Environments of Care |
6 |
Preventing falls and traumas is an important issue for nurses caring for older adults. Falls among older adults in every care setting are a large national problem. Approximately one-third of older adults living at home and up to two-thirds of older adults in long-term care facilities fall each year. When an older adult falls, the consequences may be devastating.
![]() They are likely to develop a fracture.
They are likely to develop a fracture.
![]() This may begin a spiral of iatrogenesis.
This may begin a spiral of iatrogenesis.
![]() The result may be death.
The result may be death.
The National Center for Health Statistics annual mortality report shows that fall-related deaths among older adults increased sharply between 1998 and 2006. Older men tend to die from falls; older women experience more hospitalizations for fall-related hip fracture. Normal changes of aging contribute to falls, including
![]() Visual and hearing declines
Visual and hearing declines
![]() Changes in urinary function
Changes in urinary function
Pathological aging changes also contribute to falls, including
![]() Cognitive disorders
Cognitive disorders
![]() Osteoporosis
Osteoporosis
![]() Strokes
Strokes
![]() Sensory impairments
Sensory impairments
The highest risk factor for an older adult having a fall is a history of a previous fall.
![]() Fall prevention is critical to preventing the negative consequences of falling among older adults.
Fall prevention is critical to preventing the negative consequences of falling among older adults.
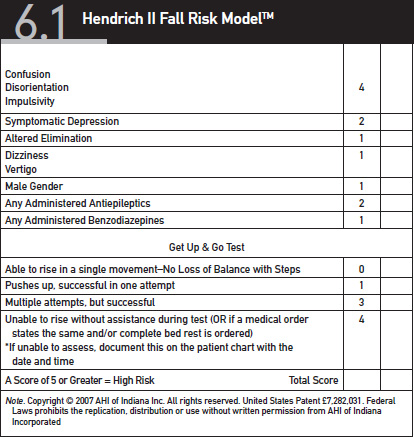
![]() Prevention begins with assessment (see Table 6.1).
Prevention begins with assessment (see Table 6.1).
![]() Prevention strategies include
Prevention strategies include
![]() Removal of fall hazards such as area rugs
Removal of fall hazards such as area rugs
![]() Appropriate nonglaring lighting
Appropriate nonglaring lighting
![]() Wall-to-wall carpeting or padding on the floor next to the bed
Wall-to-wall carpeting or padding on the floor next to the bed
![]() Bed and chair alarms to alert caregivers of older adult mobility
Bed and chair alarms to alert caregivers of older adult mobility
Despite the high risk and negative consequences of falls among older adults, restraints are not a reasonable fall prevention intervention. A physical restraint is defined as a device or object attached or adjacent to a person’s body that cannot be removed easily and restricts freedom of movement. Several types of restraints are available.
![]() Physical restraints
Physical restraints
![]() Side rails on hospital beds
Side rails on hospital beds
![]() Jackets
Jackets
![]() Belts
Belts
![]() Wrist restraints
Wrist restraints
![]() Chemical restraints
Chemical restraints
![]() Sedatives
Sedatives
![]() Hypnotics
Hypnotics
Evidence about the negative effects of the use of restraints is so disturbing that the mandate for restraint-free care can no longer be ignored. Significant morbidity and mortality risk—including asphyxiation and strangulation—is associated with the use of physical restraints, especially when patients are
![]() Confused
Confused
![]() Agitated
Agitated
![]() Experiencing new onset pressure ulcer
Experiencing new onset pressure ulcer
![]() Suffering from pneumonia
Suffering from pneumonia
![]() Neurologically impaired
Neurologically impaired
Older adults should only be restrained if they are in immediate, physical danger or are hurting themselves or others and then for only a brief period of time. The Omnibus Budget Reconciliation Act of 1987 attempted to curtail restraint use in long-term care facilities. Restraint alternatives should be implemented to keep residents safe from falls.
