Normal sinus rhythm is a regular rhythm. What we mean by this is that the complexes occur at a regular and consistent distance from each other. To use an analogy, think of how light posts are placed along the sides of the road. They are all placed at regular, recurring distances from each other along the roadside.
Why does this regularity occur? To understand why, we need to go back to the concept of automaticity and phase 4 that we talked about in Chapter 2, Electrophysiology. Remember, phase 4 is a very slow but continuous depolarization of the pacemaker cell from its most negative repolarization value until the threshold potential was reached and the cell fired. This slow, gradual phase 4 is how the pacemaking function of the cardiac cells is created. The length of the phase 4 cycle is very consistent and determines the pacemaking rate of the particular cell type involved.
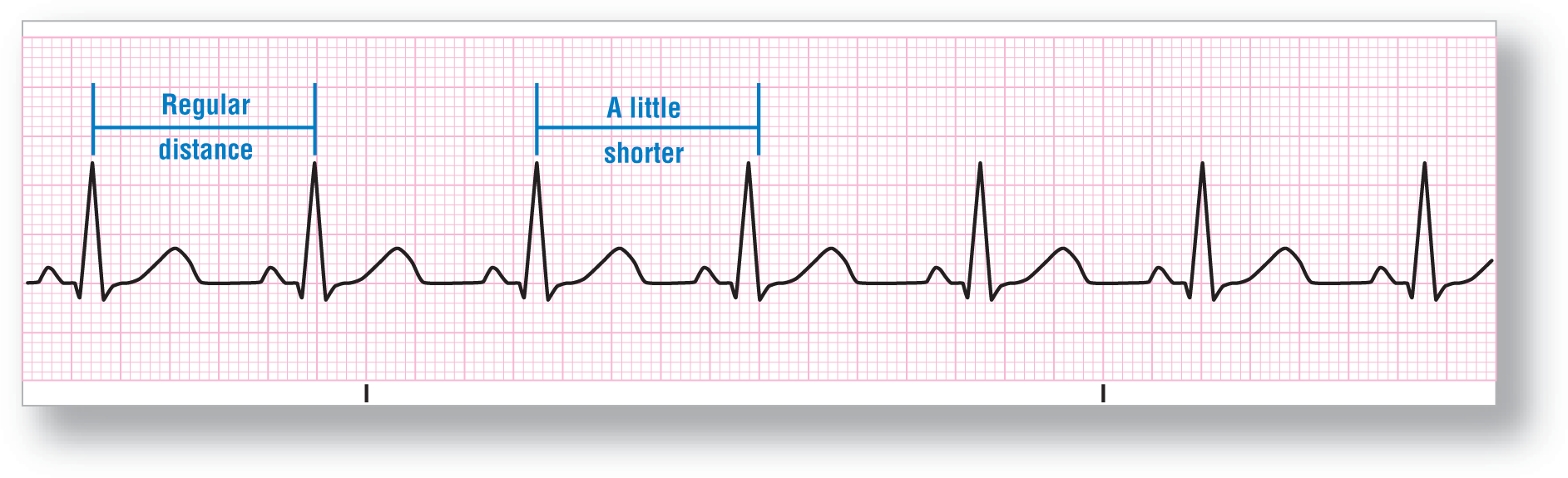
Under normal circumstances, the SA node has the fastest phase 4 of any of the cardiac cells and functions as the main pacemaker for the heart. By definition, NSR has the SA node as the main pacemaker to set the cardiac rate. This rate is very regular in most cases. Occasionally, slight variations in timing can occur. Variations of up to 0.16 seconds can occur occasionally and still be considered normal (Figure 8-9). In these cases, it is critical to remember that the P wave should have the same morphology as the sinus P wave and that the PR interval should be consistent with the regular complexes.
