‘He who fears he shall suffer, already
suffers what he fears.’
– Montaigne
Any one of us can succumb to illness and pain at any time. We then have a choice: we can take a passive role, allowing the doctor to take authority, or we can decide to be actively and knowledgeably involved in our own care – which implies taking a more holistic approach: i.e. why have I developed this pain? How is it going to affect my life? How do I feel about it? It is enormously empowering to realise that one is not a passenger but a co-driver on the route to health. And to do this we need to get to grips with the link between psychology, emotion and physiology because understanding this gives us a vital tool for the process of our recovery.
As Dr Gabor Maté says, it is important to understand that how you feel is the summation of all your bodily processes: ‘Physiologically, emotions are themselves electrical, chemical and hormonal discharges of the human nervous system. Emotions influence – and are influenced by – the functioning of our major organs, the integrity of our immune defences and the workings of many circulating biological substances that help govern the body’s physical states.’ 33
In this chapter, I hope to convince you or at least tweak your curiosity enough to make you consider deeply some fascinating truths around human behaviour: namely, how we respond to stress and how it makes us ill. This is a chapter about ‘mind over disease’ and the connections between the brain and immune system which mediate our health. I will show you that our mental and physical states are inextricably linked, and that stress and other psychological factors not only cause pain but also often alter our vulnerability to bacterial and viral infections as well as cancer, heart disease and diabetes.
In the words of the celebrated neuroscientist and pharmacologist, Professor Candace Pert: ‘It is this problem of unhealed feeling, the accumulation of bruised and broken emotions that most people stagger under without ever saying a word, that the mainstream medical model is least effective in dealing with.’ 34
Most importantly, I want you to consider that what is going on with your health, physical or mental, may be down to something, or things, you have not yet thought about. You may need to address other possible contributing elements, not just the obvious symptoms. Accepting the possibility that life and all that it throws at you is as much a cause of your pain as an injury or condition is the first step to sorting it out.
Dr Hans Kraus was the New York physician who famously treated and cured US President John F Kennedy’s spinal pain after years of failed attempts by other doctors. Kraus discovered that, though young and lean in physique, JFK was muscularly as weak as a kitten and as stiff as a board, and so he devised an intense programme of flexibility and strengthening exercises for him.
Having completed this regime, JFK was almost pain-free, and even able to play golf again. Kraus had identified a condition he termed ‘muscle tension syndrome’, which he said existed predominantly in people who were exposed to significant and constant levels of stress.
In his book Backache, Stress and Tension, Kraus explained where this tension came from: ‘Your muscles, your mind, your heart and all your organs prepare to act, but you do nothing… You may wish to fight, you may wish to flee, but modern civilisation prevents you from carrying out your natural impulses… You race your engines without going anywhere.’ 35
I have noticed in my own practice that the paradoxical relationship between inactivity (particularly in those in corporate sedentary jobs) and mental stress embodies this idea exactly. The stress response wants us to act but – stuck to our seats – we constantly repress what we feel, or rather what society feels, would be an inappropriate response physically.
My mentor, Dr John Sarno, whom I mentioned in the previous chapter, embraced the Kraus approach and developed the idea still further. He found that, although many patients responded to an exercise programme, this did not resolve all their issues. And he noticed that, although their pain might improve initially, the symptoms would often return or simply move and manifest themselves somewhere else in the body. He quickly saw a pattern develop in many of his patients, that their pain was a manifestation of repressed emotional turmoil and that this resulted in oxygen deprivation and a build-up of waste products from metabolism, which was responsible for the muscle tension and neurological irritation.
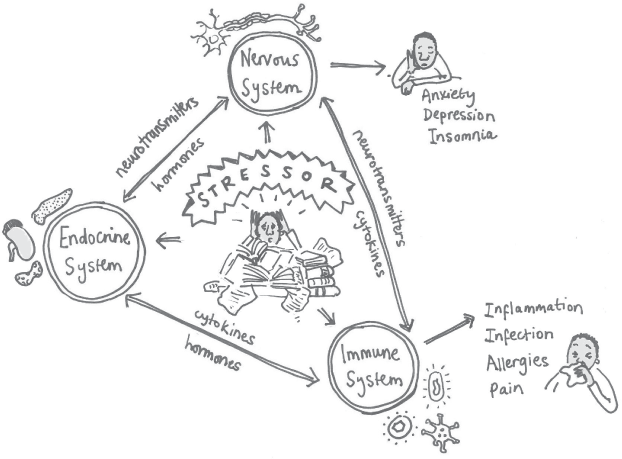
This realm of interconnectedness between the psychological processes, the hormonal glands and the immune systems that regulate our behaviour and physiological balance is the subject of a fascinating area of study known as psycho-neuroendocrine-immunology, or PNI.
