
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Discussion:
ECG 8-1 is a typical example of a normal sinus rhythm that is toward the slower end of the spectrum. It is just barely over 60 BPM, so it fits between the range of 60 and 100 BPM that is needed for NSR. The P waves are all the same morphology and the PR intervals are all identical. This is critical in determining the rhythm because it means that all of the complexes originated within the same pacemaker, in this case the sinus node. The P-P intervals are the same and the rhythm is very regular. The QRS complexes are all less than 0.12 seconds long and are similar in morphology. This rounds off all the necessary criteria for the diagnosis of NSR.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 60 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Normal sinus rhythm |
Discussion:
ECG 8-2 shows all of the characteristics of NSR. Notice that the QRS complexes are relatively isoelectric (the same distance in the positive and negative directions). The orientation of the QRS complexes does not enter into the diagnosis of NSR in any way, and you should not worry too much about it for now.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 80 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Normal sinus rhythm |
Discussion:
ECG 8-3 is also NSR. Notice that in this case, the QRS complexes are all negative. Once again, the orientation of the complexes should not enter into the diagnosis. The P waves are notched but this is a normal finding.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 95 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Normal sinus rhythm |
Discussion:
In ECG 8-4, we decided to show you an example of a rhythm strip with really small QRS complexes. Don’t let the size of the QRS complexes or the flipped T waves fool you—it is still NSR. Remember, you cannot meet the criteria for small complexes on a rhythm strip; you need the whole ECG to make that determination.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 100 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Normal sinus rhythm |
Discussion:
ECG 8-5 shows some pretty tall QRS complexes and some deep, inverted T waves. The rhythm, however, is NSR. Don’t let the size of the complexes or any other pathology steer you from making the correct call on the rhythm. Remember, to really talk about cardiac pathology, you need a full 12-lead ECG and not just a rhythm strip.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 65 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Normal sinus rhythm |
Discussion:
We decided it was time for the first curveball. ECG 8-6 also shows some very small complexes. To simplify matters, we labeled the P wave, the QRS complex, and the T waves for easy identification. The morphology of some of the P waves shows some slight irregularities. Could this be multiple pacemakers at work? The answer is no. Notice that the PR intervals are the same and that the rhythm strip is very regular. Remember, different pacemakers would alter the regularity, the P wave morphology, and the PR interval. This is NSR.
This would be tough to figure out if it were a tachycardic rhythm, wouldn’t it?
Additional Information
When Normal Sinus Rhythm Becomes More Tachycardic

From Arrhythmia Recognition: The Art of Interpretation, Second Edition, courtesy of Tomas B. Garcia, MD.
In ECG 8-7, the worst-case scenario comes true. This is the same patient as in ECG 8-6, but much more tachycardic. Now it is tougher to decide what is a P wave, what is a QRS complex, and what is a T wave. You can make some educated guesses, but that is a big risk to take when a life is at stake. Can you figure out a way to easily determine what is what?
The easiest thing to do is to change leads and see if you can get more distinctive complexes in that lead. Another method is to get a strip with simultaneous leads on it, or better yet an ECG, to identify the complexes better. Take a look at Figure 8-18. In this strip, two leads were obtained simultaneously. In lead III, the complexes are more distinctive and it is easy to identify the various parts of the complex. Now it is just a matter of following up an imaginary line from an obvious QRS complex on lead III and find the corresponding spot on lead II. That spot on lead II has to be the QRS complex. Do the same thing on the next obvious QRS complex and place your calipers between these two spots. Now, walk your calipers over and identify all of the other QRS complexes on the strip. The rhythm is easy to identify, even in lead II.