Figure 8-9 Notice the slight irregularity of the fourth complex. It is slightly early but has the same P-wave morphology and PR intervals as the other beats. This is NSR.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
On a rhythm strip or ECG, the distance is measured from one spot on a complex to the same corresponding spot on the next complex. This distance is then transferred to the remaining beats. If the distance is the same, or close to it, we say that the rhythm is regular.
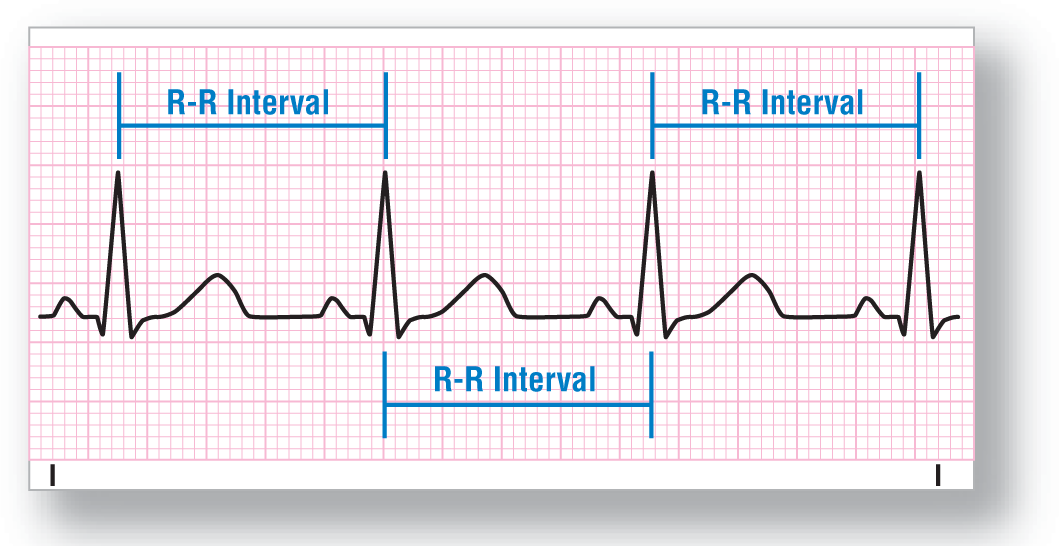
By tradition, the most common distance measured is called the R-R interval (R to R interval [Figure 8-10]). This is the distance from the top of one QRS complex to the top of the next beat. The top of the QRS is used because it is usually very easily identifiable and easy to pinpoint with your calipers.
Figure 8-10 The R-R interval is the most common distance measured because it is easy to identify the top of the QRS complex.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
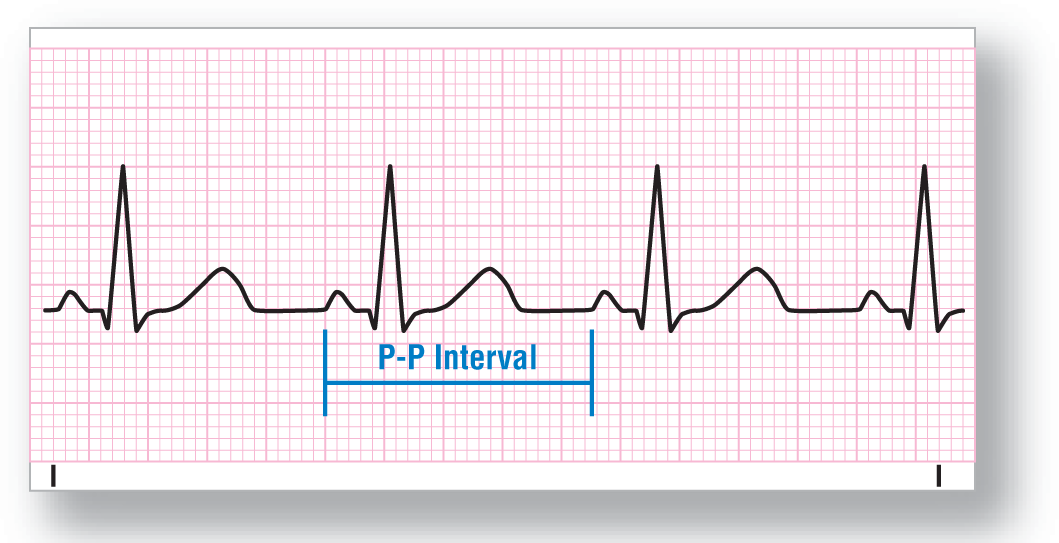
Another measurement that is constantly used is the P-P interval (Figure 8-11). You would calculate the distance the same way as the R-R interval, but you would use the top or the beginning of the P wave instead of the top of the R wave.