![]() Wall-to-wall carpeting
Wall-to-wall carpeting
![]() Mattress placed on the floor
Mattress placed on the floor
![]() Personal attendants
Personal attendants
![]() Chair or bed alarms
Chair or bed alarms
Due to normal and pathological aging, including reduction in the number of pyrogenes, older adults tend to have difficulty regulating heat and cold. Many older adults die each year from hyperthermia-related heat stroke in the summer due to exposure to extreme temperatures and inability to regulate heat though sweating. Heat stroke is the most serious form of hyperthermia and may result in death if not treated immediately. Many older adults also die each year from hypothermia, which could be reduced through exercise among older adults.
Older adults reside in a variety of care environments:
![]() Home
Home
![]() Senior housing
Senior housing
![]() Nursing home
Nursing home
![]() Assisted living
Assisted living
![]() Continuing care retirement communities
Continuing care retirement communities
![]() The street
The street
Relocation is a significant life event that may play a role in the development or severity of depression among older adults. Relocation of older adults occurs commonly as a result of
![]() Illness
Illness
![]() Decline in functional status
Decline in functional status
![]() Loss of spouse or significant other
Loss of spouse or significant other
![]() Changes in economic status caused by retirement or the death of the family provider
Changes in economic status caused by retirement or the death of the family provider
Because of the negative consequences of relocation, aging in place is emphasized as a concept that refers to remaining in one setting throughout the majority of older adulthood.
Translocation syndrome results from a change in surroundings from a home to a nursing home or assisted living facility and may trigger the onset of delirium. The syndrome may manifest as
![]() Impaired physical health
Impaired physical health
![]() Depression
Depression
![]() Disruption of established behavior patterns
Disruption of established behavior patterns
![]() Disruption of social relationships
Disruption of social relationships
Translocation from one environment to another may potentially upset the patient. Attempting to transition the patient smoothly to his or her new environment is important.
![]() Letting older adults bring favorite things to their new environment helps them transition more effectively.
Letting older adults bring favorite things to their new environment helps them transition more effectively.
![]() Empowering older adults as much as possible by allowing them to make decisions and articulate needs and desires is a critical factor in assisting their adjustment from one environment to another.
Empowering older adults as much as possible by allowing them to make decisions and articulate needs and desires is a critical factor in assisting their adjustment from one environment to another.
![]() One intervention is to orient the patient regularly and to reassure his or her safety.
One intervention is to orient the patient regularly and to reassure his or her safety.
Translocation syndrome is likely to happen during admission to a nursing home or transfer to acute care from a nursing home environment.
![]() Close attention to the transition of an older adult across environments of care is essential to minimize the symptoms of translocation syndrome.
Close attention to the transition of an older adult across environments of care is essential to minimize the symptoms of translocation syndrome.
![]() Older adults must continually be assessed for alterations in function and cognition and be supported to participate in the environment at the highest possible level.
Older adults must continually be assessed for alterations in function and cognition and be supported to participate in the environment at the highest possible level.
![]() Changes in function, cognition, and affect must be diagnosed immediately and appropriate interventions implemented to ensure as safe a transition as possible.
Changes in function, cognition, and affect must be diagnosed immediately and appropriate interventions implemented to ensure as safe a transition as possible.
![]() Little research is available regarding relocation stress and translocation of older adults.
Little research is available regarding relocation stress and translocation of older adults.
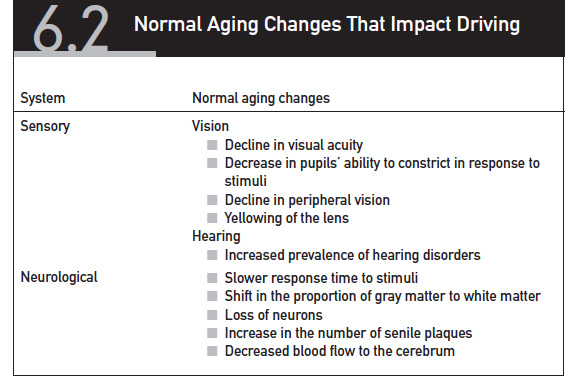
Many older adults continue to drive. As the percentage of older adults living in the United States continues to increase, the number of older drivers will also rise. The risk for injuries, hospitalizations, and death from automobile accidents is increased in the older adult population because of the many normal and pathological changes in the neuromuscular and sensory systems, listed in Table 6.2. The number of elderly traffic fatalities is expected to more than triple by the year 2030, exceeding the number of alcohol-related fatalities in 1995 by 35% (Burkhardt, Berger, Creedon, & McGavock, 1998).
