menstrual loss, thereby improving iron-deficiency anaemia.
menstrual loss, thereby improving iron-deficiency anaemia.Combined hormonal contraceptives (CHCs), including the combined pill, vaginal ring, and patch
Levonorgestrel intra-uterine system
Copper intra-uterine contraceptive device
Fertility awareness methods (FAM)
Lactational amenorrhoea method (LAM)
Despite the availability of wide variety of contraceptive methods, TOP rates remain high (UK data: 1 in 3 women have a TOP with a third requesting a repeat). Annually, about 190,000 TOPs are performed in England and Wales. At least 60% of these women report having used a contraceptive method at the time of conception, usually oral contraceptives or condoms, which require correct and consistent use. Table 34.1 compares failure rates for pills, condoms, and natural methods with typical and perfect use. At the first contraceptive consultation the HCP should:
• Consider the importance of efficacy and reversibility (is an unplanned pregnancy acceptable?).
• Find out if there is a particular interest in a contraceptive method?
• Take a comprehensive medical and sexual history. Dysmenorrhoea or heavy menstrual loss may indicate that a combined hormonal method, an injectable method, or a levonorgestrel intra-uterine system (IUS) would be ideal, offering therapeutic benefits.
• Dispel any contraceptive myths, e.g. the Pill makes you put on weight, injectables cause infertility, IUDs give you infections.
• Address the woman’s worries and concerns, and explore why any previous contraceptive methods have been discontinued
• Discuss all options, focusing on long-acting and reliable contraceptive methods (LARCs).
• Explain how individual methods work, the advantages of each method, how to use the method, and any side effects that may occur and how they may be resolved.
• Provide accurate and up-to-date advice, including information on help lines and follow-up appointments.
Table 34.1 Summary table of contraceptive efficacy
| Method | %♀ with unintended pregnancy in 1st year | %♀ continuing use at 1 year‡ | |
| Typical use* | Perfect use† | ||
| No method | 85 | 85 | – |
| Spermicides | 28 | 18 | 42 |
| Withdrawal | 22 | 4 | 46 |
| Fertility awareness methods | 24 | – | 47 |
| Diaphragm | 12 | 6 | 57 |
| Condom—female | 21 | 5 | 41 |
| Condom—male | 18 | 2 | 43 |
| Combined and progestogen-only pill | 9 | 0.3 | 67 |
| Evra® patch (transdermal combined hormone) | 9 | 0.3 | 67 |
| NuvaRing® (vaginal combined hormone) | 9 | 0.3 | 67 |
| Progestogen injectables | 6 | 0.2 | 56 |
| Intra-uterine T380A (copper T) | 0.8 | 0.6 | 78 |
| Intra-uterine (LNG-IUS) Mirena® system | 0.2 | 0.2 | 80 |
| Nexplanon® | 0.05 | 0.05 | 84 |
| Female sterilization | 0.5 | 0.5 | 100 |
| Male sterilization | 0.15 | 0.1 | 100 |
* Among typical couples who initiate use of a method (not necessarily for the first time), the percentage who experience an accidental pregnancy during the first year if they do not stop use for any other reason.
† Among couples who initiate use of a method (not necessarily for the first time) and who use it perfectly (both consistently and correctly), the % who experience an accidental pregnancy during the first year if they do not stop use for any other reason.
‡ Among couples attempting to avoid pregnancy, the % who continue to use a method for 1 year. Adapted from Trussell J (2011) Contraceptive failure in the United States. Contraception 83(5): 397–404, with permission from Elsevier.
CHCs are highly effective and quickly reversible, with failure rates of <1% per year when taken consistently and correctly (Table 34.1). 73 million ♀ (16% of all in their reproductive years) in the UK take combined oral contraception (COC). >90% of sexually active ♀ have used the pill by the time they reach 30. COC is suitable from menarche to menopause, if no contraindicating risk factors or co-existing illnesses are identified.
• Alter cervical mucus, inhibiting spermatozoa penetration.
• Produce characteristic changes in the endometrium preventing implantation of the blastocyst.
• Modify sperm function/motility and cervico-uterine secretions.
• Effective, reversible, convenient, non-intercourse related.
• Regulates and menstrual loss, thereby improving iron-deficiency anaemia.
• Reduces dysmenorrhoea and relieves ovulation pain.
• May help premenstrual symptoms.
• Helps protect against ectopic pregnancies as it inhibits ovulation.
• Decreases incidence of benign breast disease.
• Long-term users are less likely to develop fibroids and functional ovarian cysts.
• Protects against PID and the risk of hospitalization for the disease.
• Reduces incidence of endometriosis, and a useful treatment and maintenance therapy for sufferers.
• Possible in the risk of developing rheumatoid arthritis and its associated symptoms.
• Reduces risk of ovarian cancer by 20% with every 5 years of use. ♀ who use this method for 15 years have half the risk of ovarian cancer compared with women who have never used this method.
• Reduces the risk of endometrial cancer by ~50%, with protection continuing for at least 20 years after the CHC is stopped.
• Reduced incidence of large bowel cancer by up to 40%.
• Requires correct and consistent use to be effective (see Box 34.1 for instructions if taken incorrectly).
• Side effects may occur in the first few months, e.g. headaches, breast tenderness, breakthrough bleeding (although these tend to resolve quickly).
• Patches may cause a local skin reaction in about 10% of users with 2–3% discontinuing for this reason. 5–14% of ♀ using the vaginal ring complain of vaginitis.
• The vaginal ring can only be kept at room temperature for 4 months and requires a cold chain delivery system
• Potential drug interactions decrease the efficacy of these methods, e.g. use of liver-enzyme-inducing agents, St John’s wort.
• May be associated with  risk of breast cancer. The re-analysis data published in 1996 reported that current COC use the risk of developing breast cancer by 24%, but this fell back to background level 10 years or more after discontinuing the pill. However, five recently published studies have found no risk.
risk of breast cancer. The re-analysis data published in 1996 reported that current COC use the risk of developing breast cancer by 24%, but this fell back to background level 10 years or more after discontinuing the pill. However, five recently published studies have found no risk.
• After 5 years of use there may be an incidence of cervical intra-epithelial neoplasia and cancer of the cervix. COC appears to be a cofactor leading to persistence or repeated replication of oncogenic HPV. Regular cervical screening, as indicated by the NHS Cervical Screening Programme, should be advised.
• Possible small in the risk of myocardial infarction (MI) in non-smoking low-risk ♀. However, the risk may up to 20-fold in heavy smokers.
• Possible small (up to 2-fold) in the risk of ischaemic stroke in users, with about 3 ischaemic strokes occurring in 100,000 ♀ under 35 each year. Risk factors include hypertension, smoking, diabetes, and family history of stroke. No in the risk of haemorrhagic stroke in low-risk non-smoking ♀ with normal blood pressure.
• Increased risk of venous thromboembolism (VTE). Background risk of VTE in young ♀ is now thought to be about 2 per 10,000 ♀ each year. This risk increases to 5–7 per 10,000 women using CHC containing levonorgestrel, norethisterone, and norgestimate; 6–12 per 10,000 women using the vaginal ring or patch; and 9–12 per 10,000 women using CHC containing drospirenone, desogestrel, gestodene or cyproterone acetate. Increasing age, obesity, surgery, family history of VTE, and immobility the risk of developing a VTE.
Box 34.1 Missed pill rules for COCs containing ethinylestradiol
• If missed one pill anywhere in the pack:
• take forgotten pill, take next pill when due.
