From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
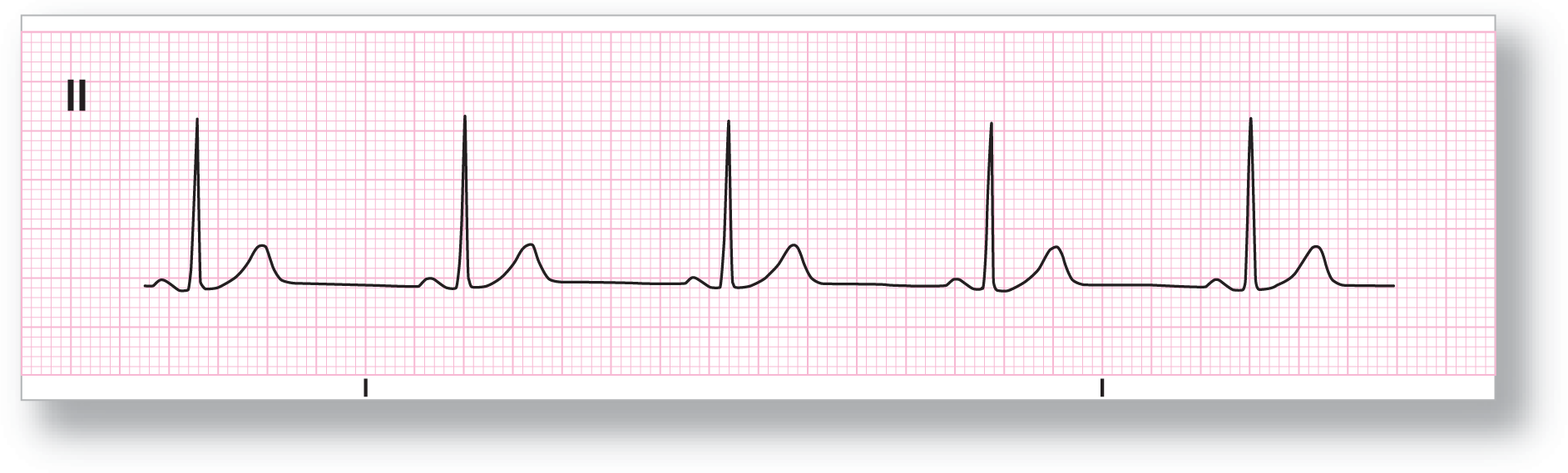
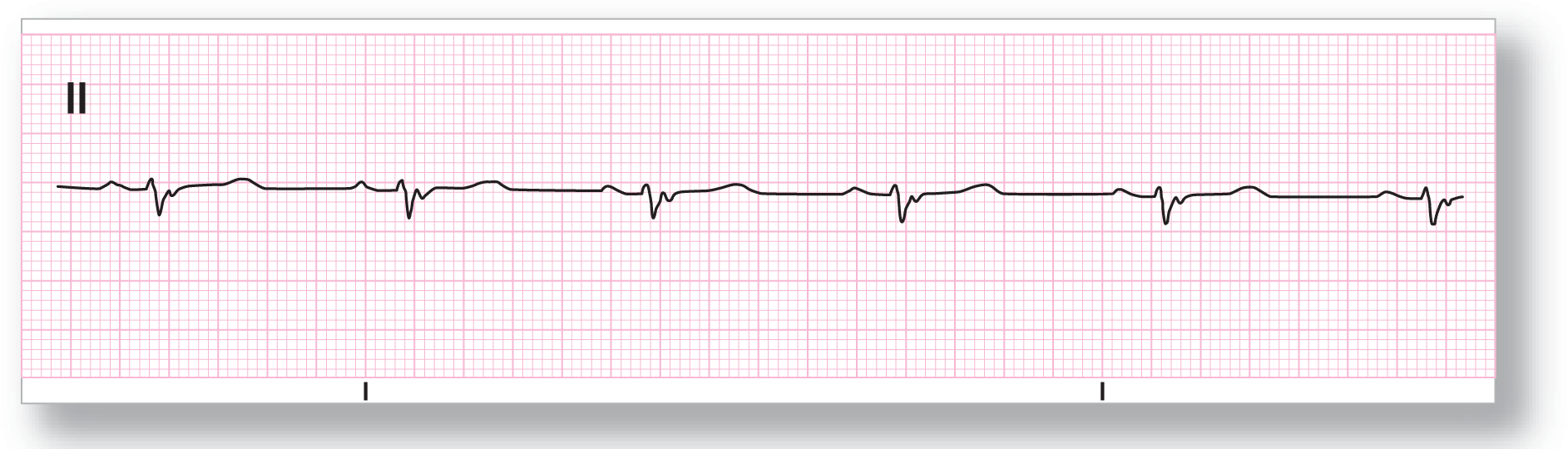
Rate: Slightly under 60 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
ECG 9-1 is an excellent example of sinus bradycardia. Notice the long, flat TP segments between each of the complexes. The waves are all normal duration and morphology. Lead II shows upright P waves so that you know that the P-wave axis is normal.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
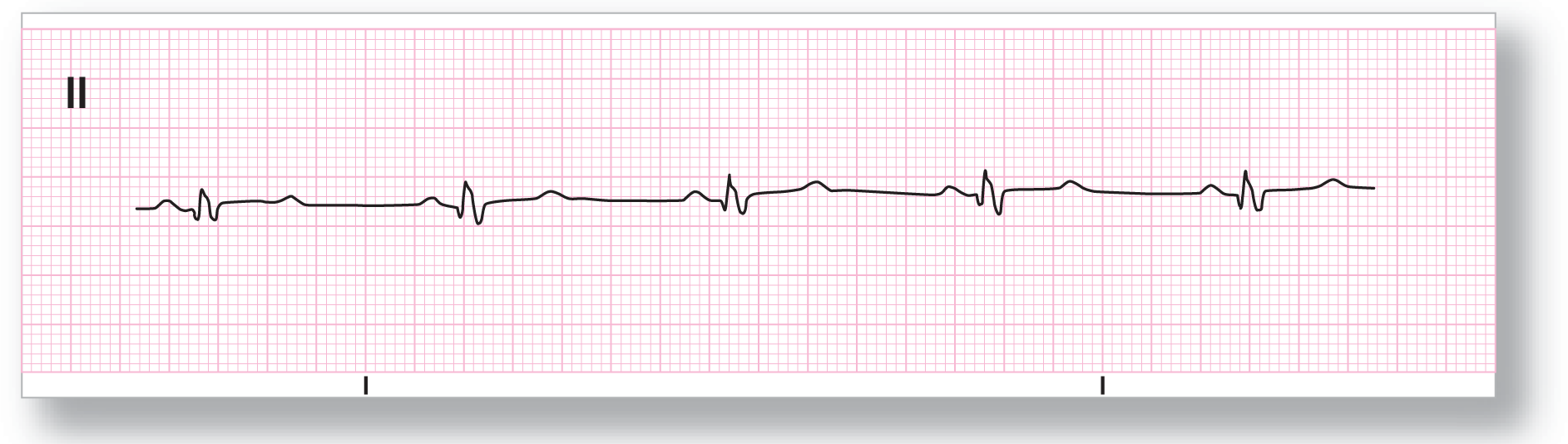
Rate: About 55 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
The first thing to catch your eye in ECG 9-2 is the relatively small size of the QRS complexes. However, they are still easily identifiable. The intervals and waves are all normal. The only interval that may be slightly widened is the QRS interval. However, on close examination, we note that the complexes are about 0.11 seconds and within the normal limits. Once again, the P waves are upright in lead II. This is sinus bradycardia. If the QRS complexes were wider than 0.12 seconds, we would have two possibilities: (1) sinus bradycardia with aberrantly conducted ventricular complexes and (2) sinus bradycardia with a bundle branch block. Comparison of this strip with others from the past would help answer the aberrancy question. An ECG would help distinguish the bundle branch block question easily. Comparison of this new ECG with an old one would help to distinguish if the bundle block is new.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
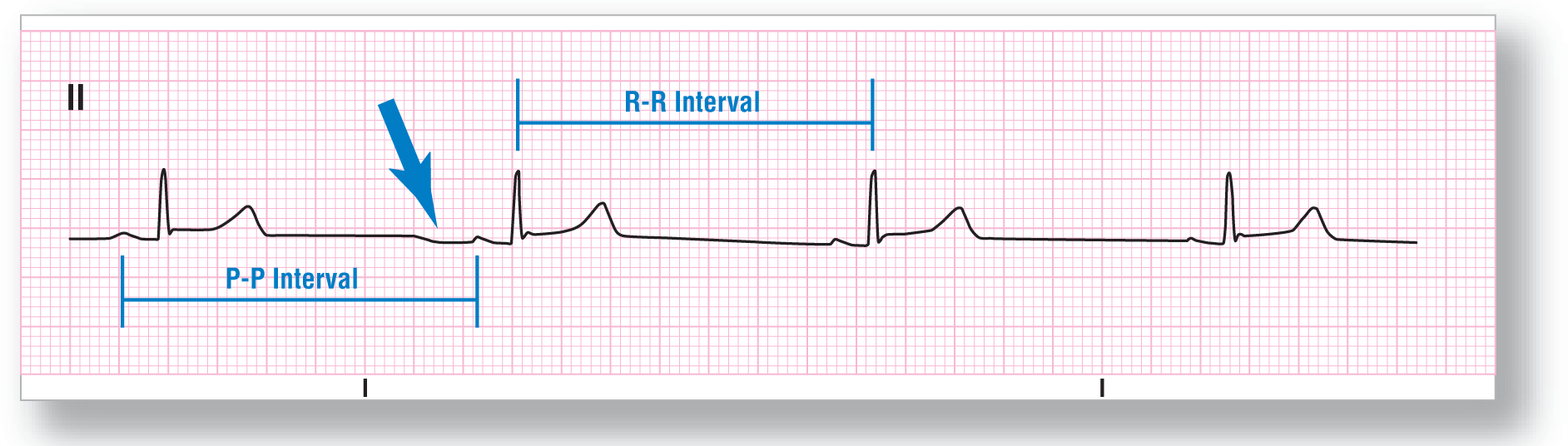