You will remember, from earlier chapters, the idea of nociception: that is, the sensory input from the body which is sent to the brain for assessment and analysis (bottom-up)? And you will remember that pain only occurs when the brain decides to recognise the information it receives from nociception (top-down)? Well, PNI is the system that the brain mobilises to carry out a response to all of the stuff it has analysed and decided needs action. The psycho- bit represents the cognitive element through which we decide what to do; the neuroendocrine- is the linked system of nerves and hormones which communicate a call to action and the specific response in different tissues and organs. The -immunology bit refers to the myriad responses in the immune system to set off inflammation if there is a need to heal, as well as the specialist cells needed to fight any infection which gets into the body as a result.
There is now consistent and growing evidence from thousands of scientific studies for a connection between life events, personality type, stress and the psychological causes of subsequent pain, disease and even malignancy.36 These life events don’t need to be extreme or traumatic; the cumulative effect of life’s mundane trials and tribulations can also have an impact on health over time. The diseases of multiple sclerosis and rheumatoid arthritis are good examples of conditions where stressful childhood parental relationships, life adversity or traumatic events either just before the onset of the disease or as a causative agent in its symptom exacerbation have been strongly linked. The common process involved in these conditions is inappropriate persistent inflammation in tissues causing long-term damage.
As early as 1939, John Scott Haldane, a British physiologist, had a hunch about the involvement of psychological factors in disease and wrote: ‘The commonest cause of gastritis, an inflamed and irritable stomach, is worry and anxiety. I had it for 15 years and then I read Lenin on Society and how to cure it. Since then I am cured.’ 37
Food for thought! (Though reading Lenin is not something I regularly prescribe for my patients.)
PNI is essentially a bodily communication system in which all the components – our thoughts, emotions, immune system and hormones – are linked by a network of two-way pathways, with one agenda: to ensure our survival and reproduction and the propagation of our genes. These connections allow the system to recognise both internal and external threats and respond with appropriate behaviour and biochemical reactions to maximise safety at as little cost as possible. This ‘super-system’ is hardwired together by the nervous system. Even the glandular and immune centres (e.g. bone marrow, thyroid and thymus glands), which were once thought to be acted on only by hormones, are extensively supplied by nerves. Within the nervous system there are many different types of neurones which serve different functions. Some simply connect other nerves, some feed, nourish and repair them, and some monitor the need for change and action it locally if necessary. But they all serve to facilitate the communication between all of the four systems of the PNI, whether it is to increase or decrease a response or just feed back to the brain on the current state of things as to how much to respond (See figure 4 overleaf).
So, the amazing news is that the brain can talk to and monitor every system in the body… and, likewise, each of the hormones and immune cells can exert their own influence on the brain. The chemicals produced by all these systems attach to receptors on brain cells, thereby directly affecting our behaviour.
Almost all cells, by the way, have receptors on their surfaces for molecules coming from the brain – this is how the brain communicates directly with the immune system and this is why any short- or long-term stimulus which acts on any part of the PNI system is felt by every other part to some degree. The stressor exerts an effect on us which causes a shift or response in the entire system. The chatter is passed down the line to every cell, regardless of its primary function. Think of the cells as being like people on a crowded tube train, everyone jostling and adjusting as one more passenger gets on. A good example of this is the white blood cells, which are the main defenders of the immune system against invaders or disease and can produce almost all the same hormones and neurotransmitters that the brain cells can. They can even produce the mood-altering and pain-relieving chemicals known as endorphins – our own happy pills. On the downside these white blood cells can produce their own chemicals (cytokines) which in the brain exert their effect as pain and depression, and in the joints as pain and swelling. The effects can be felt anywhere in the body – not just at the site of the infection.
So, we can see that there is a big ‘conversation’ going on throughout the body via a super-system of messengers using what could almost be described as a ‘molecular language’.
We have all experienced the sensation of being exposed to a brief episode of stress such as a near-miss with another car. We get the ‘prickly armpit’ sensation, rapid pulse and sweaty palms that are due to a hormone we are all familiar with: adrenaline. This is produced in the adrenal glands, located just above the kidneys.
All the cognitive and emotional centres within the brain that detect danger and threat communicate with the rest of the body through one hub called the hypothalamus, a region deep in the brain, just above the pituitary gland. And when we perceive immediate danger or fear, signals are sent via the hypothalamus, using adrenaline.