• If missed two pills (i.e. > 48 hours late) anywhere in the pack:
• use a condom or abstain for 7 days
• if pill-free interval in next 7 days do not stop pills, but start new packet straight away.
• If missed pills were in Week 1 of COC use and any unprotected sex has occurred in the 7 preceding days, then emergency contraception is required.
Although all CHCs have the same mode of contraceptive action and similar efficacy they may have different side effects or benefits (e.g. less breakthrough bleeding or an improvement in acne). The first pill prescribed should be effective, suit the majority of ♀, have a proven safety record, and be inexpensive. A monophasic 30 mcg levonorgestrel pill (such as Microgynon® 30 or a branded generic pill) fulfils these criteria. 40% of ♀ may complain of side effects or perceived associated problems and request a change.
These LARC methods avoid daily pill taking, but have a similar efficacy as COC. Both give a regular monthly withdrawal bleed and are advantageous in ♀ who cannot remember to take a daily pill or who have gastrointestinal problems affecting pill absorption. The patch needs changing every 7 days with a patch-free week every 4th week. The vaginal ring is worn for 3 out of every 4 weeks. Minor and potentially serious, but rare, side effects are similar to those with COC.
• First choice: 30 mcg levonorgestrel, monophasic preparation (such as Microgynon30® or a branded generic pill).
• To improve cycle control: 30 mcg gestodene or 35 mcg norgestimate pill or vaginal ring once pathology, drug interaction, or poor compliance are excluded (e.g. Millinette 30/75®, Cilest®, NuvaRing®).
• Oestrogen side effects: include headaches, nausea, breast tenderness, or leg cramps. Reduce the dose of oestrogen to a pill containing 20 mcg ethinylestradiol (e.g. Millinette 20/75®, Loestrin20®, Gedarel 20/150®, Daylette®) or estradiol (Qlaira®, Zoely®), or change to a progestogen-only pill.
• Progestogen side effects: include mood change, bloating, and greasy skin. Change the progestogen in the pill. Cyproterone acetate and drospirenone in COCs are useful in ♀ with acne (e.g. Dianette®, Yasmin®, or branded generic).
See Table 34.2.
Table 34.2 Starting combined hormonal contraceptives
| Circumstances | When to start | Extra precautions for 7 days? |
| Quick start | At any time, if it is reasonably certain not pregnant | Yes |
| Menstruating | Up to and including day 5 After day 5 | No Yes |
| Amenorrhoeic | At any time, if it is reasonably certain not pregnant | Yes |
| Post-abortion or miscarriage | Within 5 days After 5 days | No Yes |
| Starting combined hormonal contraception post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Not breast-feeding | Start Day 21 post-partum (note it is not advised to start CHC until Day 21 in this group of women) | No |
| From day 22 onwards (women with an additional risk factor for VTE should start CHC at 6 weeks) | Yes | |
| Breastfeeding | From delivery until 6 weeks post-partum this method is not advised | N/A |
| From 6 weeks post-partum CHC can be used safely in women with no contraindications | Yes | |
| Switching from POP | Switch immediately from POP with a 3-hour window period | Yes |
| Switch immediately from POP with 12-hour window period | No | |
| Switching from implant | Switch any time before implant expires | No |
| Switching from injection | Any time before injection expires | No |
| Switching from IUS | Switch immediately post-removal (as long as no unprotected sex in previous 7 days) | Yes (or leave IUS in situ for a further 7 days and then remove) |
| Switching from IUD | Start up to and including day 5 of cycle. IUD can be removed at the same time | No |
| After Day 5 of cycle start CHC on removal of IUD (as long as no unprotected sex in previous 7 days) | Yes (or leave IUD in situ for a further 7 days then remove) | |
Taken by 6% of ♀ in the UK. It is very effective when taken properly, but has typical failure rates of 9%.
• Ovulation may be suppressed in 50% of cycles by POPs containing levonorgestrel, or norethisterone, but in 97–99% by those containing desogestrel.
• All POPs alter the cervical mucus to reduce sperm penetration.
• POPs induce changes in the endometrium to prevent sperm survival and implantation of the blastocyst.
• Sperm motility and function is affected, preventing fertilization.
Cervical mucus effect peaks within 2–3 hours of oral ingestion and then slowly wanes. Desogestrel-containing POPs differ from more traditional POPs in that no extra contraceptive cover is required until 12 hours after a missed pill compared with 3 hours for other POPs.
POPs have frequently been restricted to ♀ who are breastfeeding or who have contraindications to taking synthetic oestrogen. However, users from all age groups may be interested in taking a POP, particularly as it is very safe and suitable for most women.
• Non-intercourse-related contraceptive.
• Simple and convenient to use.
• POPs are safe for ♀ who are breastfeeding.
• Ideal for ♀ who suffer from oestrogenic side effects when using CHCs, e.g. breast tenderness, headaches, fluid retention, or nausea.
• Suitable for ♀ over 35 years who smoke.
• Can be used in grossly obese ♀ with no dose adjustment required.
• Can be taken by ♀ with medical illnesses that contraindicate the use of synthetic oestrogen, e.g. those with hypertension, migraine with focal aura, or a previous personal history of VTE.
• No evidence of risk of cardiovascular disease, thromboembolism, or stroke.
• Minimal alteration in carbohydrate and lipid metabolism. Therefore, they are ideal for diabetics even with neuropathic or nephropathic complications.
• Can be used safely until the menopause and does not mask menopausal symptoms.
• POPs, excluding the desogestrel POP, are thought to be less effective than combined pills in practice as they are very reliant on regular pill taking (see Box 34.2 for advice on missed doses).
• May cause side effects, such as breast tenderness, mood changes, headaches, and acne.
• Can alter ovulation, thereby disrupting the menstrual bleeding pattern, with users reporting an in spotting, breakthrough bleeding, and amenorrhoea
• Functional ovarian cysts may develop in a small number of women; however, these tend to be transient and rarely require surgical intervention.
• Potential drug interactions decrease the efficacy of POP, e.g. use of liver-enzyme-inducing agents, St John’s Wort.
See Table 34.3.
Table 34.3 Starting regimens for progestogen-only pills
| Circumstances | Start when? | Extra precautions for 48 hours |
| Quick start | Any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Menstruating | Up to and including day 5 of cycle | No |
| After day 5 of the cycle | Yes | |
| Amenorrhoeic | Any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Post-abortion or miscarriage | Within 5 days | No |
| After 5 days | Yes | |
| Starting progesterone-only pill post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Breastfeeding or bottle-feeding | Upto and incl. 21 post-partum | No |
| From day 22 onwards | Yes | |
| Switching from CHC | Day 1–2 of hormone-free interval | No |
| From day 2 onwards of hormone-free interval or during week 1 of CHC use | Yes | |
| During Week 2–3 of CHC use | No as long as CHC taken properly in the preceding 7 days | |
| Switching from implant | Any time pre-expiry of implant | No |
| Switching from injectable contraception | Any time pre-expiry of injection | No |
| Switching from an IUS | Immediately post-removal (as long as no unprotected sex in previous 7 days) | Yes (or start POP then remove IUS after 48 hours) |
| Switching from an IUD | Start up to and including day 5 of cycle. IUD can be removed at the same time | No |
| After Day 5 of cycle (as long as no unprotected sex in previous 7 days) | Yes (or start POP then remove IUD after 48 hours) | |
Box 34.2 Missed pill rules for POP
• If missed traditional POP by <3 hours or desogestrel POP by <12 hours: take forgotten pill and take next tablet when due.