The growth in the number of older drivers presents additional problems, because cars, roads, and highways were not developed to accommodate normal changes of aging among older drivers. A large number of older adults thus are unable to safely drive. Driving presents a significant ethical issue of independence among older adults that should not be taken lightly. Older adults who no longer drive face significant issues with transportation. Older adults need transportation for
![]() Health care appointments
Health care appointments
![]() Shopping for food and essentials
Shopping for food and essentials
![]() Socialization
Socialization
Although van services are available in many communities to transport older adults, they are not universally available.
![]() Car and van services usually require advanced scheduling on a first-come, first-served basis.
Car and van services usually require advanced scheduling on a first-come, first-served basis.
![]() Older adults sometimes have to wait for a long time at a health care facility or physician’s office for the van to return to bring them home, extending a short appointment to a day-long outing.
Older adults sometimes have to wait for a long time at a health care facility or physician’s office for the van to return to bring them home, extending a short appointment to a day-long outing.
![]() Public transportation such as buses or subway systems may be used by older adults to attend their medical appointments.
Public transportation such as buses or subway systems may be used by older adults to attend their medical appointments.
![]() Public transportation systems have increased accessibility to accommodate disabilities among older adults.
Public transportation systems have increased accessibility to accommodate disabilities among older adults.
![]() Long walks to bus or subway stations may be barriers to public transportation system utilization among the elderly.
Long walks to bus or subway stations may be barriers to public transportation system utilization among the elderly.
![]() Caregivers, friends, and neighbors are often relied upon for transportation among older adults.
Caregivers, friends, and neighbors are often relied upon for transportation among older adults.
![]() The barriers presented by transportation to health care facilities often force older adults to delay medical treatment for health-related issues.
The barriers presented by transportation to health care facilities often force older adults to delay medical treatment for health-related issues.
![]() Lack of transportation to purchase food may contribute to malnutrition among older adults.
Lack of transportation to purchase food may contribute to malnutrition among older adults.
Most older adults prefer to stay in their own home rather than move to other care environments. Approximately 94% of older adults live in community households, either alone or with a relative. Of the 94% that live in the community, most live alone or with a spouse. Living in the same home environment through life has advantages and disadvantages. Some of the advantages are
![]() Ownership and control of one’s space and territory
Ownership and control of one’s space and territory
![]() The ability to remain among neighbors who share memories and now watch out for each other
The ability to remain among neighbors who share memories and now watch out for each other
![]() The opportunity to function as parents or grandparents to new families who move into the neighborhood
The opportunity to function as parents or grandparents to new families who move into the neighborhood
Some of the disadvantages of remaining at home:
![]() Many homes require costly and difficult repairs and maintenance that some older adults can no longer afford or manage.
Many homes require costly and difficult repairs and maintenance that some older adults can no longer afford or manage.
![]() Decline in functional status, vision, and hearing can make adaptation to a home and socialization difficult.
Decline in functional status, vision, and hearing can make adaptation to a home and socialization difficult.
![]() Medical care and assistance with activities of daily living and instrumental activities of daily living are not built into the home.
Medical care and assistance with activities of daily living and instrumental activities of daily living are not built into the home.
![]() Older adults typically have to leave home to obtain care or hire outside providers.
Older adults typically have to leave home to obtain care or hire outside providers.
![]() The latter may be costly, and expenses are not always covered by Medicare and private insurance.
The latter may be costly, and expenses are not always covered by Medicare and private insurance.
