Photo 56: Endotracheal tube with its cuff inflated, syringe attached to ET tube, oropharyngeal airway, stylet, Magill forceps, curved blade, straight blade attached to handle, and stethoscope.
For those patients who cannot maintain a clear airway or are in need of emergency ventilation, endotracheal intubation is the most effective technique by which to address trauma or medically induced respiratory complications. Endotracheal intubation consists of passing a tube directly into the trachea. Once the tube is in place, it provides for isolation of the airway, thus preventing aspiration of material and fluids (i.e., blood, vomit) into the lower airway. Should suctioning of the tracheobronchial tree be needed, this is easily accomplished by introducing a suction catheter down the endotracheal tube. The endotracheal tube can also serve as a route for the administration of some drugs (e.g., epinephrine).
The endotracheal tube’s most critical function is the establishment of a superior means for ventilating the respiratoryarrested or depressed patient without gastric insufflation. 1 The three general intubation techniques are the laryngoscopic orotracheal approach, the nasotracheal approach, and the digital approach. The laryngoscopic orotracheal approach is the most widely used.
LARYNGOSCOPIC OROTRACHEAL INTUBATION
The following equipment is needed to carry out laryn-goscopic orotracheal intubation:
1. Laryngoscope—This is a two-part device used for exposing the glottis. The handle contains the batteries for the light source, and the blade has an integral bulb which provides illumination during the procedure. Straight blades (Miller) or curved blades (MacIntosh) are offered in a variety of sizes, and their use is dependent upon personal preference.
2. Endotracheal Tube—The endotracheal tube is a transparent tube that is open at both ends. The proximal end has a standard 15 mm connector that will fit the equipment used for positive pressure ventilation. The distal end of the tube has an inflatable cuff attached to an inflating tube that, once blown up, indicates whether the cuff is inflated. Tube sizes run from 7.0 to 8.0 ID for adult females and 8.0 to 8.5 ID for adult males. (ID indicates the size of the tube’s internal diameter in millimeters.) The correct choice is the largest tube that can easily get through the vocal cords and cricoid cartilage. Too large a tube may cause damage, and too small a tube may not ensure a sufficient cuff seal. In an emergency, a good standard- size tube for an adult is 7.5 ID.
3. Stylet—The plastic-coated malleable stylet is inserted through the endotracheal tube in order to help mold the tube into a “hockey stick” shape prior to insertion into the trachea. The end of the stylet must be shorter than the endotracheal tube by at least one-half inch in order to prevent trauma to the larynx and trachea.
4. Syringe—A 10 ml syringe is necessary for cuff inflation on the endotracheal tube.
5. Magill Forceps—Magill forceps are used for the removal of foreign objects from the airway or to assist in manipulating the tip of the endotracheal tube into the glottic opening.
6. Suction—Some form of suction should be available in order to clear blood, vomitus, or other fluids obstructing the airway.
7. Lubricant—A water-soluble lubricant applied to the outside of the endotracheal tube will ease insertion.
8. Oropharyngeal Airway—An oral airway is useful in stopping the combative semiconscious patient from biting down on the endotracheal tube and closing it off.
9. Stethoscope—A stethoscope is used to determine if the endotracheal tube is in the proper location(Photo 56).
Photo 56: Endotracheal tube with its cuff inflated, syringe attached to ET tube, oropharyngeal airway, stylet, Magill forceps, curved blade, straight blade attached to handle, and stethoscope.
The following technique is used for laryngoscopic orotracheal intubation:
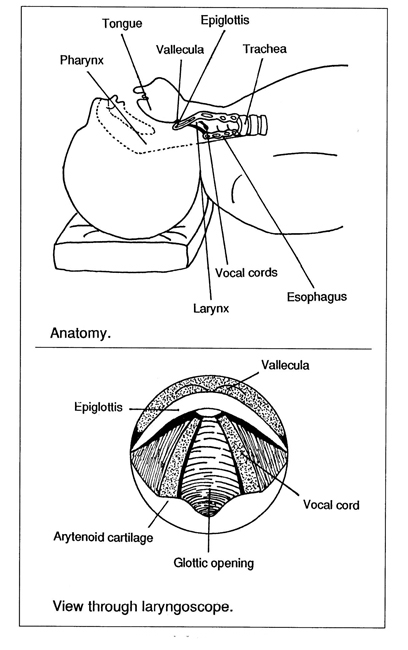
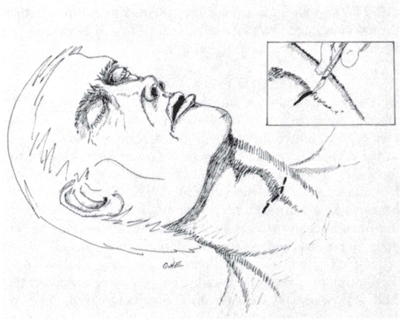
Double-check all equipment to ensure it is in working order. The laryngoscope light should shine and the cuff (balloon) of the endotracheal tube must hold its air. After checking the equipment, lubr icate the endotracheal tube. Positioning of the patient’s head is the next step. Three axes— those of the mouth, pharynx, and trachea—are aligned in order to achieve direct visualization of the larynx. To align these axes and therefore achieve the “sniffing position,” the head is extended and the neck flexed. A pillow of toweling placed under the patient’s occiput will provide the elevation needed for proper flexion of the neck (Ill. 79). Extension of the head is effected when the PHCP applies upward traction on the handle of the laryngoscope.