• If missed traditional POP by >3 hours or desogestrel POP by >12 hours:
• take last forgotten pill and next pill when due, and use condoms for 2 days.
• Emergency contraception needed if any unprotected sex since the time of the missed pill.
Injectables are highly effective and have a safety record that spans 40 years. Intramuscular progestogen-only depot providing contraceptive cover for 2–3 months was one of the first long-acting hormonal preparations to be used. Progestogen-only injectables are used by ~3% of ♀ in the UK.
Three injectable contraceptive methods are available in the UK:
• Depo-Provera® (depot medroxyprogesterone acetate (DMPA-IM)) given every 13 weeks intra-muscularly normally into gluteus maximus.
• Noristerat® (norethisterone enantate (NET-EN) given every 8 weeks IM (used infrequently in the UK for short-term interim contraception).
• Sayana-Press® (DMPA-SC), given every 13 weeks subcutaneously into the anterior thigh or abdomen. This has been licensed for self-administration.
A significant number of ♀ fail to return for their second DMPA. Prolonged/erratic bleeding is often cited as a reason for discontinuation. Pre-injection counselling, giving a realistic picture of potential side effects in the first few injection cycles, is important.
• DMPA and NET-EN inhibit ovulation by suppressing luteinizing hormone (LH) and, to a certain extent, FSH.
• Injectables alter the cervical mucus, inhibiting spermatozoa penetration.
• Injectables prevent implantation by inducing endometrial atrophy.
• Like other progestogens, injectables modify sperm function and motility.
• Very effective, reversible, and discreet method of contraception with little dependence on the user.
• Non-intercourse-related contraceptive method.
• Very safe with no reported attributable deaths.
• Safe for breastfeeding mothers.
• Helpful for ♀ with premenstrual symptoms, ovulation pain, and painful heavy periods.
• Can be used in ♀ with sickle cell disease, with evidence suggesting a in crises
• Possesses most of the non-contraceptive benefits of CHCs, including protection against PID, extra-uterine pregnancies, endometriosis, functional ovarian cysts, and fibroid formation, ovarian cancer, and a 5-fold in the risk of endometrial cancer.
• Minimal metabolic effects occur, with recent research reporting no in the risk of acute myocardial infarction, VTE, or stroke.
• Safe to use in women taking liver enzyme-inducing drugs.
• Irregular prolonged vaginal bleeding/amenorrhoea. ~1/3rd experience prolonged bleeding (>10 days) after receiving their first injection, but 50% are amenorrhoeic by 1 year.
• IM or SC administration: therefore, cannot be removed if side effects occur.
• Weight gain commonly reported, particularly in young women whose starting BMI is >30 km/m2.
• Some may complain of progestogenic side effects, including mood changes, lassitude, loss of libido, bloating, and breast tenderness.
• Causes a short delay in the return to normal fertility with the mean time to ovulation being 5.3 months after the last injection.
• DMPA may adversely affect bone mineral density (BMD), but there are no good data suggesting that it causes osteoporosis or bone fracture. Present data suggest that BMD at the lumbar spine and femoral neck are in DMPA users compared with controls. BMD recovers to a similar level to never-users on discontinuation of DMPA (usually 3–5 years in adults and 18 months if <18 years).
• Committee on Safety of Medicines advice:
• in adolescents, DMPA may be used as first-line contraception, but only after other methods have been discussed with the patient and considered to be unsuitable or unacceptable
• in all ages, careful re-evaluation of the risks and benefits of treatment should be carried out in those who wish to continue use for >2 years
• if significant lifestyle and/or medical risk factors for osteoporosis, other methods of contraception should be considered.
• There is no evidence that routinely giving ‘add-back’ oestrogen to DPMA users or additional investigations to check bone mineral density such as DEXA scans are warranted.
• low-density lipoprotein (LDL)-cholesterol and high-density lipoprotein (HDL)-cholesterol so needs to be used with caution in women who have multiple cardiovascular risk factors.
• Injection site reactions have been reported in 6% of women using Sayana-Press®
• Potential small increase in the risk of HIV acquisition, thus users of injectable contraception, as with any other method, should be advised about HIV preventative measures, such as male and female condoms.
See Table 34.4.
Table 34.4 Starting regimens for injectable contraceptives
| Circumstances | When to start | Extra precautions for 7 days? |
| Quick start | At any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Menstruating | Up to and including day 5 | No |
| After day 5 of the cycle | Yes | |
| Amenorrhoeic | Any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Post-abortion or miscarriage | Within 5 days | No |
| After 5 days | Yes | |
| Starting injectable contraception post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Breastfeeding or bottle-feeding | Upto and incl. 21 post-partum | No |
| From day 22 onwards | Yes | |
| Switching from CHC | Day 1–2 of hormone-free interval and week 2–3 of CHC use From day 2 onwards of hormone-free interval and week 1 of CHC use | No Yes |
| Switching from POP | Switch anytime | Yes |
| Switching from implant | Anytime pre expiry | No |
| Switching from IUS | Immediately post-removal (providing no unprotected sex in previous 7 days) | Yes (or start injection then remove IUS after 7 days) |
| Switching from an IUD | Give the injection up to and including day 5 of cycle. IUD/IUS can be removed at the same time | No |
| After Day 5 of the cycle start immediately post-removal (as long as no unprotected sex in previous 7 days) | Yes (or start injection then remove IUD after 7 days) | |
A contraceptive implant offers an alternative way of delivering hormones providing long-acting low-dose reversible contraception. Norplant®, the levonorgestrel implant, was available in the UK from 1993 until 1999. It consists of 6 rods inserted subdermally ~8–10 cm above the elbow on the inner aspect of the non-dominant arm. It is licensed to provide contraception over a 5-year period. UK healthcare professionals may see ♀ from sub-Saharan Africa using this multi-rod contraceptive system or the two-rod system called Jadelle®.
Implanon®, containing a single rod of 68 mg etonogestrel (the active metabolite of desogestrel), was launched in the UK in 1999. It was replaced by Nexplanon® in 2010, which also contains 68 mg etonogestrel, but has a different preloaded applicator to decrease the risk of non-insertion, and contains barium, making it radiopaque so can be located on X-Ray and CT scan if need be.
It is used by 1% of ♀ in the UK and is licensed to provide contraception for 3 years. It is one of the most effective contraceptives with recent method failure rates quoted as 0.01 per 100 implants fitted.
• Etonogestrel inhibits ovulation by suppressing LH. However, up to 5% of users may ovulate in the third year.
• Implants also alter the cervical mucus, inhibiting sperm penetration and thereby preventing fertilization.
• Implants prevent implantation by inducing endometrial atrophy.
• Implants may modify sperm function and motility.
• Long-lasting (3–5 years depending on the type of implant), effective, immediately reversible, and no effect on future fertility.
• Free from oestrogen side effects
• High user acceptability following pre-insertion counselling, with continuation rates between 67% and 78% at 12 months.
• Requires little medical attention, other than at insertion and removal.
• Can be used by those in whom synthetic oestrogen is contra-indicated.
• Safe for breast-feeding mothers.
• Nexplanon® does not adversely affect cardiovascular risk factors, thrombotic factors, CRP, cholesterol/HDL-cholesterol ratio, and nitrous oxide.
• Minimal effects on glucose metabolism and liver function.
• No adverse effect on systemic oestrogen levels or BMD.