![]() Although they may not be reimbursable, many health care services are available in the home, including
Although they may not be reimbursable, many health care services are available in the home, including
![]() Nursing
Nursing
![]() Physical therapy
Physical therapy
![]() Occupational therapy
Occupational therapy
![]() Speech-language pathology
Speech-language pathology
![]() Assistance with personal care
Assistance with personal care
![]() Social work
Social work
If an older adult can no longer live at home, attention should be given to protection of his or her territory and personal space in alternate care settings. Territoriality involves setting boundaries to protect one’s personal space. Nurses may help older adults protect their territoriality by
![]() Suggesting they bring personal items to the new space
Suggesting they bring personal items to the new space
![]() Preventing other staff and residents from invading personal space or crossing boundaries
Preventing other staff and residents from invading personal space or crossing boundaries
![]() Encouraging time in personal space
Encouraging time in personal space
![]() Assessing the amount of personal space, the comfort with eye contact, and the use of physical gestures such as hand-shaking to determine the older adult’s comfort with these common social norms
Assessing the amount of personal space, the comfort with eye contact, and the use of physical gestures such as hand-shaking to determine the older adult’s comfort with these common social norms
Generally, older adults are formally assessed by an agency to determine their need for home care services. Medicare uses the OASIS (outcome and assessment information set) to evaluate possible recipients of home care services. OASIS is a set of data elements that forms a comprehensive assessment for an adult home care patient and provides the basis for measuring patient outcomes for purposes of outcome-based quality improvement. Other community resources funded through grants distributed through Area Agencies on Aging or the federal government include
![]() Employment resources
Employment resources
![]() Senior center programs
Senior center programs
![]() Adult day care services
Adult day care services
![]() Alternative community-based living facilities
Alternative community-based living facilities
It is estimated that family members provide approximately 80% of the care for older adults. Caregiving places a tremendous burden on the caregiver that may result in
![]() Depression
Depression
![]() Grief
Grief
![]() Fatigue
Fatigue
![]() Decreased socialization
Decreased socialization
![]() Health problems
Health problems
Respite care for older adults may be found in a local skilled nursing facility so that the caregiver may vacation and rest. Other supportive services may help to ease caregiver burden, such as
![]() Home health aides
Home health aides
![]() Homemakers
Homemakers
![]() Chore services
Chore services
![]() Meals on Wheels
Meals on Wheels
Caregivers must be encouraged and supported to take care of themselves and pursue their own interests and activities.
Several types of residential facilities perform care for older adults.
Skilled nursing facilities (SNFs) may be private or public and may receive reimbursement from Medicare, Medicaid, and private insurances, or residents may self-pay.
![]() Nursing services provided in SNFs may include
Nursing services provided in SNFs may include
![]() Medication administration
Medication administration
![]() Wound care
Wound care
![]() Daily assessment
Daily assessment
![]() Meals
Meals
![]() Assistance with activities of daily living
Assistance with activities of daily living
![]() Physical therapy
Physical therapy
![]() Respiratory therapy
Respiratory therapy
![]() Speech-language pathology services
Speech-language pathology services
![]() Occupational therapy
Occupational therapy
![]() Short-term rehabilitation after surgery or medical illness
Short-term rehabilitation after surgery or medical illness
![]() Lifetime residential services
Lifetime residential services
The documentation specific to skilled nursing facilities is known as the Minimum Data Set (MDS). This is a core set of screening, clinical, and functional status elements, including common definitions and coding categories.
![]() The MDS is the foundation of the comprehensive assessment for all residents of long-term care facilities certified to participate in Medicare or Medicaid.
The MDS is the foundation of the comprehensive assessment for all residents of long-term care facilities certified to participate in Medicare or Medicaid.
![]() The MDS standardizes communication about resident problems and conditions within facilities, between facilities, and between facilities and outside agencies.
The MDS standardizes communication about resident problems and conditions within facilities, between facilities, and between facilities and outside agencies.
Assisted living facilities (ALFs) were developed in the 1980s to provide supportive residential housing for the rapidly growing elderly population. ALFs place a greater emphasis on autonomy. They are appealing housing alternatives to older adults with minor to moderate functional impairments. ALFs generally follow a nonmedical, homelike model, focusing on resident
![]() Autonomy
Autonomy
![]() Privacy
Privacy
![]() Independence
Independence
![]() Dignity
Dignity
![]() Respect
Respect
ALFs are less expensive than SNFs, but the nonmedical model also precludes reimbursement by Medicare. Medicare reimbursement for home care services may be provided by an outside home care agency. Services offered at ALFs vary, but often include
![]() 24-hour supervision
24-hour supervision
![]() Three meals a day plus snacks in a dining room setting
Three meals a day plus snacks in a dining room setting
![]() A range of personal, health care, and recreational services
A range of personal, health care, and recreational services
Services may be included in the monthly rate, or they may be offered at additional costs. Health care and nursing services available at ALFs vary widely throughout the country. Some facilities have adequate 24-hour coverage, while others do not have registered nurses on site. Disparities in state regulations have led to varied interpretations of what ALFs are and what they can do.