Rate: Slightly under 45 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
ECG 9-3 shows a really slow rate with complexes that appear fairly normal. At first glance, it is obviously sinus bradycardia. Even though this diagnosis is correct, the criteria are a bit clouded. Take a look at the second P wave. Does the morphology look different? It is a bit different. Could it be a premature atrial contraction (PAC)? The answer is no, because the P-P and R-R intervals are the same throughout the entire strip. If the complex were a PAC, the abnormal P wave and its corresponding QRS complex should have occurred sooner than expected. This one came out exactly on time. So, what caused the morphology of that P wave to be different? Notice that right before the P wave, there is a dip in the baseline (see blue arrow). This dip almost breaks the P wave in two with the second half being normal. The dip is probably due to some movement of the patient or the leads. This dip, and not an ectopic P wave, is the cause of the alteration in the morphology of the P wave. The keys to making the diagnosis are the regularity and the overall similarities between all of the complexes. Remember to always look at the company the pathology keeps; if it is not there, think about the alternatives.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
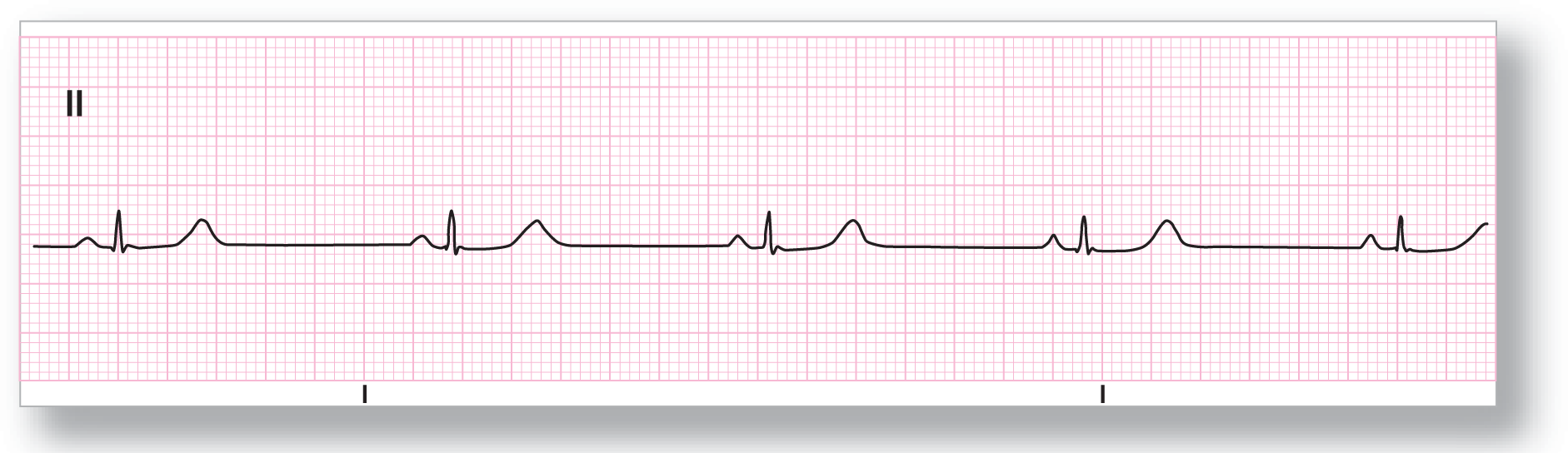
Rate: About 45 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