• Unpredictable and irregular bleeding patterns are common in Nexplanon® users with ~10% discontinuing because of prolonged and/or frequent bleeding with ~20% of 90-day reference cycles showing amenorrhoea, ~25% regular bleeding, ~30% infrequent bleeding, ~25% frequent and/or prolonged bleeding.
• Incidence of progestogen side effects with Nexplanon® similar to that with other progestogen-only methods. Side effects include headache, weight gain, acne, and mood changes.
• Insertion of implants requires a minor operative procedure under local anaesthetic by trained health professionals.
• Non-palpable implants have been reported in about 1 in 1000 insertions and are related to poor insertion technique. Very rarely, damage to the neurovascular bundle and intravascular migration has been reported. Referral to an ‘expert’ centre is advised for implant location using high frequency ultrasound scanning before removal. If the implant cannot be identified on imaging, a chest X-ray should be ordered and etonogestrel assays may be required.
• Some ♀ report mild discomfort and bruising following insertion or removal of the implants.
• Infection at the insertion or removal site, migration of the implants, and scarring are rare.
• Effectiveness may be reduced by concurrent usage of liver enzyme inducing drugs.
Contraceptive implants may not be a suitable method for some ♀ as discontinuation is not under their control.
See Table 34.5.
Table 34.5 Starting regimens for contraceptive implants
| Circumstances | When to start | Extra precautions for 7 days? |
| Quick start | At any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Menstruating | Up to and including day 5 | No |
| After day 5 of the cycle | Yes | |
| Amenorrhoeic | Any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Post-abortion or miscarriage | Within 5 days | No |
| After 5 days | Yes | |
| Starting implant post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Breastfeeding or bottle-feeding | Upto and incl. 21 post-partum | No |
| From day 22 onwards | Yes | |
| Switching from CHC | Switching on Day 1–2 of the hormone-free interval or in week 2–3 of CHC use Switching from Day 2 of the hormone-free interval and in Week 1 of CHC use | No Yes |
| Switching from POP | Switch anytime | No |
| Switching from an injection | Switch any time before injection expires | No |
| Switching from IUS | Immediately post-removal (as long as no unprotected sex in previous 7 days) | Yes (or leave IUS in for another 7 days then remove) |
| Switching from IUD | Insert the implant up to and including day 5 of cycle. IUD can be removed at the same time | No |
| After Day 5 of cycle switch immediately post-removal (as long as no unprotected sex in previous 7 days) | Yes (or leave IUD in for another 7 days then remove) | |
There are four different intrauterine systems available in the UK. Mirena® has been available in the UK since May 1995 and used by ~2% of ♀. Mirena® contains 52 mg levonorgestrel in a polydimethylsiloxane reservoir on the vertical arm of a T-shaped plastic frame. Mirena® provides highly effective, yet reversible contraception for 5 years. It is also licensed for the treatment of heavy menstrual bleeding and as the progestogen component of HRT.
Jaydess® has been available in the UK since 2014. Jaydess® contains 13.5 mg levonorgestrel in a similar T-shaped frame to Mirena®. The Jaydess® inserter tube and device itself are slightly smaller than the Mirena® equivalent. Jaydess® is licensed for 3 years and should be used for contraception only.
Levosert® has been available in the UK since 2015. Levosert® contains 52 mg levonorgestrel in a polyethylene T-shaped frame. The introducer differs from Mirena® and Jaydess®, as the fitting requires a two-handed technique. Levosert® is licensed to provide contraception and as a treatment for heavy menstrual bleeding over a 4-year period.
Kyleena® has been available in the UK since 2018. Kyleena® contains 19.5 mg levonorgestrel in a similar T-shaped frame to Mirena®. It is licensed to provide contraception for 5 years. The inserter tube and device are slightly smaller than the Mirena® equivalent.
• Alters cervical mucus and utero-tubal fluid, inhibiting sperm migration.
• Prevents endometrial proliferation by causing atrophic changes over time. This precludes implantation.
• May affect sperm motility and function.
• May suppress ovulation in some in the first year, possibly by reducing the pre-ovulatory LH surge.
• Long-acting (lasts 3–5 years, depending on the IUS) and independent of intercourse.
• Highly effective contraceptive (as effective as female sterilization) with an immediate return to fertility after removal. The in use of LARCs, such as the IUS has led to in requests for female sterilization in the UK.
• Reduces normal menstrual blood loss. After 3 years of use, 24% of women using Mirena® and 13% using Jaydess® have become amenorrhoeic. It is thought that Levosert® and Kyleena® have similar bleeding profiles to that of Mirena®.
• 90% after 12 months use have an in haemoglobin and serum ferritin. This has led to hysterectomies performed in the UK. They can be used in ♀ with coagulation disorders.
• Long-term use of Mirena® may prevent fibroid formation. Mirena® reduces heavy menstrual bleeding associated with fibroids and adenomyosis.
• Mirena® reduces the incidence of dysmenorrhoea.
• Mirena® may be a useful medical treatment for ♀ suffering from endometriosis-related problems with significant in severity and frequency of pain/menstrual symptoms. Good as maintenance therapy following conservative surgery for endometriosis.
• No evidence that serum oestradiol and BMD are affected.
• When used alongside oestrogen, Mirena® can be used in the treatment of premenstrual syndrome.
• May protect against the development of endometrial hyperplasia and cancer. Resolves endometrial hyperplasia without atypia in 92% of cases and endometrial hyperplasia with atypia in 67%. Not affected by concurrent use of liver enzyme-inducing drugs.
• May cause irregular/prolonged bleeding in the first 3 months. Prolonged bleeding/spotting (>6 months following fitting) may occur in those with heavy menstrual bleeding, with or without fibroids. Pre-insertion counselling should include information on menstrual disturbance.
• May be expelled or displaced, particularly with intra-cavity fibroids or heavy menstrual loss.
• Fitting may be painful and seen as invasive by women.
• Small risk of PID within first 20 days after fitting, particularly in young ♀. Screen for STIs prior to fitting in those at risk.
• ~10% of women using Mirena® may develop functional ovarian cysts, but these tend to resolve over 6 months or so, and rarely require surgical intervention. Approximately 22% of women using Kyleena® in clinical trials have been found to have ovarian cysts, most of which are asymptomatic.
• Risk of uterine perforation when fitting IUS (< 2/1000 devices fitted). Risk rises to 6/1000 insertions in breastfeeding women.
• Some progestogenic symptoms in the first few months, i.e. breast tenderness, bloating, or acne. These usually settle.
• Overall incidence of ectopic pregnancy is lower than in the general population, but if IUS fails then it is thought that up to 50% of pregnancies may be ectopic. It can be used in ♀ with a past history of ectopic pregnancy.
• Cannot be used as an emergency form of contraception.
See Table 34.6.
