Chronic Illness Is Born
What we know about illnesses and risk factors for illness that your body can tell us
CASE 1: Patient HB is a 39-year-old man who is a physical education teacher in a high school. He weighed 326 pounds. When he came to see Dr. A, his blood pressure was in the 190/70 mmHg range (very high). His LDL cholesterol was 160 gm/dL, and his triglycerides were 360 gm/ dL. He showed signs of prediabetes. His EKG had already changed to show strain from the blood pressure. Dr. A put him on blood pressure medications and an intensive diet. She put him on an exercise plan. He lost 100 pounds. His blood pressure came into the 120 mmHg range. His LDL cholesterol dropped into the 130 gm/dL range, and his triglycerides came down into the 150 gm/dL range (normal). He felt like he could keep up with his students and was feeling better.
CASE 2: JS is a 45-year-old accountant who is morbidly obese with diabetes, hypertension, and atrial fibrillation (abnormal heart rhythm). He had sleep apnea (intermittently using a CPAP machine to keep his airways open so he could get enough oxygen at night). He was a former wrestler and wanted to get back to it. He came to see Dr. A for preoperative clearance to treat an injured toe. Dr. A put him on medication to control his heart rate and manage his blood pressure. She insisted on the patient’s compliance with use of their CPAP machine. She put him on a plant-based, whole-grain diet. He was the perfect patient. He lost 65 pounds, came off of some of his blood pressure medications, and decreased medication for his blood sugar. His heart rates were better controlled, and he felt great. Dr. A sent him for foot surgery, and after the three-month healing of his toe, he started to wrestle again. He said he couldn’t believe he was wrestling again. He didn’t think he would ever get back to it.
How We Become at Risk for Illness
Many of the illnesses we see in our practices are due to a disruption in balance. In this chapter, we are going to explore what has happened to illness over the decades.
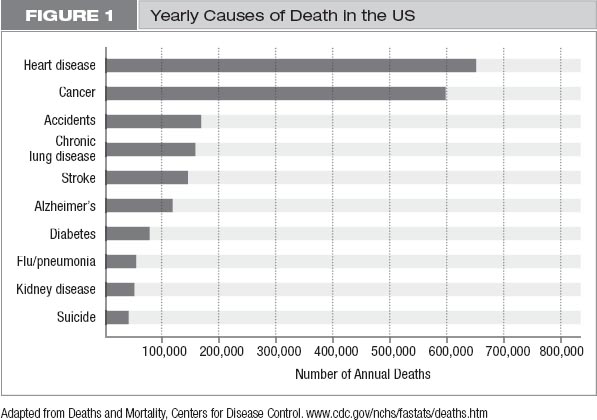
Heart disease, stroke, and cancer are the top killers of men and women around the world.1 In America, we are seeing more lung cancer, breast cancer, pancreatic cancer, and colon cancer than ever before. We also see more Alzheimer’s disease, more autoimmune disease, and more osteoarthritis than in years past. (Figure 1)
Over the decades, we have also seen individuals in our communities become more sedentary and gain more weight. Food preparation has shifted away from fresh food and cooking daily to ordering fast food and microwaving precooked or preprepared meals. Foods are filled with preservatives to increase their shelf life. Our jobs have become more sedentary. As a society, we work more and drive home in cars instead of walking. With these changes, we are fatter than ever before in history, with more than two of every three adults overweight or obese.2 (See figure 2.) With that, the number of people with diabetes and prediabetes has reached 100 million people, and 10 percent of the US population is now diabetic.3
Let’s talk for a moment about these illnesses in more detail.
