressive care, the patient’s condition will deteriorate quickly as his respiratory and circulatory functions are compromised. Tension and hemothoraxsis are emergencies in which minutes count. In these instances, needle chest decompression and insertion of a chest tube in the field can make the life-or-death difference for a patient who has little hope for prompt transport to a hospital.
MECHANICS OF THE INJURY
The pleura is a thin layer of tissue that lines the inner side of the thoracic cavity as well as the lung itself. In the undamaged chest/lung, there is no space between the pleural layers because they ride close to one another. In the damaged chest/lung, air may flow between the two pleural layers, creating an unnatural space. As this space grows, it leads to a condition known as a pneumothorax. If bleeding is present, blood will accumulate between the two pleural linings, resulting in a hemothorax (Photo 30). When there is an escape of both air and blood into this “pleural space,” a hemopneumothorax is present. A tension pneumothorax, which develops from either blunt or penetrating trauma to the lung, creates a one-way valve which allows air to enter the pleural space. The affected lung is soon collapsed, and the mediastinum is pushed in the opposite direction, resulting in impaired circulatory function and eventual im - pinge ment upon the remaining good lung (Ill. 46).
Photo 30: Gunshot wound to the chest. A wound of this type would result in a hemothorax. (Photo courtesy of the Georgia Bureau of Investigation/Photo Lab.)
A hemothorax develops as lacerated pulmonary vessels spill blood from the injured lung into the pleural space. The severity of a hemothorax is brought into greater clarity when one considers that each thoracic cavity may contain up to 3 liters of blood. 2 As blood fills the pleural space, the injured lung is soon displaced and collapsed. Circulation through the inferior and superior vena cavae, along with the respiratory functions of the uninjured lung, are eventually compromised by the growing pleural space. As more blood is lost into the pleural space, circulatory and respiratory functions deteriorate into a vicious cycle of shock and hypoxemia (Ill. 47).
NEEDLE CHEST DECOMPRESSION
An expedient technique for the relief of a tension pneumothorax is needle chest decompression. Needle chest decompression is a temporary measure requiring later replacement with a chest tube. When the patient exhibits signs and symptoms of a tension pneumothorax—with either marked respiratory distress, cyanosis, loss of consciousness, or loss of a radial pulse—a needle chest decompression is indicated. 3
The procedure is begun by the PHCP identifying the fifth or sixth intercostal space in the midaxillary line on the injured side; an alternate site is the second intercostal space in the
midclavicular line. 4 If a chest tube is on hand, it can be inserted in this second intercostal site in lieu of the needle. 5 After prepping the site with an antiseptic solution, a 14-gauge overthe- needle catheter (the same as used in IV therapy) is passed through a condom in order to make a one-way valve. The catheter is then inserted just over the top of the rib through the parietal pleura until air escapes. The needle is removed and the catheter is left in place until a chest tube can be inserted (Photo 31). After the procedure, the patient’s torso should be elevated 20 to 30 degrees to assist in the movement of the trapped air.
Photo 31: The PHCP is removing the needle while leaving the catheter in place through the condom. The condom will be unrolled to produce the one-way valve.
CHEST TUBE INSERTION
When chest trauma causes a symptomatic hemothorax, blood must be drained from the chest via a chest tube (Photo 32). Drainage of the hemorrhaged blood will have a positive effect on the patient’s respiratory efforts, it will help avoid development of a constricting peel from the forming blood clot, and it also will allow measurement of the rate of blood loss.
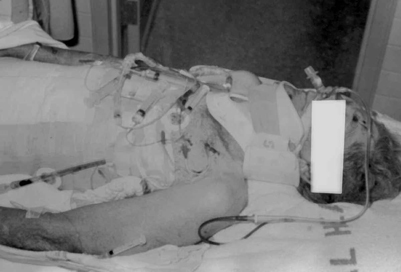
Photo 32: Chest tube in place on a patient who has suffered multiple trauma. Also note endotracheal tube and nasogastric tube in place. (Photo courtesy of Georgia Bureau of Investigation/Photo Lab.)
The two major considerations to be addressed prior to insertion of the chest tube are adequate anesthesia of the insertion site and proper tube placement. The procedure can be extremely painful, so injection of the site with Lidocaine is important. The diaphragm is often elevated on the side of the injury, thus possible penetration of the liver or spleen could occur if the chest tube is placed too low.
At the beginning of the procedure, the patient is placed on his back with the arm of his injured side placed under his head. A pillow is placed under his back to raise it slightly. The sixth intercostal space on the mid-axillary line is prepped with an antiseptic and the area is anesthetized. 6 The needle and syringe used for the injection of the Lidocaine can also be used to check tube placement by pushing it a little further into the chest cavity and aspirating hemorrhaged blood. If blood is not aspirated, the site is probably too low, and the PHCP is in danger of intra-abdominal placement of the chest tube.