Table 34.6 Starting regimens for intra-uterine systems
| Circumstances | When to start | Extra precautions for 7 days? |
| Menstruating | Up to and including day 7 (avoiding insertion when menstrual flow is heavy, thereby reducing subsequent expulsion) | No |
| After day 7 of the cycle, as long as it is reasonably certain that ♀ is not pregnant | Yes | |
| Amenorrhoeic | Any time, if it is reasonably certain that ♀ is not pregnant | Yes |
| Post-abortion or miscarriage | Within 5 days | No (ensure no continuing pregnancy/retained products first) |
| After 5 days | Yes (ensure no continuing pregnancy/retained products first) | |
| After surgical TOP | Insert at time of the surgical TOP | |
| Starting intra-uterine system post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Breastfeeding or bottle-feeding | After day 28 (including following a Caesarean section) | Yes |
| Switching from CHC | Fit on Day 1 of hormone-free interval or during Week 2–3 of CHC use Fit from Day 2 of hormone-free interval and during Week 1 of CHC use | No Yes (or fit IUS and continue CHC for another 7 days) |
| Switching from POP | Switch anytime | Yes |
| Switching from implant | Any time before implant expires | No |
| Switching from injection | Any time before injection expires | No |
| Switching from IUD | Switch methods immediately if Day 1–7 of cycle | No |
| After day 7, advise no sexual intercourse for 7 days prior to switching the methods | Yes | |
IUDs are used by >110 million ♀ world-wide, with >50% of these users in China. Only 6% of ♀ in the UK use IUD, possibly because of concerns and myths attached to these methods. IUDs available in the UK are small copper-containing devices in varying shapes and sizes. Most have a central frame made of polyethylene impregnated with barium, making them radiopaque. A frameless device called GyneFix® is also available. Most devices contain >300 mm2 of copper, making them a highly effective, reversible, and inexpensive contraceptive option.
• Prevents fertilization as copper ions are toxic to sperm and ova (main mechanism).
• All IUDs the number of leucocytes in the endometrium, producing a typical ‘sterile’ inflammatory endometrial response, which helps prevent implantation. Copper enhances this reaction. The increased copper content of cervico-uterine mucus inhibits sperm penetration.
• An IUD is not an abortifacient.
• Long-term (up to 10 years), highly effective contraceptive with no delay in return to fertility following removal.
• No associated weight gain or hormonal side effects.
• Very effective as an emergency contraceptive. Can be fitted up to 5 days after unprotected sexual intercourse (UPSI) or 5 days after estimated time of ovulation, whichever is later.
• High acceptability and good continuation rates.
• Inexpensive and very cost-effective.
• Risk of ectopic pregnancy is low in devices with 300 mm2 of copper. The incidence of ectopic pregnancy is 0.02 per 100 women-years, which is less than in those using no contraceptive method.
• May cause menstrual irregularities with intermenstrual bleeding and spotting more common in the first 6 months after insertion.
• Periods may become heavier, more prolonged, and painful, especially soon after insertion. ~10% of ♀ discontinue in the first year, citing menstrual bleeding and pain as the main reason.
• Users are more prone to bacterial vaginosis.
• ~1 in 20 IUDs are expelled; more likely within the first 3 months of fitting and similar for all types.
• Risk of PID associated with insertion, especially within the first 20 days. May be prevented by pre-insertion STI screening for those at risk.
• Rare complications, e.g. uterine perforation may occur in <2/1000 insertions (increased to 6/1000 insertions in breastfeeding ♀).
See Table 34.7.
Table 34.7 Starting regimens for intra-uterine devices
| Circumstances | When to start | Extra precautions for 7 days? |
| Menstruating | At any time in the cycle if it is reasonably certain that the ♀ is not pregnant (avoiding insertion when menstrual flow is heavy, thereby subsequent expulsion) |
No |
| Amenorrhoeic | Any time if it is reasonably certain that ♀ is not pregnant | No |
| Post-abortion or miscarriage | Immediately at the time of surgical TOP | No |
| At any time following medical termination or miscarriage by an experienced clinician, as long as there is no concern that the pregnancy is not ongoing or that there are retained products of conception | No | |
| Starting intra-uterine device post-partum | ||
| Circumstances | When to start | Extra precautions for 7 days? |
| Breastfeeding or bottle-feeding | After day 28 (including following a Caesarean section) if it is reasonably certain that ♀ is not pregnant | No |
| Switching from CHC | Switch immediately | No |
| Switching from POP | Switch immediately | No |
| Switching from implant | Any time before implant expires | No |
| Switching from injection | Any time before injection expires | No |
| Switching from IUS | Switch immediately – ensure the patient has not had unprotected sex in the 7 days prior to the change | No |
These are often thought to be messy and difficult, and hence are used by <1% of ♀ in the UK. However, the ease of use and lack of interference with intercourse often surprises ♀. Must be used correctly and consistently, as typical failure rates in the first year can be high (12%). Should be fitted by a trained HCP who can advise about use of additional spermicide.
Physical and chemical barrier to sperm entering the upper female genital tract (when used with a spermicide). Diaphragms sit between the posterior fornix and the pubis to cover the cervix. Cervical caps fit directly over the cervix by suction and are ideal for ♀ with long cervices and ♀ with recurrent UTIs when using diaphragms.
• Effective with careful consistent use (6% failure rate with perfect use).
• Can be inserted anytime time before sex.
• No established health risks or systemic side effects.
• Silicone alternatives available for women with latex allergies.
• High failure rates in practice (12% with typical use), therefore, requires careful use on all occasions.
• Must remain in place for 6 hours after the last episode of sexual intercourse, but should stay in for no longer than 48 hours
• May become dislodged during sex.
• May risk of cystitis or UTI.
• Potential risk of TSS if left in situ longer than the recommended time specified by the manufacturer.
• Should be used with a spermicide. More spermicide should be inserted into the vagina if the cap/diaphragm has been in situ for over 3 hours or before repeated sex occurs to efficacy.
• Spermicide is considered ‘messy’ by some users.
• Spermicide-induced vaginal irritation in some users.
• Needs to be fitted by a HCP.
• May need to be re-fitted after certain circumstances, for example weight changes of ±3 kg and having a baby.
• Can become damaged by oil-based lubricants.
The female condom (Femidom®) was first marketed in the UK in 1992 but very few ♀ in the UK use this method. It can be bought in pharmacies and is acceptable to some ♀ who often alternate between using male and female barrier methods.
The female condom is a lubricated loose-fitting, polyurethane sheath with two flexible rings. The closed end with the loose ring is inserted into the vagina and the outer ring covers the vulva. It acts as a physical barrier between sperm and ovum.
• Acts as a contraceptive and may also protect against some STIs (inconsistent data).
• Theoretical benefit in helping to protect against HPV transmission and cancer of the cervix.
• Effective with careful use (5% failure rate with perfect use).
• Under direct control of the user.
• Can be inserted at any time before having sex.
• No additional spermicide required.
• Can be used with oil-based products.
• Polyurethane is stronger than latex and breakage is rare.
• No need for male erection before use.
• Has high failure rates in practice (typical failure rate 21%).
• Has a high slippage rate (about 6%).
• Requires thought before use and careful insertion to be effective.
One of the oldest forms of contraception. Available in the UK as creams and pessaries. Many different substances have been used in the past, but preparations available in the UK contain nonoxynol-9.
• Widely available in pharmacies and simple to use.
• Enhance efficacy of barrier methods.
• Useful during the peri-menopause (♀ >45 years with irregular cycles and some vasomotor symptoms).
• Can be used while breastfeeding (until menstruation returns and weaning begins).
• Must not be used as sole contraceptive in most circumstances (28% typical failure rate when used alone in fertile ♀).
• Can be messy and cause local irritation.
• Waiting time of approximately 4 minutes after insertion of pessaries before they melt.
• Those available may damage the vaginal epithelium and have the potential to transmission of STIs.
The condom or ‘sheath’ has been used to protect against transmission of STIs and prevent pregnancy over the centuries. It is still one of the most popular contraceptive methods and is used by 25% of British couples. They are readily available from a variety of outlets. Condoms must be used correctly and on all occasions when close sexual contact occurs to be effective. Typical failure rate is high (18%).