Diabetes
Having diabetes puts us at significant risk for heart disease. We often find that people don’t understand why diabetes is dangerous. When we discuss diabetes in this book, we are primarily talking about type 2 diabetes, which is associated with obesity and insulin resistance. In order to understand diabetes, you have to understand the role of the pancreas. The pancreas is an organ in our bodies that makes the hormone insulin. The pancreas’s job is to bring glucose into cells to build fat stores for later energy use. There are receptors on the pancreas for the insulin hormone. These receptors are like entry cards to get into cells. In the case of obesity or excess fat, there can be masking of the receptors on the cells, and the insulin hormone is not able to attach to these receptors. This is called insulin resistance. Without entry into cells, insulin isn’t effective and doesn’t get turned into fat. As a result, more sugar is floating around in the bloodstream. Some people might see that as positive and say, “If I can eat and not have it turn to fat, that’s a good thing, right?”
Unfortunately, no. The problem is that floating sugars are extremely inflammatory, so as they circulate through the body, they irritate your blood vessels. They cause fissures in the blood vessels of the heart and cause scabs or plaque to form. The plaque migrates to the eyes and damages their small blood vessels, so people slowly lose their vision. As these scabs build in other blood vessels, they prevent blood from flowing to the various organs. Eventually, one of those blood vessels is completely blocked, and a part of the organ that the blood vessel supplies will die.
Studies show that weight loss can decrease blood sugars and correct diabetes.4 Reducing simple carbohydrates and refined sugars will help reduce insulin resistance and diabetes. It seems, then, we have the ability to change the course of the disease, and with the reduction of diabetes, there will be a reduction of cardiovascular disease. (See Consider 1.)
CONSIDER 1
 Consider what you are doing to your body to put yourself at risk for diabetes.
Consider what you are doing to your body to put yourself at risk for diabetes.
Heart Disease
Let’s talk about heart disease a little more, beginning with how it develops. Cardiovascular disease, often referred to as coronary artery disease or heart disease, is the formation of plaque in the coronary arteries. These arteries sit on the surface of the heart and supply blood to the heart so the heart can pump blood to the rest of the body. We often talk about these coronary arteries as the plumbing for the heart pump. When there is plaque buildup in the pipes, blood can’t effectively flow through them and the heart can’t pump well. Then there would be limited blood flow to the brain and other essential organs, causing damage to those organs. So, keeping the coronary arteries in good health is key to overall health.
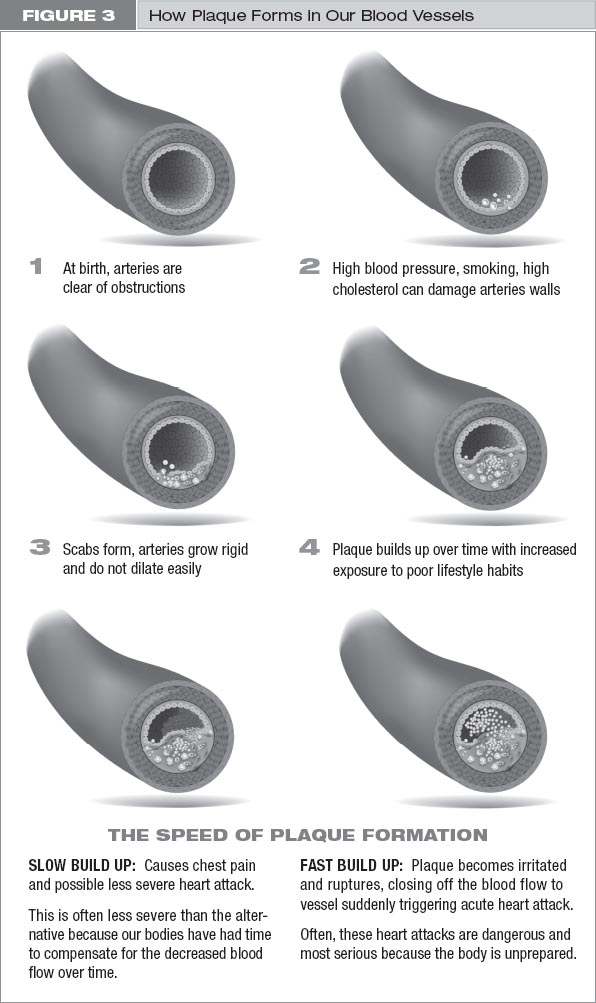
How do we get plaque in our pipes, though? The endothelium is the inner layer of cells in all blood vessels, including the pipes in the heart—the coronary arteries. The endothelium is responsible for dilating the blood vessels to accommodate changes in activity level. When we exert ourselves, our blood vessels widen to allow more blood to flow through them, so it can reach the organs that need it. When we develop risk factors for heart disease, such as high cholesterol, high blood pressure, or smoking, the endothelium of the blood vessels becomes damaged. This is called endothelial dysfunction, which is the beginning of atherosclerosis (also known as coronary artery disease or heart disease). When the endothelium is damaged, it becomes rigid and does not dilate easily.
