CHAPTER 23
Status Epilepticus
Defined as continuous seizures or repetitive, discrete seizures with impaired consciousness in the interictal period. The duration of seizure activity to meet the definition has traditionally been 15–30 min. A more practical definition is any situation requiring the acute use of anticonvulsants; in generalized convulsive status epilepticus (GCSE), this is typically when seizures last >5 min.
CLINICAL FEATURES
Has numerous subtypes: GCSE (e.g., persistent, generalized electrographic seizures, coma, and tonic-clonic movements), and nonconvulsive status epilepticus (e.g., persistent absence seizures or focal seizures, confusion, or partially impaired consciousness, and minimal motor abnormalities). GCSE is obvious when overt convulsions are present, but after 30–45 min of uninterrupted seizures, the signs may become increasingly subtle (mild clonic movements of the fingers; fine, rapid movements of the eyes; or paroxysmal episodes of tachycardia, pupillary dilatation, and hypertension). EEG may be the only method of diagnosis with these subtle signs; therefore, if a pt remains comatose after a seizure, EEG should be performed to exclude ongoing status epilepticus. GCSE is life-threatening when accompanied by cardiorespiratory dysfunction, hyperthermia, and metabolic derangements such as acidosis (from prolonged muscle activity). Irreversible neuronal injury may occur from persistent seizures, even when a pt is paralyzed from neuromuscular blockade.
ETIOLOGY
Principal causes of GCSE are antiepileptic drug withdrawal or noncompliance, metabolic disturbances, drug toxicity, CNS infections, CNS tumors, refractory epilepsy, and head trauma.
TREATMENT Status Epilepticus
GCSE is a medical emergency and must be treated immediately.
• First attend to any acute cardiorespiratory problems or hyperthermia.
• Perform a brief medical and neurologic exam, establish venous access, and send labs to screen for metabolic abnormalities including anticonvulsant levels if pt has a history of epilepsy.
• Anticonvulsant therapy should then begin without delay (Fig. 23-1)
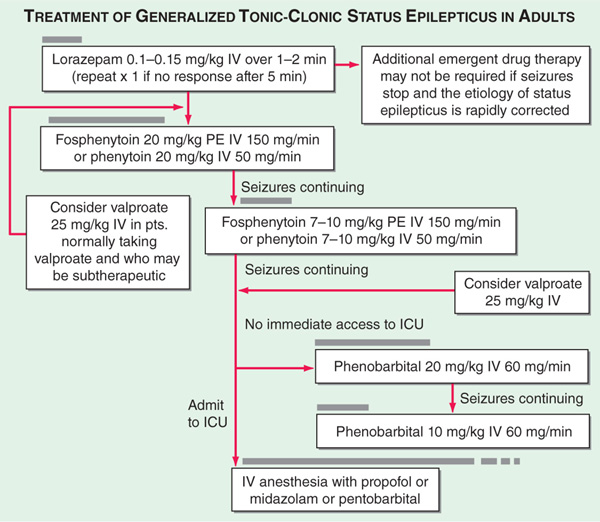
FIGURE 23-1 Pharmacologic treatment of generalized tonic-clonic status epilepticus in adults. The horizontal gray bars indicate the approximate duration of drug infusions. IV, intravenous; PE, phenytoin equivalents.
• In parallel, it is essential to determine the cause of the seizures to prevent recurrence and treat any underlying abnormalities.
The treatment of nonconvulsive status epilepticus is somewhat less urgent since the ongoing seizures are not accompanied by the severe metabolic disturbances of GCSE; however, evidence points to local cellular injury in the region of the seizure focus, so the condition should be treated as promptly as possible using the general approach for GCSE.
PROGNOSIS
The mortality rate is 20% in GCSE, and the incidence of permanent neurologic sequelae is 10–50%.

For a more detailed discussion, see Lowenstein DH: Seizures and Epilepsy, Chap. 369, p. 3251, in HPIM-18.