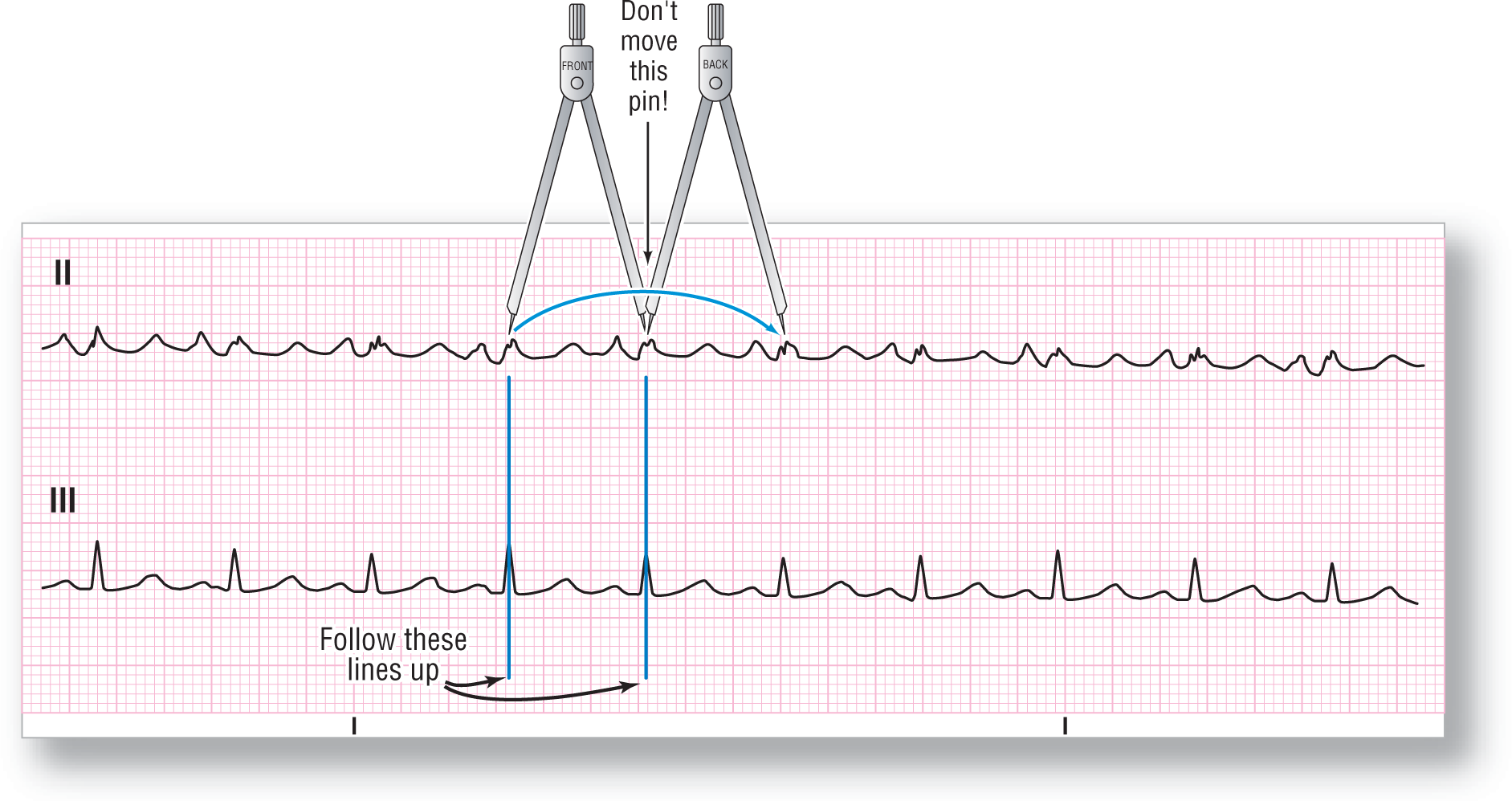
Figure 8-18 When attempting to measure complexes that are difficult to read, obtain a strip from another lead. This may help to clarify the ECG components and accurately measure the complexes.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
DescriptionHere is a clinical pearl: Contrary to popular opinion, lead II is not always the best lead to identify rhythms. Which is the best lead? The answer is that it varies from patient to patient. In some patients, it will be lead II. In others, it may be lead V1. In others, it may be aVL. You just never know. The take-home message is this: When you are dealing with a complex arrhythmia, obtain multiple leads or a full ECG. This makes identification easier and safer.
Additional Information
Key Points: Normal Sinus Rhythm
(If the QRS complexes were wide but the other criteria were all met, we would say that the rhythm was sinus but not normal sinus.)