Figure 4: The PNI system, which connects our emotions, thoughts, hormones and immune system.
Adrenaline acts on a part of the nervous system called the autonomic nervous system, which has two distinct parts: the sympathetic system, which governs our immediate ‘fight or flight’ response; and the parasympathetic system, which governs our ‘rest and digest’ functions. In an ideal world, most of the time we should be in the zen-like parasympathetic domain: relaxed, ruminating, digesting, making love and going about our daily activities, and only nudging into the sympathetic zone occasionally when roused.
However, due to the stresses of our modern lives now, and any that we may have experienced in our formative childhood years, we tend to shift into the sympathetic domain. Here we sit in a constant state of readiness to fight or to run. This is OK for the short term but if it goes on too long, messages get sent to the hypothalamus, which in turn activates another part of the adrenal glands to secrete cortisol, the uber-hormone of the stress response. Cortisol has a huge number of effects on the PNI system, through many chemical and electrical messengers. Its immediate effect is to mobilise energy systems to make them available for survival. And it acts on almost every tissue of the body; from the brain to the immune system and from bones to intestines. Despite there being a general increase in immune activity during stress, cortisol’s immediate effect is to dampen the stress reaction, keeping immune activity within safe levels. The stress response can be seen not only as the body’s reaction to threat but also as its attempt to maintain stability and homeostasis. The body is held, if you like, in a state of physiologically controlled panic.
It was Dr Hans Selye who first described how the biology of stress affected three types of tissue or organs: in the hormonal system (enlarged adrenal glands); in the immune system (spleen, thymus and lymph glands); and in the digestive system (intestinal lining). In one of his first studies, rats exposed to stress for long periods showed enlarged adrenals, shrunken lymph nodes and ulcerated intestines.38 This would explain why so many stress sufferers present with stomach and intestinal problems and ulcers.
The most pertinent element of the cortisol response for our purposes, as we think about chronic pain, is its effect on inflammation.
In a study he conducted at Carnegie Mellon University, Professor Sheldon Cohen showed that chronic psychological stress is associated with the body losing its ability to regulate the inflammatory response, because the immune cells in the tissues become insensitive to cortisol.39 (Some practitioners have begun to refer to this state as adrenal fatigue, although that remains a controversial diagnosis.) Cohen’s was a major finding as it solved a conundrum that the medical profession had struggled with for some time: namely, if cortisol inhibited the inflammatory response – indeed, cortisol injections have been used for many years to ease inflamed and painful joints – how could it also stimulate it? Cohen discovered that the acute short-term effects of cortisol are indeed anti-inflammatory but that with prolonged secretion the effect is lost.
He went on to show that the effects of psychological stress on the body’s ability to regulate inflammation can promote the development and progression of diseases such as joint disease and autoimmune conditions such as rheumatoid arthritis, which predominantly manifest in the inflammatory response and the failure to recognise ‘self’ – the so-called ‘friendly fire’ effect. Cohen observed that when cortisol is not able to serve its regulatory function, inflammation can get out of control. Such inflammation can affect a multitude of tissues, most particularly the linings of the joints and the spine, and the stomach and digestive system.
New and exciting research has shown that the chemicals I mentioned earlier, cytokines, which are actively involved in the inflammatory stress response, can also cross what is known as the blood–brain barrier, which was previously thought impossible, as is elegantly described by Dr Edward Bullmore in his book The Inflamed Mind.40 It is now believed that cytokines which get through the specialist cells (endothelial cells) lining the small blood vessels of the brain can trigger inflammation in the brain and that this may be the source of many forms of depression and possibly even dementia. This finding has raised many new questions, for example whether people suffering with painful arthritis are depressed simply because of the pain or whether in fact depression is part of the inflammatory process affecting the sensitive neural tissues.
The details are still uncertain but people who are depressed show an array of immunological changes, even without other illness being present. Equally, people who have a lot of inflammation in their bodies, such as rheumatoid arthritis, frequently report depression as well as higher levels of pain.
Cohen, in his research, also showed that people who were exposed to a prolonged stressful event and who were therefore unable to control the inflammatory response were much more likely to succumb to a cold virus. He demonstrated that stress has an impact on heart disease and asthma, because these conditions are also inflammation-based.
