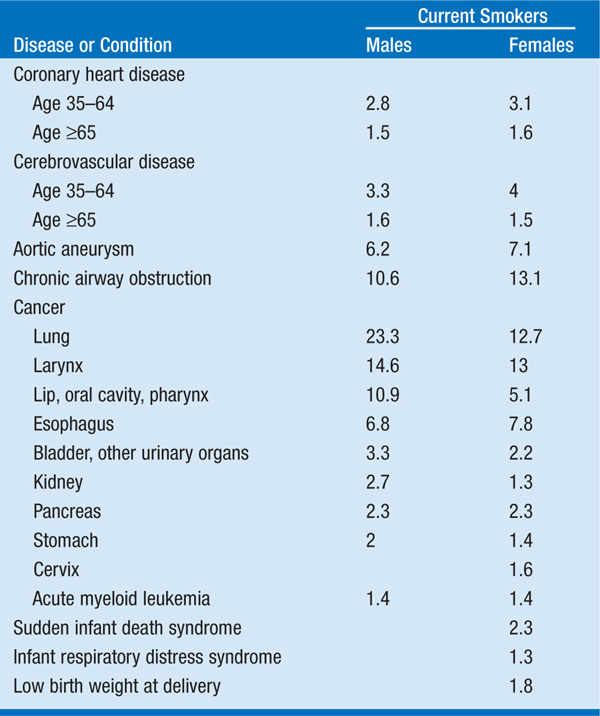
Over 400,000 individuals die each year in the United States from cigarette use: one out of every five deaths nationwide. Approximately 40% of smokers will die prematurely unless they are able to quit; major diseases caused by cigarette smoking are listed in Table 217-1.
TABLE 217-1 RELATIVE RISKS FOR CURRENT SMOKERS OF CIGARETTES
APPROACH TO THE PATIENT Nicotine Addiction
All pts should be asked whether they smoke, their past experience with quitting, and whether they are currently interested in quitting; those who are not interested should be encouraged and motivated to quit. Provide a clear, strong, and personalized physician message that smoking is an important health concern. A quit date should be negotiated within a few weeks of the visit, and a follow-up contact by office staff around the time of the quit date should be provided. Incorporation of cessation assistance into a practice requires a change of the care delivery infrastructure. Simple changes include:
• Adding questions about smoking and interest in cessation on pt-intake questionnaires
• Asking pts whether they smoke as part of the initial vital sign measurements made by office staff
• Listing smoking as a problem in the medical record
• Automating follow-up contact with the pt on the quit date
TREATMENT Nicotine Addiction
• Clinical practice guidelines suggest a variety of pharmacologic and nonpharmacologic interventions to aid in smoking cessation (Table 217-2).
TABLE 217-2 CLINICAL PRACTICE GUIDELINES
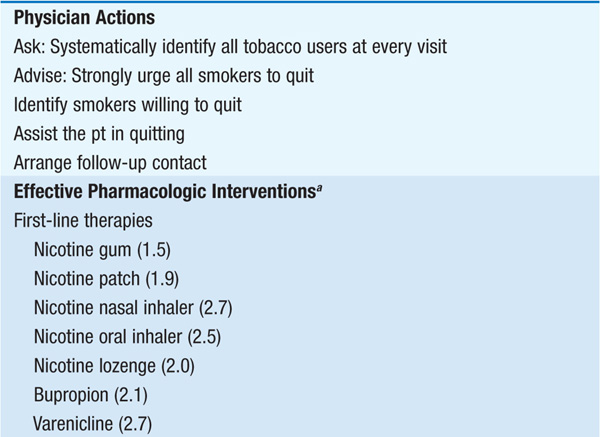
• Numerous nicotine-replacement products exist, including over-the-counter nicotine patches, gum, and lozenges, as well as nicotine nasal and oral inhalers available by prescription; these products can be used for 3–6 months with a gradual step-down in dosage with increasing duration of abstinence.
• Prescription medications that have been shown to be effective include antidepressants such as bupropion (300 mg/d in divided doses for up to 6 months) and varenicline, a partial agonist for the nicotinic acetylcholine receptor (initial dose 0.5 mg daily increasing to 1 mg twice daily at day 8; treatment duration up to 6 months). Antidepressants are more effective in pts with a history of depressive symptoms.
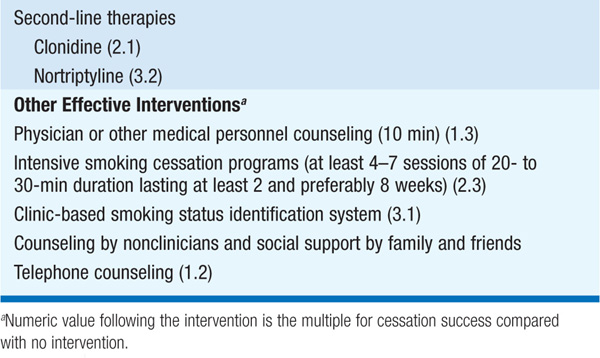
• Clonidine or nortriptyline may be useful for pts who have failed first-line therapies.
• Current recommendations are to offer pharmacologic treatment, usually with nicotine replacement therapy or varenicline, to all who will accept it and to provide counseling and other support as a part of the cessation attempt.
Approximately 90% of individuals who will become cigarette smokers initiate the behavior during adolescence; prevention must begin early, preferably in the elementary school years. Physicians who treat adolescents should be sensitive to the prevalence of this problem and screen for tobacco use, reinforcing the fact that most adolescents and adults do not smoke, and explaining that all forms of tobacco are both addictive and harmful.