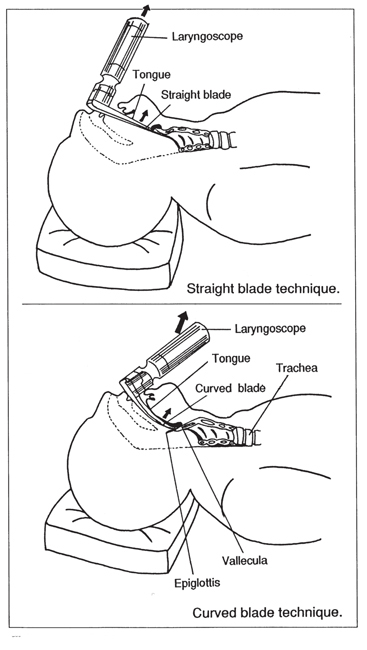
Once the patient has been positioned, the mouth is opened with the fingers of the right hand. The laryngoscope is held in the left hand and the blade inserted in the right side of the mouth, displacing the tongue to the left. The blade is moved carefully toward the midline and advanced to the base of the tongue. When a straight blade is used, it is advanced to just beyond and under the tip of the epiglottis. Upward traction is then applied with the handle of the laryngoscope, moving the base of the tongue and the epiglottis anteriorly to expose the glottic opening (Ill. 80) (Photo 57).
The tip of the curved blade is advanced into the vallecula. Lifting the laryngoscope upward and forward at the base of the tongue and epiglottis will expose the glottic opening. Neither type of blade should be used in a prying motion, and the upper teeth should never be used as a fulcrum. Observe the vocal cords before advancing the endotracheal tube. The tube is advanced over the right corner of the mouth and through the vocal cords until the cuff is just below the vocal cords. The stylet is removed and the cuff inflated (Ill. 81).
Proper positioning for the endotracheal tube must not be taken for granted. Its correct placement is validated by auscultation of the lungs and epigastric area. While ventilation is in progress, the lateral aspect of the chest at the midaxillary line is auscultated for breath sounds on both sides with a stethoscope (Photo 58). The epigastric area is then auscultated. If there are no breath sounds during auscultation of the lungs, or if there are gurgling sounds in the epigastric area, the endotracheal tube must be removed promptly since the esophagus has been intubated. Once the patient has been hyperventilated, the procedure can be tried again.
Photo 58: While ventilation is being carried out by a second PHCP, the PHCP in this photo is listening for breath sounds in the chest. Note that his hand is on the patient’s chest to feel for its rise and fall, and his eyes are focused on the chest in order to confirm other indicators.
Photo 60: Patient ventilation via bag valve to ET tube. Note orophrangeal airway is inserted and the ET tube is positioned properly to the side of the mouth.
If breath sounds are heard only in the right lung, the endotracheal tube is in the trachea, but it is too far down and lodged in the right mainstem bronchus. In such a case, simply pull back on the tube a little until breath sounds are heard in both lungs. Before beginning the intubation procedure or during breaks between tries, the PHCP should remember to hyperventilate the patient. Once the patient has been intubated, he can be ventilated easily via the mouth-to-tube or bagvalve- mask-to-tube approach (Photos 59 and 60).
NASOTRACHEAL INTUBATION
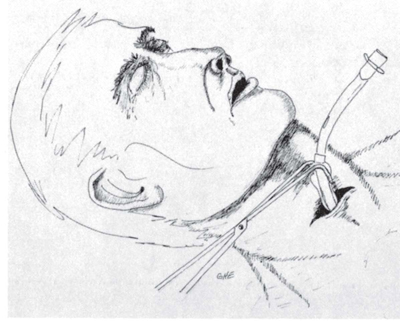
Due to the difficulty associated with the nasotracheal form of intubation, it may only be justified when the patient’s mouth cannot be opened because of clenched jaws, a suspected neck injury, or when lack of equipment restricts the PHCP to this approach. Since there is no visualization of the glottic opening in this form of intubation, guidance of the ET tube is dependent upon the PHCP perceiving the intensity of the patient’s exhalations. Bulging and anterior displacement of the laryngeal prominence generally indicates that the endotracheal tube has entered the glottic opening. Correct endotracheal tube placement is checked by holding a hand over or placing an ear over the opening of the endotracheal tube to detect airflow as well as auscultation of breath sounds (Photo 61).