Male condoms come in different shapes, colours, sizes, and flavours. Most are made of latex, with the only contraindication being latex allergy. The majority of reactions are type IV hypersensitivity (mild genital inflammation), although rarely anaphylaxis can occur with type I hypersensitivity. Polyurethane, deproteinized latex, and polyisoprene condoms are available as alternatives. Condoms lubricated with a non-spermicidal agent are now advised since the addition of a spermicide may cause local genital irritation and thin the vaginal mucosa in ♀, leading to possible transmission of STIs. Additional spermicide does not improve the contraceptive efficacy of male condoms. Non-oil-based lubricants are recommended, especially for anal sex, to reduce the risk of breakage (3% breakage rate compared with 21.4% when lubricant is not used), but should not be applied directly to the penis under a condom as this may cause slippage.
Users should be advised to check their condoms for safety markings (CE markings or Kitemark) and expiry date.
• Acts as a physical barrier between sperm and ovum.
• No known serious side effects.
• Acts as a contraceptive and helps to provide protection against STIs and cervical neoplasia (Box 34.3).
• Effective with careful use (2% failure rate with perfect use).
• Latex-free condoms are available for those who have latex allergies.
• Under direct control of the user.
• High failure rates in practice.
• Transmission of STIs possible even with careful and consistent use.
• Oil-based lubricants and some vaginal preparations may affect latex condoms with risk of breakage. Aqueous-based lubricant should be used for anal sex to reduce the risk of breakage. ‘Stronger’ condoms result in similar breakage rates. Therefore, they are not recommended.
• Requires the penis to be erect before use.
• Has a high slippage rate if lubricant is placed in the condom.
Box 34.3 Male condoms and STI protection
Effective condom use reduces HIV transmission by 85% (meta-analysis data ranges between 73% and 96%)
Data on other STIs is inconsistent and the degree of protection provided by male condoms is difficult to assess. However:
• Gonorrhoea and chlamydia: strong evidence that condoms reduce the risk of gonorrhoea and chlamydia in both men and women (review of 45 published studies).
• Trichomoniasis: conflicting data; however, TV is more likely to be found in inconsistent condoms users; therefore, correct and regular condom use is recommended.
• Anogenital herpes: conflicting data. Evidence of protection using male condom for HSV-2 sero-discordant couples or those with >4 sex partners, but no evidence for sex workers, their clients, and GUM male heterosexual attenders. Consistent and correct use of male condoms is recommended.
• Syphilis: limited data regarding the usefulness of condoms exists, although regular and correct condom use is recommended to protect against syphilis transmission.
• Anogenital HPV: risk of cervical and vulvo-vaginal HPV infection reduced with consistent condom use. Regression and clearance of flat penile warts and cervical intra-epithelial neoplasia has also been reported in association with condom use.
• Hepatitis B virus: reduced core antibody rates in female sex workers who consistently use condoms.
Using condoms with sex toys will also decrease the risk of STI acquisition.
Estimated minimum level of protection against infection provided by consistent condom use:
• HSV infection in ♀ may be reduced but no evidence in ♂. Conflicting data on HPV infection but may incidence in ♂ and delay progression of CIN in ♀.
FAM has replaced the terms ‘rhythm method’, ‘natural family planning’, or using the ‘safe period’. FAM relies upon the detection of ovulation. It is effective if couples abstain from penetrative vaginal sex during the fertile period of the menstrual cycle or use a barrier method. Normally, a minimum of three menstrual cycles’ information is needed for accurate prediction of the fertile phase. Efficacy is improved if several FAMs are used concurrently, such as menstrual records, basal body temperature, and cervical mucus indicators. The failure rate is 6% with perfect use of devices such as Persona®, which detect the fertile phase by measuring urinary oestriol-3-glucuronide and LH.
Fertility awareness is used by 2% of couples in the UK, but by many more worldwide to space their family.
• Can be used to plan pregnancy, as well as prevent conception.
• If multiple methods are used together perfectly, the pregnancy rate may be as low as 4%.
• No known physical side effects.
• Non-intercourse-related method.
• No mechanical devices or hormones used.
• Acceptable to all cultures and religions.
• No follow-up is necessary once the user has learnt the method.
• Relatively high failure rate in practice, if only one fertility awareness method is used (24%).
• Requires commitment of both partners.
• Needs to be taught by a trained practitioner in order to use successfully.
• Requires careful observation and record-keeping, which may take time to learn.
• Users must have high motivation, as long periods of abstinence from intercourse are required.
• No protection against STI transmission.
Breastfeeding is a natural way of spacing children, since suckling suppresses LH and FSH, resulting in amenorrhoea, and stimulates prolactin, leading to lactation. LAM is very effective, offering 98% protection against pregnancy under the following conditions:
• Fully or almost fully breast-feeding (feeding with no substitutes and at regular periods on demand, day and night).
• Menstruation has not returned.
• Non-intercourse-related method.
• No mechanical devices or hormones used.
• Acceptable to all cultures and religions.
• Does not cause nausea or weight gain.
• Acceptable to many users and ‘natural’.
• Failure rate low when the woman fulfils all the conditions of LAM.
• Higher failure rate if the woman is supplementing with bottle feeding.
• No protection against STI transmission.
‘Withdrawal’ is the oldest method of birth control and is still one of the most popular natural contraceptive methods worldwide. In the UK 4% of couples use this method and it can be practiced by any couple at any time.
• Does not cause nausea or weight gain.
• High failure rate (22% in practice).
• May be unsatisfying for both partners.
• Partial ejaculation of semen can occur.
• No protection against STI transmission.
Emergency contraception (EC) involves methods that can be used in the event of UPSI to prevent pregnancy. These methods are not abortifacients as they do not disrupt implantation of the blastocyst.
Research began in the 1960s to develop post-coital contraception. A licensed preparation that became available in the UK in the early 1980s comprised two doses of 100 mcg ethinylestradiol and 500 mcg levonorgestrel to be taken within 72 hours of UPSI. We now know that progestogen-only emergency contraception containing 1500 mcg of levonorgestrel, taken in a single dose (Levonelle 1500® or branded generics) are more effective with fewer side effects.
Ulipristal acetate (EllaOne®), a selective progesterone receptor modulator, was launched in the UK in 2009. It has a similar mode of action to progestogen-only emergency contraception, but equally effective up to 5 days after UPSI.
Oral EC is now widely available with >50% being provided by a chemist or pharmacy, where it can be purchased or obtained ‘free at the point of contact’ through local patient group directions.
LNG-EC works by delaying ovulation, rather than preventing implantation of the blastocyst, if taken before the start of the LH surge. No effect if taken after this time. Thought to prevent about 70% of pregnancies; may be more effective if taken as soon as possible after UPSI.
Providers should inform users of likely mode of action, to dispel some of the myths that oral EC ‘causes abortions’, contains ‘dangerous hormones’, and can affect future fertility.
A single dose of LNG-EC is licensed to be taken up to 72 hours after an episode of UPSI, and can be given multiples times in the same cycle if need be. ♀ taking liver-enzyme-inducing drugs, such as carbamazepine or St John’s wort, should take two LNG-EC 1500 mcg tablets as a single dose. Additionally, women who weight more than 70 kg or have a BMI >26 kg/m2 should take double-dose LNG-EC if they are unable to be fitted with an IUD or take ulipristal acetate emergency contraception (UPA-EC).