Figure 8-11 The P-P interval can also be used for measuring distance.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
By definition, rhythms have to be either regular, regularly irregular, or irregularly irregular. We discussed the issues with regularity earlier. Now, let’s turn our attention to the issues with irregularity.
Regularly Irregular Rhythms
To discuss irregularity, we need to understand the difference between a rhythm and a rhythm with an overlying cardiac event that momentarily alters the cadence of the underlying rhythm. Suppose you had a strip with an NSR clearly visible on it; for simplicity, we represented each complex with a gold bar in Figure 8-12. Suddenly another pacemaker in the heart became irritable and fired early. The morphology of either the P wave or the QRS complex generated by the secondary pacemaker would be different and early compared with the rest of the complexes around it. Let’s use a blue circle in Figure 8-12 to represent this cardiac event. Would this new rhythm have a new name? The answer is no. What we say is that the patient has a normal sinus rhythm with a ________ (the blank will be filled in by the name of the event). For example, we would say that the patient had a normal sinus rhythm with a PVC.
Figure 8-12 An example of normal sinus rhythm interrupted by an event, after which normal sinus rhythm continues. Each gold vertical bar represents a complex.
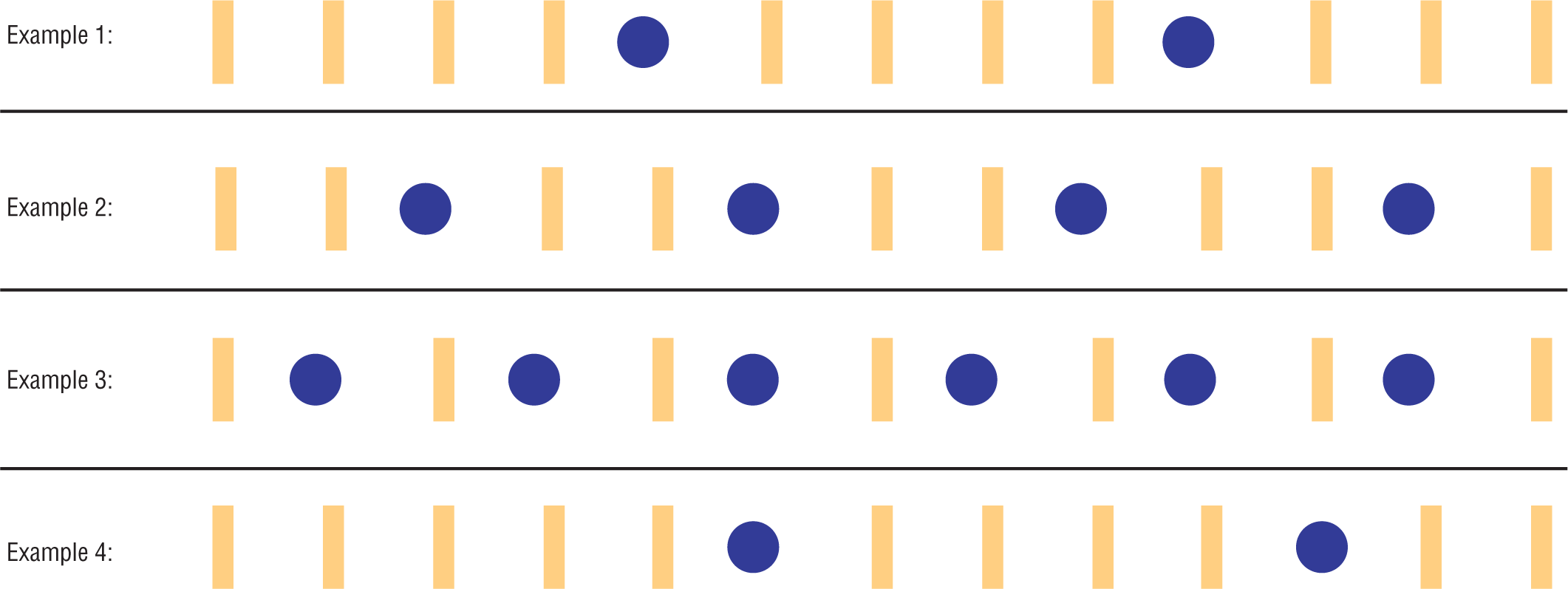
This is an example of a regularly irregular rhythm. Let’s break down this term a bit further in order to understand it more clearly. The first word “regularly” signifies that the underlying rhythm is regular. It could be any of the regular rhythms that we will discuss in this book, but it has to be a regular rhythm. The second word denotes the abnormal events that occur between or inside of the regular rhythm. That irregularity may occur once, twice, or be a recurring event at various intervals during the strip (Figure 8-13).