This damaged endothelium becomes a site for more plaque being deposited. Then platelets (which form clots) come to the site because they see damage to the blood vessel and start repairing the lining. This process of endothelial dysfunction and subsequent platelet adhesion (clot formation) creates the beginning of an atheromatous plaque, plaque forming on the insides of our artery walls. Think of this plaque like a scab on the body when it’s injured. But unlike the outer surfaces of our bodies, where it does not matter how big the scab is because space is infinite, in a blood vessel it matters a great deal. The larger the scab, the more blood flow is obstructed. Blood can’t get where it needs to go. (See figure 3 on the next page.)
As we develop more risk factors or the risk factors we have progress, more plaque adheres to the scab, and it gets bigger and bigger. When the plaque closes off the blood vessel completely, a person has a heart attack. There are two types of heart attacks. One type is where a small plaque or scab sitting in a coronary artery suddenly and randomly ruptures (explodes) in a blood vessel, and a 30 percent blockage of a blood vessel becomes a 100 percent blockage. That creates an acute heart attack and often results in death or heart failure. These are the heart attacks where patients are rushed urgently into our procedure labs and need to have a blood vessel opened quickly, usually with a stent.
The late actors James Gandolfini and Carrie Fisher died of this type of heart attack. We never know which of the scabs is going to rupture, but we do know that inflammation plays a role. Something irritates the cap of the scab, and it becomes susceptible to rupture, leading to subsequent blockage of the blood vessel. Interestingly, a plaque that has blocked 30 percent of a blood vessel is more likely to rupture and cause a major heart attack than one that has blocked 80 percent because the larger plaque has become calcified and hardened and is therefore less prone to rupture. Different imaging techniques help us understand which plaques are most prone to rupture, but the answer remains elusive. The best procedures we have are stress testing or taking X-rays of the heart arteries (to give something called a coronary calcium score) and measuring inflammatory markers that are specific to the heart. Highly sensitive C-reactive protein (hs-CRP) is a marker of inflammation, and this can often give us useful information that the heart is irritated.
The second type of heart attack occurs when blood flow demand and supply are mismatched. This happens when plaque builds up over time in the coronary arteries but doesn’t always completely occlude the artery. It can also happen when there is another stressor, such as elevated blood pressure, infection, or anemia. The body needs the heart to pump blood to the other organs, but the coronary arteries are filled with plaque and the body can’t get the heart to pump faster. As a result, people can develop chest pain and decreased blood flow to parts of the heart as well.
How can we decrease inflammation in the heart? We know that statins decrease the inflammatory marker, highly sensitive CRP, and can stabilize plaque, even when LDL cholesterol is not elevated. That is why so many of our cardiac patients are on statins. There are decades of data to show how effective statins are in reducing cardiovascular risk, and their benefits cannot be underestimated. There are also studies, however, supporting that many foods in our diet are inflammatory and cause the body to become irritated. Studies have shown that eating just one fatty meal can create endothelial dysfunction within four hours after the meal.5 There are other studies that show how changing to a primarily plant-based diet will reduce inflammation and can decrease risk for cardiovascular disease.6,7 Then there are other options besides pills to make us better! Yay! More on this on pages 53–72.