LNG-EC is available from GPs, nurses, community settings, and pharmacies. It has few side effects and no known teratogenicity. It can be prescribed in advance for those using barrier methods or ‘perceived to be at risk’. It is the preferred oral EC option in women who are breast-feeding, wanting to ‘quick-start’ a hormonal method of contraception or require EC because of missed pills.
UPA-EC is a progesterone receptor modulator and works by stopping or delaying ovulation. It is effective throughout the fertile phase and at the start of the LH surge, but not once the LH surge has peaked. A single dose of UPA-EC can be taken up to 120 hours after UPSI and can be given more than once in the same cycle if needed. If taken within licensed indications, it will prevent 60–80% of pregnancies. UPA-EC is excreted in breastmilk, so if ♀ is breastfeeding, she must express and discard her breastmilk for the next 7 days. Not advisable to quick-start hormonal contraception for 5 days if UPA-EC has been taken, as its mode of action may be affected. Use of condoms or abstinence required during this time, until contraceptive method effective.
Also thought that hormonal contraception taken in the 7 days prior to taking UPA-EC will affect its action; therefore, LNG-EC or a copper IUD is the preferred choice.
UPA-EC is not recommended for use in women who are taking liver enzyme-inducing medication.
Copper IUD (Cu-IUD) is the most effective method, preventing almost 100% of pregnancies if fitted within 120 hours of the first episode of UPSI any time in a menstrual cycle or after multiple episodes of UPSI, but no later than 5 days after the estimated time of ovulation. Cu-IUDs must be used, rather than the LNG- IUS.
Cu-IUDs viability of the ova, sperm numbers reaching the fallopian tubes; may prevent implantation by inducing endometrial changes.
A Cu-IUD should be offered to all ♀ requesting EC, as it is the most effective choice. However, oral EC should be prescribed if referral elsewhere is necessary or there is likely to be a delay in fitting a Cu-IUD. This will ensure that a method of EC has been provided if Cu-IUD insertion fails or the appointment is not kept.
• Suitable following multiple episodes of UPSI, but within 5 days after the estimated time of ovulation.
• Appropriate if vomiting follows oral EC.
• Ideal choice if requested as a long-term contraceptive method.
• Effective contraception for rest of menstrual cycle.
• Most effective method, especially if UPSI occurs close to the time of ovulation.
• Similar to Cu-IUDs used as a long-term contraceptive method.
• Possible pain at insertion, particularly if nulliparous.
• Some women perceive the fitting of an IUD to be ‘invasive’.
• Risk of pelvic infection within the first 20 days. ▶ Screen for STIs prior to fitting. Some may consider antibiotic cover, while awaiting results in high-risk groups.
• Does not protect against STI transmission.
Male and female sterilization is the main method of contraception for ~17% of couples in England and Wales. Female sterilization is normally performed as a day-case procedure. Regarded as permanent, as reversal, which requires surgery, may not be 100% successful.
Counsel use of effective contraception prior to surgery as up to 3% of ♀ may be pregnant at the time of sterilization. Sterilization should be postponed if there is any risk of pregnancy. Avoid routine sterilization immediately post-partum, post-abortion, or without considering other reversible options. Female sterilization has by >50% over the last 20 years, with the introduction of LARC.
Occlusion of fallopian tubes blocking the sperm and preventing fertilization. If done at laparoscopy or laparotomy, tubes are occluded by using clips, rings, or excising a part of the tube. If done hysteroscopically, micro-inserts placed into the tubes via the ostia. Hysteroscopic sterilization (Essure®) was discontinued in the UK in 2017.
• Highly and immediately effective.
• High user satisfaction, removing fear of unplanned pregnancy.
• Requires a general anaesthetic.
• Reversal requires a major surgical procedure and is not funded by the NHS.
• Other hormonal contraceptive methods are equally effective, and are reversible with additional non-contraceptive benefits.
• Has associated complications in 0.9–1.6 per 100 cases, with clips having the lowest complication rate of 0.47 per 100 cases (Box 34.4).
Box 34.4 Complications of female sterilization
• Anaesthetic complications: overall mortality from anaesthetic complications is very low.
• Operative complications: occur in 0.5–1% of procedures.
• Perforation of bowel, blood vessels, or bladder at the time of the procedure: the need for laparotomy as a result of a serious complication is about 1.9 per 1000 procedures and risk of death is 1 in 12,000 laparoscopies.
• Abdominal discomfort and shoulder tip pain: from intra-peritoneal gas still remaining in the abdominal cavity. This slowly improves over 24–48 hours.
• Late re-canalization of fallopian tubes: Failure rates with Filshie clips are quoted as 2–3 per 1000 procedures. Occurs even up to 10 years after surgery with a cumulative ectopic pregnancy rate being as high as 31.9 per 1000 procedures, depending on the sterilization method used.
• Complaints of heavy menstrual bleeding leading to hysterectomy: Women often stop hormonal methods of contraception that have controlled their menstrual loss and pain. With advancing age, menstrual problems and this can lead to requests for treatment. There is a 17% cumulative probability of undergoing a hysterectomy when reviewed 14 years after female sterilization.
• Regret: not uncommon following sterilization, with 3–10% of couples reporting this. Regret is more common when the operation has been performed in those <30 years old and within a year of the birth of a child.
In the UK ~11% of couples rely on male sterilization as their chosen method of contraception, with ~60% of all sterilization procedures performed on ♂. This ratio is different in other parts of the world, with ♀ ×10 more likely to be sterilized than their ♂ counterparts.
Male sterilization techniques in the UK aim to divide the vas deferens using ligation or coagulation, usually under local anaesthetic.
• Very safe and effective with a failure rate of ~1/2000 in a lifetime after a negative ‘clearance of sperm’ test done at 12 weeks.
• Permanent method ameliorating concerns about future contraception or unplanned pregnancy.
• Minor surgical procedure, normally performed under local anaesthetic and taking 10–15 minutes.
• Can be done at a doctor’s surgery or clinic.
• No evidence of i risk of testicular/prostate cancer.
• No increased risk of coronary heart disease.
• Reversal is not easy and is not funded by the NHS.
• Couples may regret this decision, especially if they are young (<30 years old).
• Not immediately effective, requiring a negative semen analysis before other methods can be abandoned.
• Surgical procedure with associated complications (Box 34.5).
Box 34.5 Complications of male sterilization
• Local complications: bruising and swelling with some discomfort or pain for a short time following the procedure. Scrotal haematoma formation occurs in 1–2% following vasectomy.
• Wound infection: in <2%. May require antibiotic treatment.
• Failure to achieve azoospermia: in ~0.5%. Further surgery may be required.
• Sperm granulomata: small tender lumps that form at the cut ends of the vas deferens, caused by leakage of sperm into the tissue from the cut ends, leading to local inflammation. Can be excised.
• Chronic scrotal pain: ~10% complain of chronic scrotal pain following vasectomy. May be made worse by sexual arousal or ejaculation. Local scar tissue formation and induration may be the cause. Further surgery to remove the epididymis and occluded vas may be indicated in some.
• The vast majority of ♀ infected with HIV are of reproductive age, with many relying solely on barrier methods and, therefore, at risk of an unplanned pregnancy.
• Effects of some antiretrovirals on the foetus may be severe (e.g. efavirenz, resulting in anencephaly in animal studies). Long-term effects are unknown, with concerns over haematological, metabolic and neurological abnormalities, and mitochondrial dysfunction.