Figure 8-13 Examples of regularly irregular rhythms in which the event does not alter the underlying cadence of the regular rhythm.
In some cases, the cardiac event may alter the rate of the original regular rhythm but the subsequent rhythm could still be regular. Look at Figure 8-14. At the start of the strip, we have a nice, slow, regular rhythm. Then a cardiac event occurs. After the event, the underlying rate or pacemaker has changed but the rhythm still remains regular. This is still considered a regularly irregular rhythm and is quite a common occurrence in many patients. We describe this rhythm by breaking down each component and mentioning them separately—for example, a normal sinus rhythm with a PVC followed by a sinus tachycardia.
Figure 8-14 An example of normal sinus rhythm interrupted by an event, followed by sinus tachycardia.
When a rhythm is completely chaotic and you cannot find any underlying regularity, we say that it is irregularly irregular. They are easy to spot because the cadence of the complexes is completely haphazard. In addition, the P waves and PR intervals, if there are any, are almost always variable in morphology.
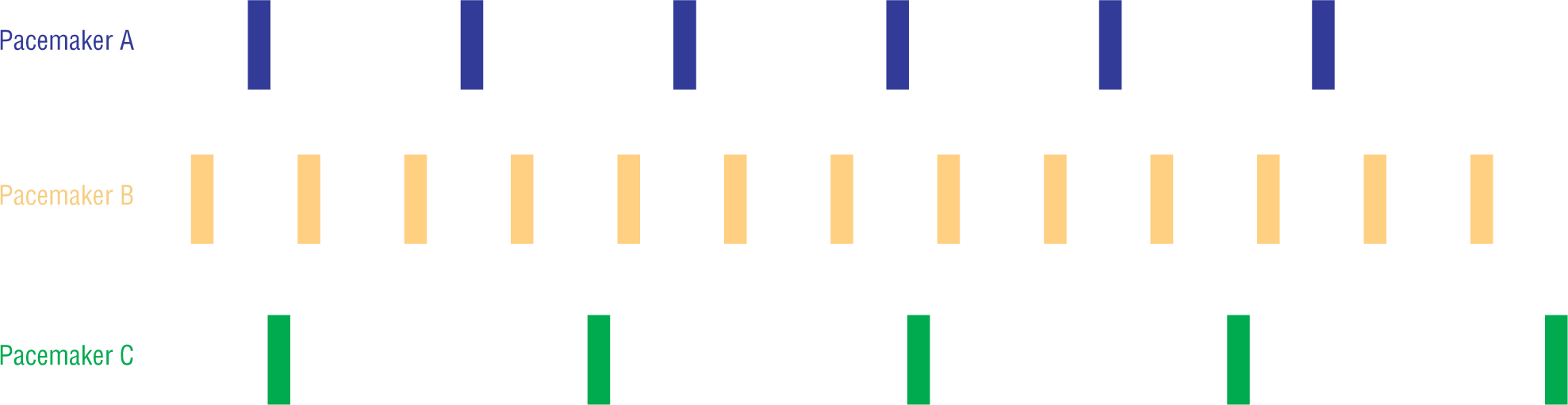
How does a rhythm become totally chaotic? Well, let’s look at a case involving three different atrial pacemakers, each firing at its own intrinsic rate. In Figure 8-15, we have isolated the rhythm strip from the three different pacemakers: A, B, and C. For simplicity, we will use different colored bars to represent the complexes generated by each of the pacemakers.
