CHAPTER 177
Sarcoidosis
DEFINITION
An inflammatory multisystem disease characterized by the presence of noncaseating granulomas of unknown etiology.
PATHOPHYSIOLOGY
The cause of sarcoid is unknown, and current evidence suggests that the triggering of an inflammatory response by an unidentified antigen in a genetically susceptible host is involved. The granuloma is the pathologic hallmark of sarcoidosis. The initial inflammatory response is an influx of CD4+ (helper) T cells and an accumulation of activated monocytes. This leads to an increased release of cytokines and the formation of a granuloma. The granuloma may resolve or lead to chronic disease, including fibrosis.
CLINICAL MANIFESTATIONS
In 10–20% of cases, sarcoidosis may first be detected as asymptomatic hilar adenopathy. Sarcoid manifests clinically in organs where it affects function or where it is readily observed. Löfgren’s syndrome consists of hilar adenopathy, erythema nodosum, acute arthritis presenting in one or both ankles spreading to involve other joints, and uveitis.
Disease manifestations of sarcoid include:
• Lung—most commonly involved organ; >90% of pts with sarcoidosis will have abnormal CXR sometime during course. Features include hilar adenopathy, alveolitis, interstitial pneumonitis; airways may be involved and cause obstruction to airflow; pleural disease and hemoptysis are uncommon.
• Lymph nodes—intrathoracic nodes enlarged in 75–90% of pts. Extrathoracic lymph nodes affected in 15%.
• Skin—25% will have skin involvement; lesions include erythema nodosum, plaques, maculopapular eruptions, subcutaneous nodules, and lupus pernio (indurated blue-purple shiny lesions on face, fingers, and knees).
• Eye—uveitis in 30%; may progress to blindness.
• Upper respiratory tract—nasal mucosa involved in up to 20%, larynx 5%.
• Bone marrow and spleen—mild anemia and thrombocytopenia may occur.
• Liver—involved on biopsy in 60–90%; rarely important clinically.
• Kidney—parenchymal disease <5%, nephrolithiasis secondary to abnormalities of calcium metabolism.
• Nervous system—occurs in 5–10%; cranial/peripheral neuropathy, chronic meningitis, pituitary involvement, space-occupying lesions, seizures.
• Heart—disturbances of rhythm and/or contractility, pericarditis.
• Musculoskeletal—bone lesions involving cortical bone seen in 3–13%, consisting of cysts in areas of expanded bone or lattice-like changes; dactylitis; joint involvement occurs in 25–50% with chronic mono- or oligoarthritis of knee, ankle, proximal interphalangeal joints.
• Constitutional symptoms—fever, weight loss, anorexia, fatigue.
• Other organ systems—endocrine/reproductive, exocrine glands, GI.
EVALUATION
• Hx and physical exam to rule out exposures and other causes of interstitial lung disease.
• CBC, Ca2+, LFTs, ACE, PPD, and control skin tests.
• CXR and/or chest CT, ECG, PFTs.
• Biopsy of lung or other affected organ.
• Bronchoalveolar lavage and gallium scan of lungs may help decide when treatment is indicated and may help to follow therapy; however, these are not uniformly accepted.
DIAGNOSIS
Made on basis of clinical, radiographic, and histologic findings. Biopsy of lung or other affected organs is mandatory to establish diagnosis before starting therapy. Transbronchial lung biopsy usually adequate to make the diagnosis. No blood findings are diagnostic. Differential diagnosis includes neoplasms, infections including HIV, other granulomatous processes.
As sarcoidosis may remit spontaneously, treatment is based largely on the level of symptoms and extent of organ involvement (Figs. 177-1 and 177-2). When systemic therapy is indicated, glucocorticoids are the mainstay of therapy. Other immunomodulatory agents have been used in refractory or severe cases or when prednisone cannot be tapered.
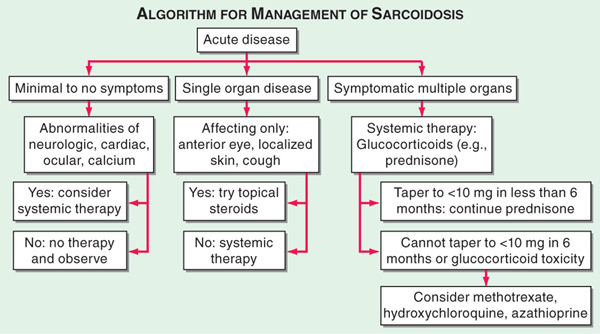
FIGURE 177-1 The management of acute sarcoidosis is based on level of symptoms and extent of organ involvement. In pts with mild symptoms, no therapy may be needed unless specified manifestations are noted.

FIGURE 177-2 Approach to chronic disease is based on whether glucocorticoid therapy is tolerated.
OUTCOME
Sarcoidosis is usually a self-limited, non-life-threatening disease. Overall, 50% of pts with sarcoidosis have some permanent organ dysfunction; death directly due to disease occurs in 5% of cases usually related to lung, cardiac, neurologic, or liver involvement. Respiratory tract abnormalities cause most of the morbidity and mortality related to sarcoid.

For a more detailed discussion, see Baughman RP, Lower EE: Sarcoidosis, Chap. 329, p. 2805, in HPIM-18.