Once the insertion site is verified, a 3 cm incision is made with a scalpel until fat is seen. The fat is spread by a clamp, exposing the intercostal muscles (Ill. 48). These muscles are also incised and spread open with a clamp, at which time blood and air should escape (Ill. 49).
Illustration 48: Exposing the intercostal muscles.
Illustration 49: The intercostal muscles being spread open with a clamp.
The chest tube is pushed into the pleural cavity between the jaws of the clamp about 10 cm, or at least until the drainage holes on the tube are within the pleural space (Ill. 50). A Foley catheter can be used in a makeshift approach (Photo 33). Once the chest tube is in proper position, it is connected to tubing that leads to a drainage bottle. Proper tube placement can be evaluated by monitoring the rise and fall of the water in the drainage bottle with each inspiration and expiration. If water does not rise and fall, or if no bubbles are noted, tube placement should be reevaluated.
Photo 33: Chest tube in the foreground. Foley catheter in the background. Note drainage holes in the tubes that are placed inside the chest.
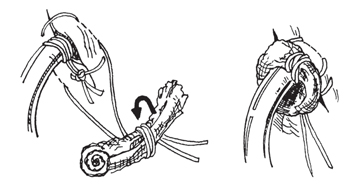
Illustration 51: Applying the stay suture.
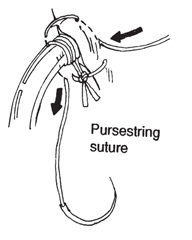
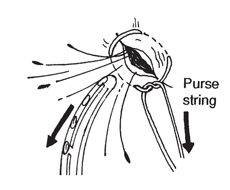
Illustration 52:Threading the purse-string suture.
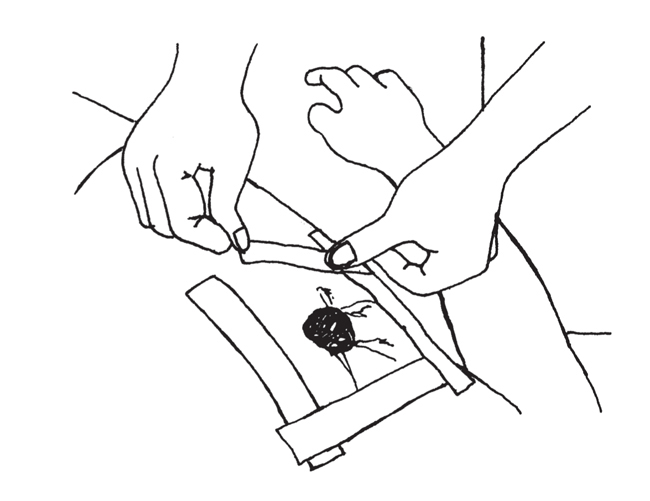
Illustration 53:Dressing the insertion site.
The chest tube is fastened to the outer chest wall with 3-0 size suture. To form an airtight seal, a stay suture is wrapped around the tube several times and drawn tight with another knot (Ill. 51). A purse-string suture is then threaded to ensure a seal when the chest tube is removed at a later date (Ill. 52). The extra suture from the purse string is wrapped around a 2 x 2 inch sponge and then wrapped around the tube to serve as a dressing (Ill. 53). The dressing is held down with tape.
THE DRAINAGE BOTTLE
The drainage bottle, which must lie below the patient in order to work, serves as a means to collect blood and fluids. More importantly, the drainage bottle and underwater seal take advantage of gravity as a means to effect drainage of the chest. Chest drainage is also assisted by exhalation, which pushes air and liquid out of the pleural space.
For the water seal (one-way valve) to function properly, the end of the tubing must be below the surface of the sterile water. The drainage tube should be just a little under the surface of the water (Ill. 54). If the tube is too deep as a result of collection buildup, resistance to air passage through the tube can prevent air escape, resulting in a pneumothorax, even with a “functioning” chest drain. A 20- to 30-degree elevation of the patient’s torso should help pool the blood and thereby facilitate drainage.
POST CHEST TUBE INSERTION ASSESSMENT
With fluid replacement and chest drainage, many pulmonary lacerations that do not directly involve a major vessel will heal on their own. Relief of the tension in the chest may be followed by hemorrhage from a vascular injury that can only be corrected by a surgeon opening the patient’s chest to stop the bleeding. If drainage from the chest is less than 150 ml per hour, there are no large or continuous air leaks, and there is no major damage to the trachea, esophagus, bronchial tree, or cardiovascular system, drainage and other supportive measures are probably adequate. 7 This is particularly true if the patient’s vital signs are stable.