Figure 8-15 Examples of complexes generated by different pacemakers.
Not a big deal, right? The rhythm for each of the three pacemakers is clearly delineated and easy to spot. Keep in mind that each one of those stars represents an entire complex, P wave, PR interval, QRS complex, and ST-T waves. Also keep in mind that each one of the P waves and PR intervals may be different. Still not a problem—it is still easy to visualize.
Now, let’s make all three pacemakers fire simultaneously in the same heart and have each one continue to fire at its own intrinsic rate. Can you visualize what the strip would look like?
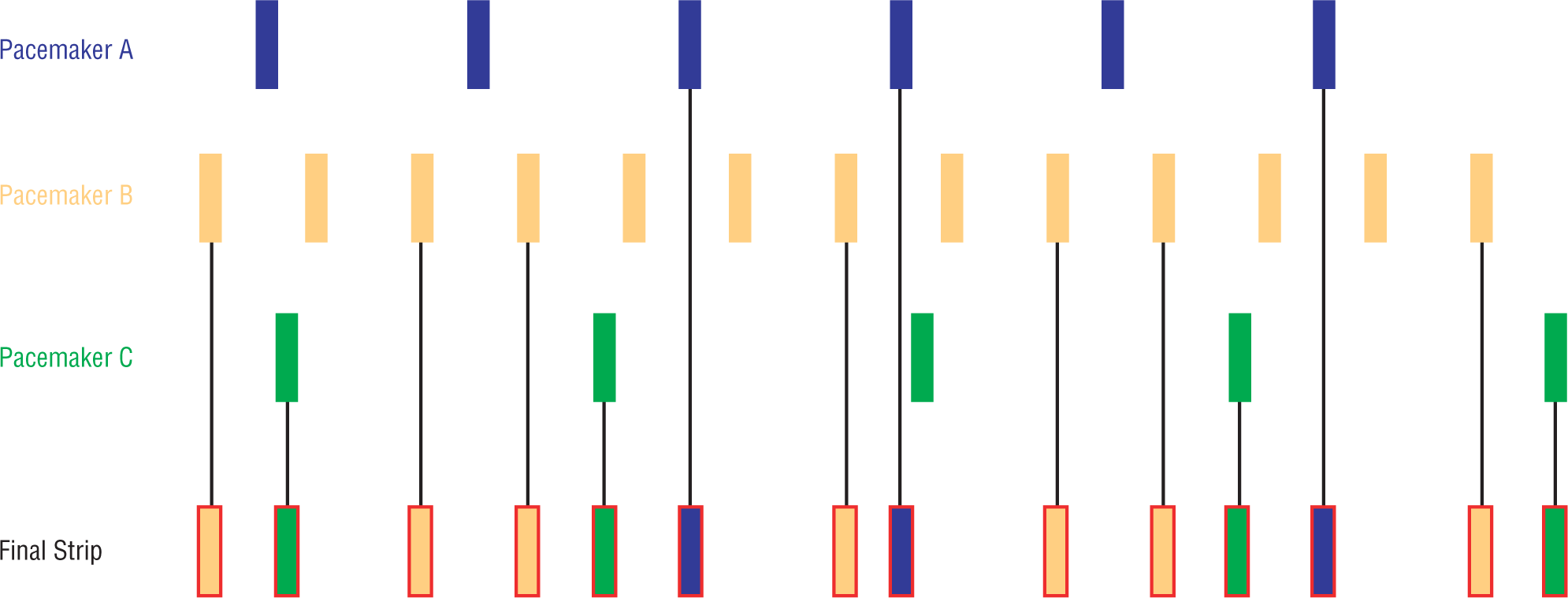
Taking into account that some complexes would not be transmitted because they fall on the absolute refractory period, and the fact that some may not be transmitted for other unclear reasons, we can make a reasonable guess as to what the final strip would look like with these three pacemakers (Figure 8-16). As you can see, the final strip has very few repetitions of any R-R interval. This strip is typical of the chaotic and completely random pattern seen in an irregularly irregular rhythm.
Figure 8-16 An example of a rhythm strip in which three different pacemakers exist.
To make matters a bit more complex, we need to remember that some complexes will fuse to form entirely new complex morphologies and completely different R-R intervals. To continue adding complexity, suppose there were four pacemakers instead of three. What if there were five or six pacemakers? Now, you can begin to imagine the complexity found in irregularly irregular rhythms. Luckily for us, there are only three main irregularly irregular rhythms: wandering atrial pacemaker, multifocal atrial tachycardia, and atrial fibrillation. We will discuss each of these in great detail later on in the book. This is an initial introduction to the topic.
We have taken a serious look at how NSR is formed. We have reviewed the characteristics of NSR and some of the principles that are beautifully outlined by this rhythm, for example, regularity. Now, it is time to begin to actually look at some strips. In this book, we will try to show you various examples of each of the rhythms. We will show you some examples that are at the fast end of the spectrum, some that are at the slow end of the spectrum, some with positive complexes, and some with negative complexes. It is critical for you to apply the concepts we have learned to each strip. The concepts are what you will need to remember.
Additional Information
Nomenclature
A little problem with nomenclature . . .
Many authors state that in NSR the width of the QRS complex must be less than 0.12 seconds wide. They use the term regular sinus rhythm rather than normal sinus rhythm to describe rhythms with wide QRS complexes, but the methodology is not always spelled out. The majority of clinicians and authors use the terms interchangeably.
This text sticks with the strictest criteria and states that the QRS has to be normal width in order for the rhythm to be normal sinus rhythm. We will use the term sinus rhythm or regular sinus rhythm to describe strips with abnormally wide QRS complexes. Clinically, the important point to try to resolve is why the QRS complexes are wide in the first place.