• Drug interactions between hormonal contraceptives, some antiretrovirals and certain antibiotics. For up-to-date information, consult the online HIV drug interaction tracker:  http://www.hiv-druginteractions.org (Box 34.6).
http://www.hiv-druginteractions.org (Box 34.6).
• Possible HIV transmission to the ♂ partner.
Box 34.6 Interactions and hormonal contraception
• Rifampicin and rifabutin: powerful enzyme inducers.
• CHC—efficacy reduced therefore use not advised
• POP—efficacy reduced, therefore, use not advised
• Implant—efficacy reduced, therefore, not recommended
• Broad-spectrum antibiotics: not affected.
• All nucleoside reverse transcriptase inhibitors, including Combivir® and Truvada®, can be used safely.
• Efavirenz not compatible with oral methods, but DMPA is OK.
• Always check for antiretroviral drug interactions to identify potential drug interactions ( www.hiv-druginteractions.org).
Can be recommended for use by all HIV +ve ♀ and ♂, preferably in combination with another contraceptive method, if contraception is essential. If ♂ condom is unacceptable, consider ♀ condom.
Both are safe in HIV infection, as operative risks are no greater than in those who are HIV –ve. However, if complications occur, they could be more serious in those with advanced HIV disease and so other methods may be more acceptable. Caution should also be exercised in newly diagnosed patients who may be coming to terms with their condition and could change their views with regard to future pregnancies. A longer-term reversible method may be preferable.
There are no HIV-specific contraindications in those who are well and not on any treatment. Care must be taken to avoid any potential drug interactions.
As with CHCs, there are no specific contraindications, but care needs to be taken to avoid drug interactions.
DMPA’s efficacy is not affected by anti-retrovirals and the injection interval does not require altering from the standard 13 weeks. Some antiretrovirals may adversely affect bone mineral density, therefore, other progestogen-only contraceptive options may be preferred.
• Cu-IUDs are highly effective and cost-effective.
• LNG-IUS are highly effective and can be used to treat menstrual problems, which are frequently seen in the Black African population.
• There are no drug interactions.
• IUD/IUS can be used without limitation in women whose CD4 count is >200 cells/mm3.
• In women whose CD4 count is <200 cells/mm3 IUD/IUS should be fitted with caution, although there is no issue with continuing to use the method if it is already in situ.
• Risks of complications and pelvic infection following IUD/IUS insertion are thought to be similar to those in HIV –ve ♀
• IUD/IUS use is not associated with risk of HIV transmission to a non-infected partner.
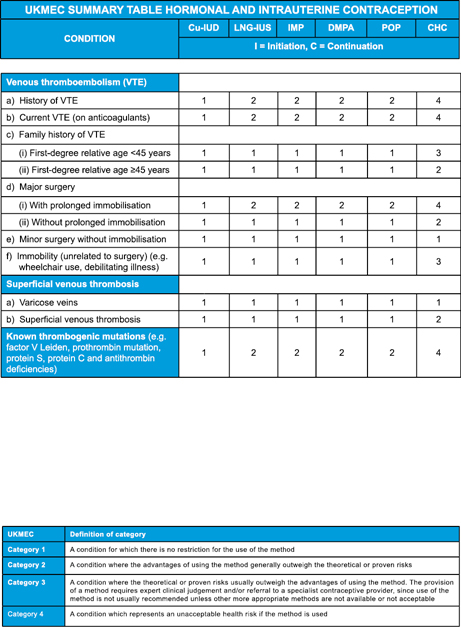
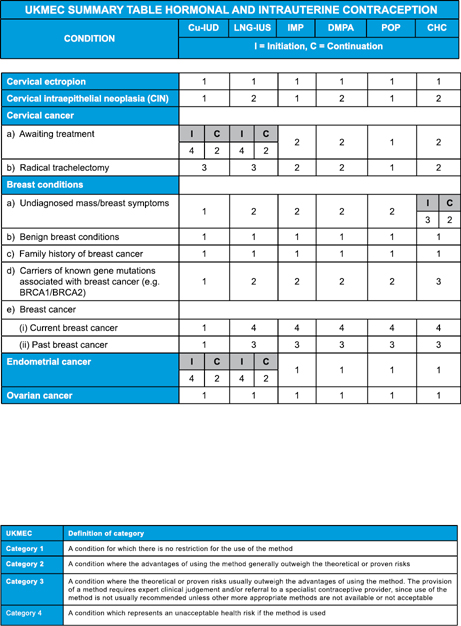
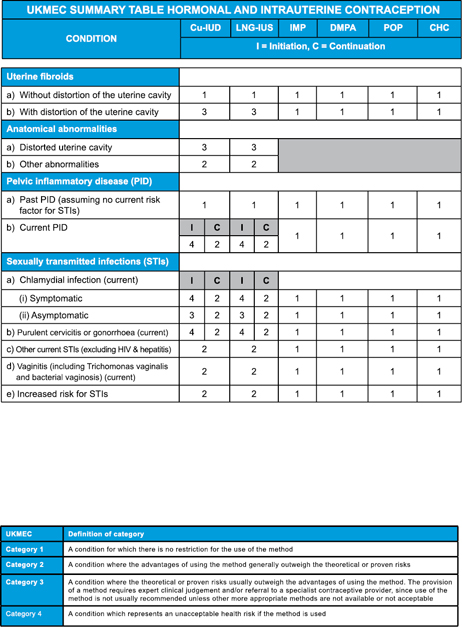
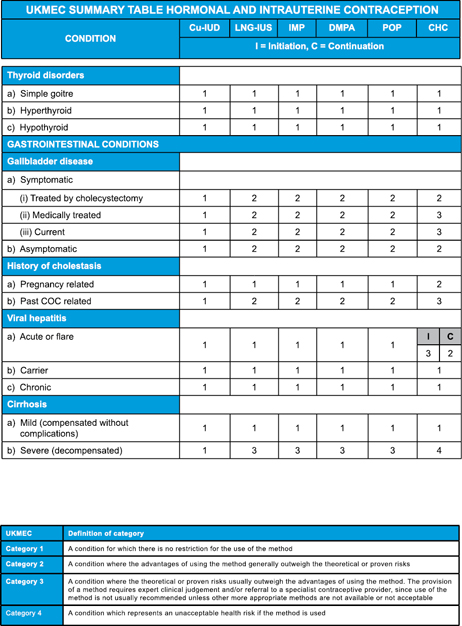
The UK Medical Eligibility Criteria for contraceptive use has adapted WHO guidance, and classifies the acceptability of each contraceptive method in different conditions into one of four categories.
• Category 1: a condition for which there is no restriction on the use of the contraceptive method.
• Category 2: a condition where the advantages of using the method generally outweigh the theoretical or proven risks.
• Category 3: a condition where the theoretical or proven risk generally outweighs the advantages of using the method. The provision of a method requires expert clinical judgement and/or referral to a specialist contraceptive provider, since use of the method is not usually recommended, unless other more appropriate methods are not available or not acceptable.
• Category 4: a condition that represents an unacceptable health risk if the contraceptive method is used.
UKMEC guidelines are summarized in Table 34.8.
Table 34.8 UK Medical eligibility criteria for contraceptive use guidelines (UKMEC) 2016*
|
|
Further information
UK Medical Eligibility Criteria for contraceptive use (UKMEC) 2016 Summary tables https://www.fsrh.org/standards-and-guidance/documents/ukmec-2016-summary-sheets/
Faculty of Sexual and Reproductive Health guidelines https://www.fsrh.org/standards-and-guidance/current-clinical-guidance/