Renal calculi are common, affecting ~1% of the population, and recurrent in more than half of pts. Stone formation begins when urine becomes supersaturated with insoluble components due to (1) low urinary volume, (2) excessive or insufficient excretion of selected compounds, or (3) other factors (e.g., urinary pH) that diminish solubility. Approximately 75% of stones are Ca-based (the majority Ca oxalate; also Ca phosphate and other mixed stones), 15% struvite (magnesium-ammonium-phosphate), 5% uric acid, and 1% cystine, reflecting the metabolic disturbance(s) from which they arise.
Stones in the renal pelvis may be asymptomatic or cause hematuria alone; with passage, obstruction may occur at any site along the collecting system. Obstruction related to the passing of a stone leads to severe pain, often radiating to the groin, sometimes accompanied by intense visceral symptoms (i.e., nausea, vomiting, diaphoresis, light-headedness), hematuria, pyuria, urinary tract infection (UTI), and, rarely, hydronephrosis. In contrast, stag-horn calculi, associated with recurrent UTI with urea-splitting organisms (Proteus, Klebsiella, Providencia, Morganella, and others), may be completely asymptomatic, presenting with loss of renal function.
Most stones are composed of Ca oxalate. These may be associated with hypercalciuria and/or hyperoxaluria. Hypercalciuria can be seen in association with a very high-Na diet, loop diuretic therapy, distal (type I) renal tubular acidosis (RTA), sarcoidosis, Cushing’s syndrome, aldosterone excess, or conditions associated with hypercalcemia (e.g., primary hyperparathyroidism, vitamin D excess, milk-alkali syndrome), or it may be idiopathic.
Hyperoxaluria may be seen with intestinal (especially ileal) malabsorption syndromes (e.g., inflammatory bowel disease, pancreatitis), due to reduced intestinal secretion of oxalate and/or the binding of intestinal Ca by fatty acids within the bowel lumen, with enhanced absorption of free oxalate and hyperoxaluria. Ca oxalate stones may also form due to (1) a deficiency of urinary citrate, an inhibitor of stone formation that is underexcreted with metabolic acidosis; and (2) hyperuricosuria (see below). Ca phosphate stones are much less common and tend to occur in the setting of an abnormally high urinary pH (7–8), usually in association with a complete or partial distal RTA.
Struvite stones form in the collecting system when infection with urea-splitting organisms is present. Struvite is the most common component of staghorn calculi and obstruction. Risk factors include previous UTI, nonstruvite stone disease, urinary catheters, neurogenic bladder (e.g., with diabetes or multiple sclerosis), and instrumentation.
Uric acid stones develop when the urine is saturated with uric acid in the presence of an acid urine pH; pts typically have underlying metabolic syndrome and insulin resistance, often with clinical gout, associated with a relative defect in ammoniagenesis and urine pH that is <5.4 and often <5.0. Pts with myeloproliferative disorders and other causes of secondary hyperuricemia and hyperuricosuria due to increased purine biosynthesis and/or urate production are at risk for stones if the urine volume diminishes. Hyperuricosuria without hyperuricemia may be seen in association with certain drugs (e.g., probenecid, high-dose salicylates).
Cystine stones are the result of a rare inherited defect in renal and intestinal transport of several dibasic amino acids; the overexcretion of cystine (cysteine disulfide), which is relatively insoluble, leads to nephrolithiasis. Stones begin in childhood and are a rare cause of staghorn calculi; they occasionally lead to end-stage renal disease. Cystine stones are more likely to form in acidic urinary pH.
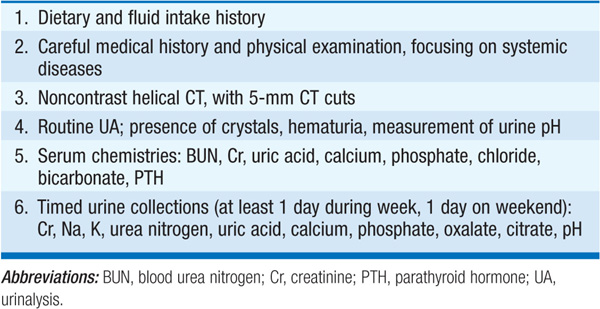
Although some have advocated a complete workup after a first stone episode, others would defer that evaluation until there has been evidence of recurrence or if there is no obvious cause (e.g., low fluid intake during the summer months with obvious dehydration). Table 156-1 outlines a reasonable workup for an outpatient with an uncomplicated kidney stone. On occasion, a stone is recovered and can be analyzed for content, yielding important clues to pathogenesis and management. For example, a predominance of Ca phosphate suggests underlying distal RTA or hyperparathyroidism.
TABLE 156-1 WORKUP FOR AN OUTPATIENT WITH A RENAL STONE
TREATMENT Nephrolithiasis
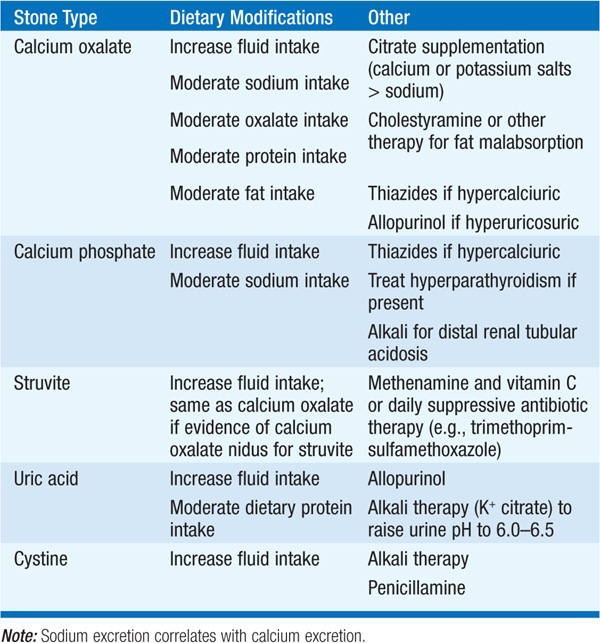
Treatment of renal calculi is often empirical, based on odds (Ca oxalate stones most common), clinical history, and/or the metabolic workup. An increase in fluid intake to at least 2.5–3 L/d is perhaps the single most effective intervention, regardless of the type of stone. Conservative recommendations for pts with Ca oxalate stones (i.e., low-salt, low-fat, moderate-protein diet) are thought to be healthful in general and therefore advisable in pts whose condition is otherwise uncomplicated. In contrast to prior assumptions, dietary calcium intake does not contribute to stone risk; rather, dietary calcium may help to reduce oxalate absorption and reduce stone risk. Table 156-2 outlines stone-specific therapies for pts with complex or recurrent nephrolithiasis.
TABLE 156-2 SPECIFIC THERAPIES FOR NEPHROLITHIASIS