Photo 61: Nasotracheal intubation of a patient. A stethoscope has been taped to the end of the ET tube to assist in proper placement. This technique is used when a laryngoscope is not available or a neck injury is suspected.
DIGITAL INTUBATION
Before the advent of the laryngoscope, endotracheal intubation was performed by the digital technique. Digital endotracheal intubation in the field is useful in those patients who have suffered facial injuries that distort anatomy, have bleeding or fluid buildup that obstructs visualization of the glottic opening, or are at risk of having suffered a cervical spine injury. The technique is based upon the simple approach of feeling the epiglottis with the fingers and then slipping the endotracheal tube through the glottic opening (Ill. 82).
The PHCP kneels at the patient’s left shoulder, facing the patient. The endotracheal tube is lubricated, shaped in the form of a J, and the stylet is slid down the tube. The PHCP places the index and middle fingers of his left hand down the midline of the tongue. This movement should also be augmented with a pulling forward on the tongue and jaw in order to lift the epiglottis up within reach of the middle finger. Once the epiglottis is reached, it is pressed forward with the middle finger. With his right hand, the PHCP then inserts the endotracheal tube into the mouth. The index finger of the left hand is used to keep the endotracheal tube tip against the side of the middle finger. With the middle finger keeping the epiglottis out of the way and the index finger used to keep the endotracheal tip against the side of the middle finger, the endotracheal tube is advanced by the right hand into the glottic opening.
Confirming Proper Endotracheal Tube Placement
Endotracheal intubation in the field is a crucial emergency airway skill that can have tragic consequences if esophageal intubation goes unrecognized. In such a case, the airway is not protected and ventilation efforts are useless. To confirm proper endotracheal tube placement, attention to the following signs are used to identify endotracheal tube location. The PHCP should not depend upon only one sign but rather upon a combination of signs that will be determined by the intubation approach used.
1. The most reliable sign is visualization of the endotracheal tube passing through the glottic opening. Although the most reliable, it is not applicable in all intubation techniques and may be difficult to ascertain in the patient suffering facial trauma or in whom the head and neck are immobilized due to suspected cervical spine injury.
2. An anterior displacement of the laryngeal prominence may be seen as the endotracheal tube passes into the trachea.
3. Phonation is a sign that the endotracheal tube is misplaced into the esophagus.
4. Auscultation for breath sounds is done on the right and left apex and midaxillary areas, as well as in the sternal notch. Ventilation should result in breath sounds being heard in both lungs. The epigastrium should be silent because gurgling sounds would indicate that ventilated air is passing into the stomach.
5. Palpation/visualization of the chest wall as ventilation is carried out will result in the PHCP being able to see and feel the chest wall rise and fall if the endotracheal tube is properly placed.
6. The cynotic patient should have improved color as the result of correct endotracheal tube placement.
Securing the Endotracheal Tube
Endotracheal tubes are dislodged easily in the field. Once the endotracheal tube is in proper position and ventilation is in progress, an oropharyngeal airway is inserted to prevent the patient from biting down on the tube. The patient’s face is dried off so that tape run around the neck and endotracheal tube will adhere. The endotracheal tube’s final placement should be in the corner of the mouth.
CRICOTHYROIDOTOMY
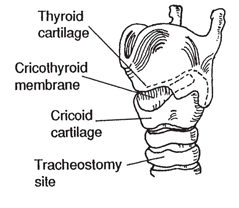
There are situations that arise, particularly in the field, in which respiratory ventilation of a patient cannot be accomplished with intubation through the mouth or nose. When all other effor ts fail, the inser tion of an endotracheal tube through the cricothyroid membrane is an accepted approach for establishing an emergency airway. The cricothyroid membrane is an acceptable insertion site because there are no important organs or vessels between the skin and the airway that can be damaged, and it is easy to locate anatomically.
The cricothyroidotomy is begun by placing a pillow under the shoulders of the patient and hyperextending his neck. The PHCP now locates the thyroid and cricoid cartilages. The indentation felt just below the thyroid cartilage and just above the cricoid cartilage is the appropriate site for scalpel incision of the cricothyroid membrane (Ill. 83).
The skin and cricothyroid membrane are punctured in the midline, with the incision extended about 1 cm toward each side in a transverse manner. The endotracheal tube is inserted until the cuff is no longer seen (Ills. 84 and 85). The cuff is inflated just enough to stop air from leaking around the tube when ventilation is in progress (Photo 62). If the patient is conscious, the insertion site should be anesthetized if the situation at hand will allow for this delay.
NOTES
1 Textbook of Advanced Cardiac Life Support (American Heart Association, 1987), p. 30.