In 2013, a joint study carried out by several US universities, led by UCLA and Ohio State, found that individuals who had chronic exposure to adverse environments (bereavement, social isolation and low socio-economic status) showed increased inflammation in their bodies41 – that their sympathetic nervous system stimulated their bone marrow to produce immature pro-inflammatory cells and that this inflammation was capable of causing pain at multiple sites. Furthermore, it was shown to inhibit the production of genes designed to mount an immune response to viruses. Hence many sufferers of cold sores (which are caused by a herpes simplex virus) report that they develop a sore only when they are stressed or run down. The dip in the immune system function allows the virus to activate itself. Shingles, another herpes virus, follows a similar pattern. These viruses which live within us permanently, are suppressed by a healthy immune system until we are stressed either by our environment or by another infection, ‘distracting’ the immune system from it.
Obesity is another cause of stress on our systems that results in inflammation. We now know that people who are significantly overweight and who as a result produce adipose tissue (a form of body fat) have increased levels of inflammation in their bodies. Researchers have shown that an overload of fat in our bodies damages the mitochondria, the ‘power generators’ in our cells, which are responsible for providing energy for metabolism.42 The body then mounts an immune response to repair or break down the damaged mitochondria. And this leads to inflammation in the tissues, which causes joint pain and arthritis, and inflammation of the blood vessel walls, which results in atherosclerosis, a cause of stroke and heart disease.
If that weren’t enough to convince you of the dangers of stress, there is also now evidence that a vicious cycle can develop between obesity and cortisol. Cortisol is known to increase the absorption of fat when we are stressed and classically redistributes it around and inside the abdomen. When going through stressful periods, even slim people who do not overeat can discover that they have fat around their middles which they cannot shift. This is the most serious type of weight gain as it is the most detrimental to health. It is why the medical profession has started using the hip-to-waist ratio (which involves dividing the circumference of your waist by that of your hips) rather than Body Mass Index to measure obesity.
So we can see how, paradoxically, a biochemical system designed to preserve life becomes a major cause of pain and illness. In the short term, this mechanism is extremely effective in the emergencies it was designed to protect us from. But if triggered for prolonged periods and without remission, it produces permanent damage and long-lasting pain. Chronically stimulated, adrenaline raises blood pressure and damages the heart, while cortisol impairs the immune system and damages tissue.
The awkward truth here is that science is now proving that the ‘H’ word, holism (treating the whole person, taking into account medical and social factors, rather than just the symptoms of disease) is the way forward. Holistic medicine has become associated with quackery, snake oil and wooden beads, but in many ways it resembles how the old-school avuncular physicians approached the patient’s story. With fewer diagnostic tests at their disposal, country GPs (think of the TV series Dr Finlay’s Casebook if you are old enough) viewed patients within the context of their environment and used as much life wisdom to treat them as medical knowledge. They honed their bedside manner with the use of time-honoured clinical skills which reassured their patients.
With a move towards a symptom-based reductionist philosophy of tests and imaging, driven by the infiltration of profit-obsessed pharmaceutical and biotech companies into hospitals, medical schools and universities, the old-style holistic principles have long been sidelined and are now applied only by alternative healing practitioners.
Gratifyingly, and in my own practice lifetime, we are beginning to see a swing back towards a more 360-degree view of illness and disease – though using new terms such as ‘functional’ or ‘integrated’ medicine, rather than the ‘H’ word. And this, I hope, is going to change the whole approach to the treatment of pain.
Twenty-year-old Max came to see me with his mother. His family is well-off and have lived all over the world. Max had been to the best schools, and he emphasised the fact that he was now doing a psychology degree, as if to warn me off indulging in any psychobabble. At several stages he had been at boarding school and thus living apart from his parents, who are now separated. The tension between Max and his mother was palpable, and he barely looked at either her or me as he related his tale. He had a constant air of angry petulance and sighed or held his breath every few seconds. He referred to his mother for details he clearly knew himself and was on edge constantly. It was obvious that he was treated as the ‘sickly child that needed to be fixed’. He sweated nervously and had clammy palms when we shook hands. He was tall and very lean, and from the way he sat, folded his arms and fidgeted, I could see he was hypermobile (double-jointed). He smelt strongly of tobacco and the scent of marijuana emanated from every pore. He had rowed competitively at school and university.
Max had a set of musculoskeletal symptoms that he couldn’t cope with any more. He had head, neck and back pain and he always felt twisted physically. Indeed, one practitioner had told him that his symptoms were all down to scoliosis, being born with a twisted spine. Additionally, he was light-headed and struggled to sleep and concentrate. He frequently had palpitations.
Max had seen a multitude of practitioners, both conventional and alternative, but none had managed to get to the bottom of his issues and his parents had spent a fortune on tests and imaging.