ECG 9-4 also has some very small QRS complexes. The rate is very slow at 45 BPM. The P waves, PR intervals, and QRS complexes are all similar in morphology and duration. This is another example of sinus bradycardia. You should clinically evaluate this patient, and anyone who is severely bradycardic, closely for any signs of hemodynamic insufficiency.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly under 60 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
ECG 9-5 meets all of the criteria for sinus bradycardia. The QRS complexes, if you measure them, are wider than 0.12 seconds. You will need to do some investigation to rule out aberrancy or another cause for the wide QRS complexes. When we performed an ECG and compared it to an old one, we found out that the patient had a long-standing bifascicular block with a right bundle branch block and a left anterior hemiblock. The P waves were identical to the ones found in prior ECGs and strips, so the rhythm is sinus bradycardia.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly under 60 BPM |
PR intervals: Prolonged, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present |
Rhythm: Sinus bradycardia |
Discussion:
Did you notice anything peculiar on ECG 9-6? If you did not, go back and examine it again, this time taking some extra time and measuring all of the intervals. The patient definitely has a rate less than 60 BPM and the P waves are upright in lead II. The QRS width is less than 0.12 seconds, which is normal. The problem lies in the PR interval. The PR interval is prolonged by being over 0.20 seconds (one big block). For now, just be aware of the problem and document it. Later on, after we discuss atrioventricular (AV) blocks, you will call this sinus bradycardia with a first-degree AV block.