High Cholesterol
Cholesterol is an important substance for the body. It helps build the walls of our cells. It is the foundation of our sex hormones and important for formation of myelin sheaths, which are necessary for nerve conduction. When we have too much cholesterol, however, it finds other homes, such as in our heart arteries, head arteries, and legs. There are two main types of cholesterol: HDL (good cholesterol) that is responsible for removing cholesterol from the blood and taking it to the liver, and LDL (bad cholesterol) that puts it back into the blood vessel and helps to form plaque. When we are born, our LDL cholesterol levels are about 50 gm/dL. As our cholesterol levels go up with diet changes and other factors, we know we are more at risk for heart disease.
We often hear from our patients that their children “can afford to eat McDonald’s food and fried chicken” because they are young. Is that really true? When we look at autopsies of children who died of unrelated causes, we find fatty streaks, signifying early plaque formation. Seventy-seven percent of men who fought in the Korean War had evidence of significant atherosclerosis. The average age of those men was 22 years.8 Similar findings were seen in American men who fought in Vietnam.9 This shows that the process starts at such a young age, and that what we put into our bodies at that young age matters. We can never afford to eat poorly. The bad foods that we eat as children put us at risk for heart disease and, as we will discuss later, for autoimmune disease, cancer, and other chronic illnesses as well. (See chapter 6 for details). The habits we create in children will last for a lifetime. It is so much easier to expose our children to healthy foods from the beginning so they will build a lifelong love of eating well.
Obesity and Hypertension
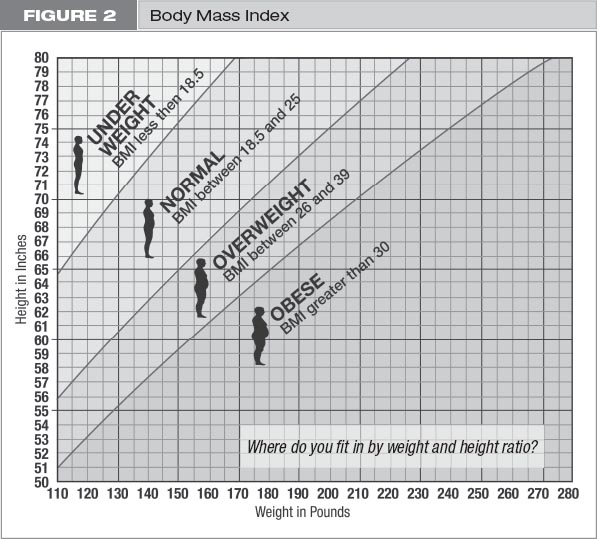
Before we talk about obesity, we need to define the terms. Obesity is often based on the body mass index (BMI), which is weight in kilograms divided by height (in meters) squared. There are many calculators available on the internet to aid in calculating your BMI. (See figure 2 on page 25.) Normal body mass indices are between 18.5 and 24.9 kg/m2. Being overweight is defined as having a body mass index between 25 kg/m2 and 29.9 kg/m2.10 There are gradations of obesity, but for our purposes, obesity is defined as a body mass index of greater than 30 kg/m2. BMI is not a perfect assessment for obesity. BMI does not take into account thin people who have high fat percentages and central obesity (fat around the abdomen) or heavier people who have high muscle mass. We feel fat percentage and muscle mass are more informative than BMI. However, many of the national assessments are based on BMI. As noted earlier, as of 2009 over two-thirds of the population is considered overweight or obese.11
Being overweight and obese are associated with an increased risk of death.12 In studies of overweight individuals above 50 years of age, there was nearly a 20 to 50 percent increased risk of dying.