REMOVAL OF THE CHEST TUBE
Once the lung has fully expanded and there have been no air leaks for 24 hours, the chest tube has been stopped up for 24 hours, or fluid output is less than 50 ml per day, the chest tube usually can be removed. 8
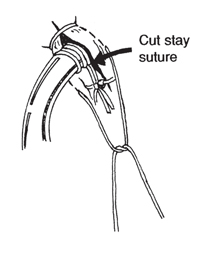
An X-ray of the chest is taken to ensure that the lung is fully inflated (it is also used to check tube placement), but unfortunately this important diagnostic tool is not often available for the PHCP. The purse string is unrolled, stay sutures are cut, and, while the patient holds a deep breath, the chest tube is pulled free and the purse string closed (Ills. 55 and 56). A dressing is then placed over the incision site. It is not a good practice to remove the chest tube in the field, and, if at all possible, it should be left in until the patient has reached a hospital.
Illustration 55: Stay suture cut.
Illustration 56:Chest tube removed and the purse-string struture closed.
COMPLICATIONS ASSOCIATED WITH NEEDLE
CHEST DECOMPRESSION
AND CHEST TUBE INSERTION
Needle chest decompression and chest tube insertion are not risk-free. Poor technique can easily contribute to the demise of the patient. Proper needle and tube placement, which will avoid lacerating the intercostal artery and vein that run around the inferior margin of each rib, is of particular concern. A needle or chest tube advanced too far into the chest can lacerate a variety of important structures. Poor patient assessment can lead to the creation of a pneumothorax by inappropriately initiating the procedures when they are not needed. And finally, during transport of the patient with a chest tube, it is not uncommon for the chest tube to be clamped off and removed from the water seal for ease of mobility. This practice should be avoided because the clamped-off tube can lead to a tension pneumothorax in the unhealed lung.
DRESSING THE CHEST WOUND
For needle chest decompression and chest tube drainage to function properly, the wound site (be it the result of a bullet or a knife) must be dressed with an occlusive dressing. The immediate application of an occlusive dressing along with other basic life-support procedures (i.e., oxygen and IV therapy) take initial precedence over needle chest decompression and chest tube drainage. The purpose of the occlusive dressing is to prevent air from entering the chest through the wound, with the possible consequence of a pneumothorax.
The dressing can consist of any material that will ensure an airtight seal over the wound (e.g., aluminum foil, plastic wrap, Vaseline gauze). The traditional technique is to tape down all four sides of the dressing (Ill. 57). The last edge is taped down after the patient exhales forcefully. The dressing should be large enough to cover at least 2 inches past the wound on all four sides. If tape won’t stick to a wet or bloody chest, large trauma dressings can be held down with cravats that surround the chest. If an exit wound is present, as is commonly found with a gunshot wound, it must be covered too.
When the PHCP has neither the time nor equipment to carry out a needle chest decompression, a flutter valve dressing may be applied over the wound site to prevent the development of a tension pneumothorax. With the flutter valve, one corner of the occlusive dressing is left untaped (Ill. 58). As the patient inhales, the dressing will seal the wound. With exhalation, the free corner acts as a flutter valve to release air that is trapped in the chest. The advantage of the flutter valve over the traditional dressing approach is that the flutter valve does not tend to develop a tension pneumothorax that is sometimes seen with the traditional dressing approach.
Should a tension pneumothorax develop under a traditional dressing, one corner of the dressing is lifted up until the patient’s condition improves. Once the patient’s respiratory distress has abated, the wound is resealed. The procedure may have to be repeated a short time later. When a functional needle chest decompression or chest tube has been established, the flutter valve is taped closed.
NOTES
1 Stephen Westaby, Wound Care (St. Louis, MO: The C.V. Mosby Company, 1986), p. 118.
2 John Emory Campbell,Basic Trauma Life Support (Englewood Cliffs, NJ: Prentice-Hall, Inc., 1988), p. 97.
3 Ibid. pp. 346-347.
4 Ibid. p. 347.
5 Thomas Clarke Kravis and Carmen Germaine Warner,Emergency Medicine (Rockville, MD: Aspen Systems Corporation, 1983), p. 1095.
6 Ibid. p. 1097.
7 Stephen Westaby, Wound Care (St. Louis, MO: The C.V. Mosby Company, 1986), p. 140.
8 Walter J. Pories and Francis T. Thomas, Office Surgery for Family Physicians (Stoneham, MA: Butterworth Publishers, 1985), p. 163.