He was understandably sceptical as to whether I would be able to help him. His mother wanted to stay in the room even for his examination. Max did not actually protest but it was clear he would rather she was not there, particularly as I asked him to undress so I could examine him. It was almost as if he knew it was inappropriate that she should stay but he wanted her to be there all the same.
When I examined his back, I saw he had a marginal ‘S’ bend curve in his spine, of only a few degrees. On my computer, I showed Max a picture of another patient’s anonymised X-ray, which had a dramatic scoliosis of 52 degrees. He drew in his breath and said, ‘Will I end up like that? She must be in agony!’ I explained that she wasn’t actually, and never had been, despite how impressively twisted she was. This went some way to reassuring him, but I also asked him: ‘If she isn’t in pain, how come you are, with such a small curve?’
He thought about this for a moment and raised his eyebrows quizzically. I told him that, despite all the things reported on MRI and X-ray, his curve had almost nothing to do with the pain he complained of. I explained that a lot of the asymmetrical muscle tension on the left-hand side of his low back was in fact due to years of rowing with one oar on the same side. Over the period of ten years that he had been competing, he had developed a shortened pattern in the muscles on one side because it had never been addressed. This was further reflected in the very small muscles at the base of his skull, on the opposite side, where he had been compensating through his neck to keep his eyes on horizontal. All of this was exacerbated by the deep intrinsic muscle tension that he constantly experienced, primarily due to his ‘Type A’ perfectionist and controlling character, and his all-round ‘high-performance’ upbringing. Max had no control over his current state and that bothered him too. He had never been allowed to relax or really enjoy life, because it was always about competing either academically or in the sporting arena or even within his own family, where success was expected and praised.
During the little time he spent with his parents, he would always seek their approval and affirmation by impressing them. Throughout his schooling he had always been a survivor and had seemed very resilient but he was not able to express himself emotionally, nor did he really know how he felt. All he knew was that he had to be in a constant state of readiness.
I explained to Max that he was hypermobile in many of his joints and soft tissues and this meant that his muscles had to work harder to fight against gravity and maintain his posture. This would make his muscles ache and cause him pain.
He was surprised when I asked, ‘Do you find that you need to move to think? That sitting still is always a problem for you and that you fidget in cinemas and tap your foot?’
His eyes almost welled up in relief that someone finally understood him. His gaze, which had previously flitted around the room, now fixed me intently. I went on to explain to him that it was clear from the way he fired his core muscles that he had not learned to crawl properly as a child – a major motor coordination developmental milestone.
Indeed, his mother confirmed that he’d gone straight to walking but had needed a lot of help. I suspected that although he had no problems with coordination in real terms, he had always been slightly clumsy and always lacked the speed, strength and agility that many of his friends had. That is why he had taken up rowing: as a sport, it does not require multi-skilled tasks. The pressure – and his ultimate failure – to be in the other ‘A’ sports teams had pushed him towards it.
The first thing to do with Max was to try to teach him to cope with his stress regarding his performance and show him that when he relaxed his muscles, he not only felt less twisted but also in less pain, and that his mind would calm and he would sleep better. I asked him to stop smoking marijuana as it is a drug of withdrawal and as such was preventing him from engaging in what he needed to do to get better. We could teach him to switch off by other means. I also asked him to avoid caffeine and nicotine for three months as we tried to calm his nervous system down.
I gave him my Bakpro tools – a specialist kit for pain relief I have developed43 – to help him release the painful trigger points that had developed in his muscles at multiple sites. This would not only help him reduce and eventually eliminate his pain but also teach him that he had better control over his condition than he thought. Over the next few sessions, I asked his mother not to come with him; this removed the gag on him talking about his family life and the pressure involved. I manipulated and mobilised all his spinal restrictions, which quickly got rid of his headaches, and taught him exercises to release the asymmetry in his muscles.
At our subsequent appointments, Max no longer had clammy hands and he did not sweat so profusely. He was palpably calmer, and his posture was relaxed. The colour had returned to his face due to the improved oxygenation of his tissues now that he did not hyperventilate. For the first time in some years, he discovered the benefits and delights of a good night’s sleep and was more able to concentrate on his work. He had found it surprisingly easy to give up smoking dope now that life was better.
Perhaps most gratifyingly, Max now had a delightful girlfriend whom he brought to meet me one day. She said she had always liked Max in class, but he was always so ‘wired’ and intense. He always moaned about his health. She noticed that one day something seemed to change in him, and she liked it. So she said yes when he asked her out.