Continuing care retirement communities (CCRCs) are defined as “full service communities offering long-term contracts that provide for a continuum of care, including retirement, assisted living and nursing services, all on one campus” (New Life Styles, 2005). They are a housing alternative for older adults that arose in the 1980s with the purpose of facilitating aging in place. CCRCs provide several levels of care, including
![]() Independent living
Independent living
![]() Assisted living
Assisted living
![]() Skilled nursing care
Skilled nursing care
Older adults may remain in the community by changing the level of care they receive as changes occur in their health, functional, or cognitive status. CCRCs are very expensive and require an entrance fee and a monthly payment. However,
![]() Skilled levels of care are reimbursable under Medicare.
Skilled levels of care are reimbursable under Medicare.
![]() Independent and assisted living are privately paid.
Independent and assisted living are privately paid.
![]() Periodic home care services may be reimbursable under Medicare by home care nurses.
Periodic home care services may be reimbursable under Medicare by home care nurses.
Residence in a CCRC requires a commitment to a long-term contract that specifies the housing, services, and nursing care provided. AARP (2007) reports that there are three types of CCRC contracts:
![]() Extensive contracts include unlimited long-term nursing care at minimal or no increase in monthly fee.
Extensive contracts include unlimited long-term nursing care at minimal or no increase in monthly fee.
![]() Modified contracts include a specified amount of long-term care. If chronic conditions require more care beyond the specified time, the older adult is responsible for payments.
Modified contracts include a specified amount of long-term care. If chronic conditions require more care beyond the specified time, the older adult is responsible for payments.
![]() With fee-for-service contracts, the older adult pays the full daily rates for long-term nursing care.
With fee-for-service contracts, the older adult pays the full daily rates for long-term nursing care.
CCRCs originated from religious or social groups interested in caring for members of their communities. More recently, private investors have begun to purchase and operate these communities. Services provided depend on the level of care and range from
![]() Basic recreational services in independent living to
Basic recreational services in independent living to
![]() Full care and meals in a skilled nursing environment
Full care and meals in a skilled nursing environment
Homelessness is a significant problem among the older adult population. Little is known about the homeless older population because they rarely seek health services, and thus they are difficult to access. The few available studies estimate that there are between 60,000 and 400,000 older homeless adults in the United States. The typical older homeless person is a man. Despite the lack of health service use among older homeless adults, this population suffers from
![]() Mental illness
Mental illness
![]() Alcohol abuse
Alcohol abuse
![]() Drug abuse
Drug abuse
These risk factors increase the prevalence of the following conditions among homeless older adults:
![]() Morbidity
Morbidity
![]() Mortality
Mortality
![]() Decreased bone density
Decreased bone density
![]() Malnutrition
Malnutrition
![]() Hip fracture from falls
Hip fracture from falls
![]() Motor vehicle accidents
Motor vehicle accidents
American Association of Retired Persons (AARP). (2007). Continuing care retirement communities. Retrieved July 14, 2007, from http://www.aarp.org/families/housing_choices/other_options/a2004-02-26-retirementcommunity.html
Burkhardt, J. E., Berger, A. M., Creedon, M., & McGavock, A. T. (1998). Mobility and independence: Changes and challenges for older drivers. Washington, DC: Department of Health and Human Services (DHHS), under the auspices of the Joint DHHS/DOT Coordinating Council on Access and Mobility.
New Life Styles. (2005). Types of senior housing and care. Retrieved August 25, 2007, from http://www.newlifestyles.com/resources/articles/Selecting_a_Continuing.aspx