What is it that our overweight and obese population is dying of? In one study, overweight men and women had a 52 percent and 62 percent risk, respectively, of death from cancer.10 According to the Prospective Studies Collaboration analysis, when obese individuals were examined, a proportionately increased risk of heart disease, diabetes, cancer, and lung disease was found.13 Cancers associated with increased weight, in particular, are liver cancer, kidney cancer, and breast, endometrial (uterine), prostate, and colon cancer. On the other hand, there are multitudes of studies to corroborate that the leaner we are, blood pressures decrease, sugars become more controlled, and we feel better.14
Obesity is strongly associated with high blood pressure (hypertension) and high cholesterol. Obese people typically eat more saturated fats and highly salted foods, which are felt to be significant causes of not only obesity but also of worsening blood pressure and high cholesterol. More than 100 million American adults, about 33 percent of the total adult population, have total cholesterol levels greater than 200 mg/dL (ideal is less than 200 mg/dL).15 Of people with high cholesterol, about 67 percent of them are either overweight or obese. With the new American Heart Association hypertension guidelines, now almost 50 percent of Americans are considered hypertensive.16
Hypertension causes damage to the blood vessels, and high cholesterol boosts plaque formation. Both are directly linked to increased risk of heart disease. In the Framingham Study, obese people had more than twice the risk of heart disease compared to their leaner counterparts.17 Obese individuals are more likely to have weakening of the heart or heart failure, as well as abnormal heart rhythms.
There is also a link between obesity and stroke, liver disease, and arthritis. The more weight we carry on our joints, the more traumas those joints suffer. Arthritis is one of the most costly morbidities associated with obesity. We have even linked skin changes, such as thickening of the skin (acanthosis nigricans), stretch marks, and increased hair production in women to obesity.
We weren’t always so fat. We can all recall that when we were younger, people were smaller. When Dr. A was 20 years old, she weighed 120 pounds and wore a size four. Three babies and 15 years later, she now weighs a bit more than that, but she still wears a size four. Why is that? This is called vanity sizing. Retailers have gotten smarter. As people gained weight, they didn’t fit into their usual sizes and needed bigger clothing. But people didn’t want to buy larger sizes, so they didn’t buy as many clothes. As a result, clothing manufacturers have adjusted their sizes to allow consumers to buy smaller-sized garments and feel skinnier. We heard a great story on Hidden Brain, Shankar Vedantam’s show on National Public Radio, stating that a size six in 1970 would be comparable to a size two in 1996 and a size zero in 2012. Size zero! As we have gotten larger, we have changed our concept of what is normal. We are changing the sizes of our clothes to reflect that change, so we don’t feel we are bigger. But we know that we are.
Many environmental factors contribute to obesity. Large portion sizes, high-sugar drinks, fast food, decreased physical activity, and watching more television are all linked to obesity. Television has been shown to directly influence our risk of obesity, and these trends are likely to follow into adulthood.18
Back in the old days, when people lived off the land, we were not an overweight population. We worked in the fields all day, picked our food for supper from the garden, and ate it while it was fresh. We ate more vegetables, fruits, and nuts. We lived off the land and only killed what we needed to feed our families. Nothing was wasted.
Over time, we have left our farms. We go to fast-food restaurants to get a quick meal as we drive to work. We sit for eight to ten hours per day and get up only to refill our sodas and eat meals. Often we are so busy that food is brought into meetings, so we don’t have to break for a meal. We eat what is there and often much more than we need. We eat snacks and desserts because they are readily available. We then drive home and are usually too tired to exercise. We might eat a quick frozen dinner in front of the television and fall asleep. We snack until the late hours of the night. The sizes of our plates have gotten larger, so we eat more food. We drink less water and supplement with sodas and coffee to keep us awake because we are often tired. We eat pasta and simple sugars all day, so we have constant dips and plateaus in our energy levels. We then get a jolt of caffeine to keep us awake during the post-eating dips. Over time, we have become overweight and sedentary.
We have the ability to change this. Now that we have talked about the changes in chronic illness over time and the diseases our bodies are at risk for, we want to shift attention to the link between what we eat and how it changes the composition of our gut flora, which in turn activates abnormal body responses.