Additional Information
Slight Variations in P Waves and PR Intervals
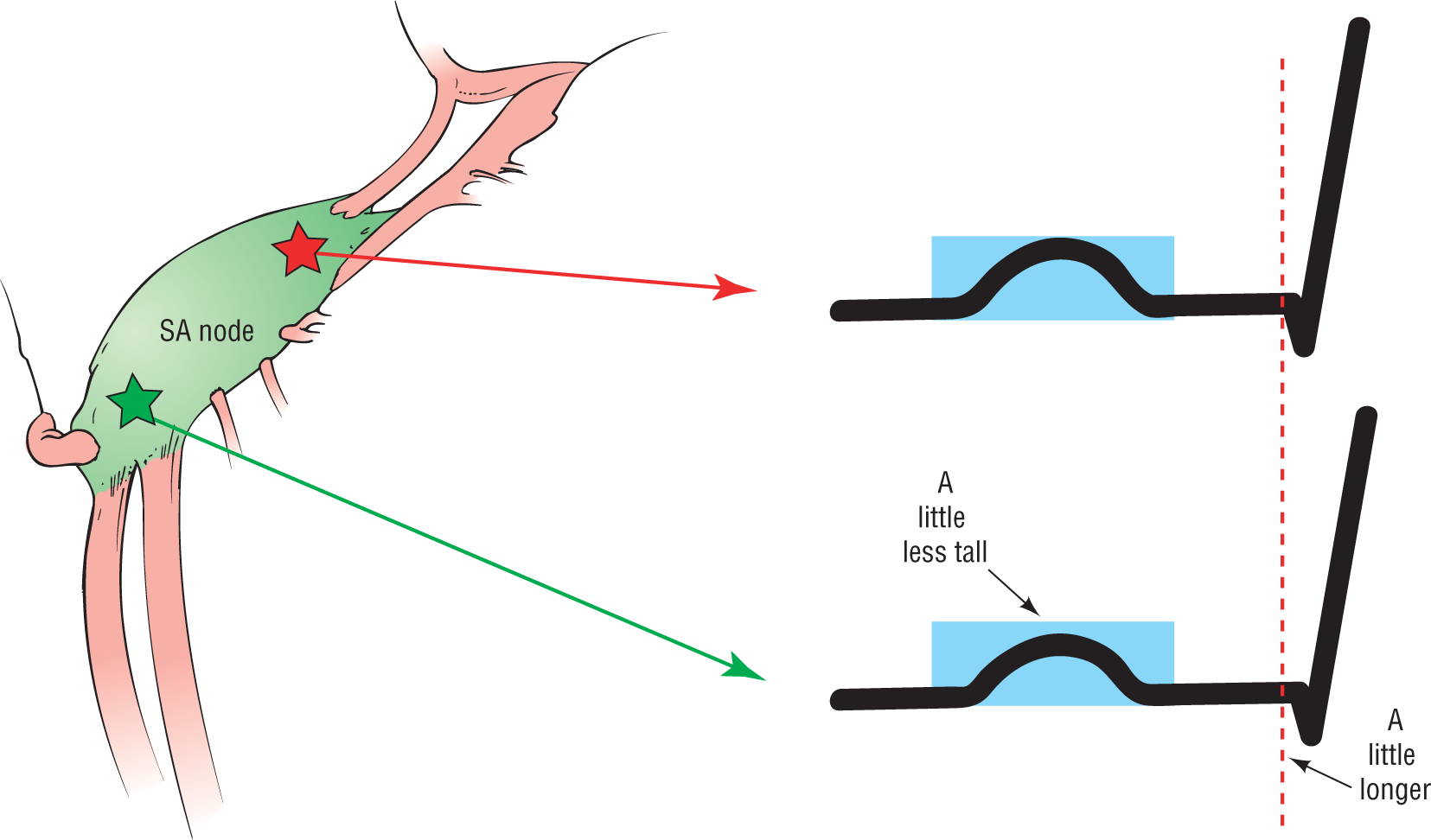
We should clarify something about P morphology and PR morphology. Electrophysiology studies have shown us that there can be some minimal differences in appearance between P waves and PR intervals that start in the same SA node (Figure 8-17). The reason for this is that the SA node is not just one single cell, or even one small area, but rather a fairly long spindle-shaped structure. The pacing cells can sometimes vary within the SA node, and these minor differences in location can cause very minimal alterations in the morphology of the P and the length that the impulse has to travel to reach the AV node, hence the PR interval. When we say “identical” in this book, we mean that they are so similar as to almost guarantee the same site of origin. Pacemakers located outside the SA node would cause fairly obvious morphologic differences that would be easy to identify.
Figure 8-17 There can be slight differences in appearance between P waves and PR intervals that start in the same SA node.