As its name implies, a sinus block (SA block) refers to a complete block or failure of the sinus node to capture or depolarize the atrial myocardium. The block can last for one, two, or more cycles, but the hallmark of a sinus block is that the pause is always an exact multiple of the normal P-P interval (Figure 12-1). The block is an exact multiple of the P-P interval because the sinus pacemaker, unaware of the block that is occurring farther down the line, continues to fire at its intrinsic rate. Eventually, one of the sinus impulses will be able to get through to capture the atrial myocardium and end the SA block.
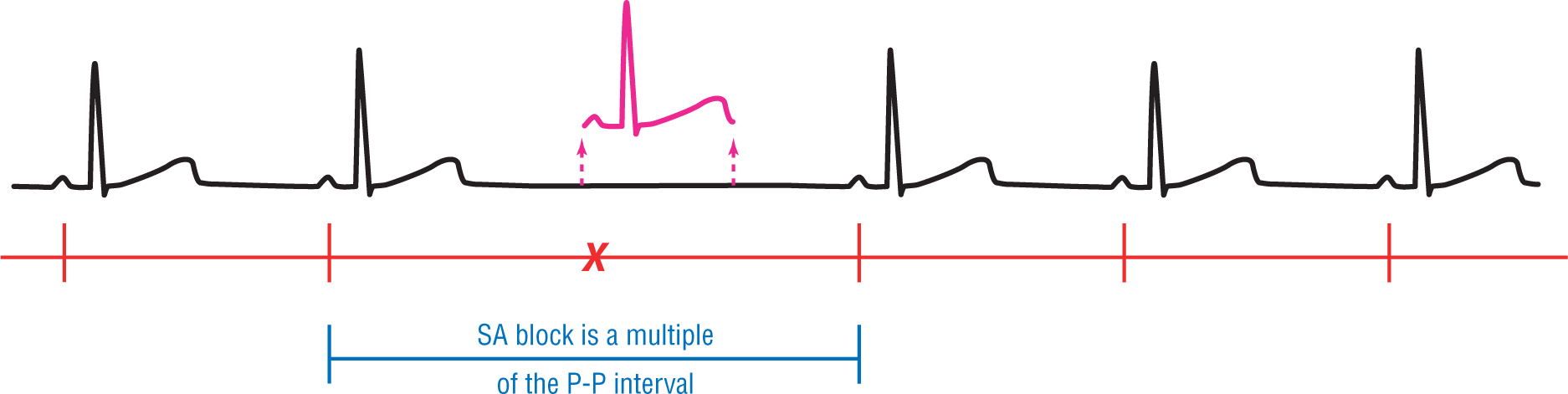
Figure 12-1 A sinus block occurs when the SA node is completely prevented from conducting the impulse to the atria but the pacemaker itself remains untouched. For this reason, the underlying cadence of the rhythm remains untouched. SA blocks are always some multiple of the P-P interval. In this case, note that the SA block is two times the normal P-P interval.
Take a look at Figure 12-1. Note that there is a normal sinus rhythm occurring at the intrinsic rate set by the sinus pacemaker. Suddenly, one of the impulses fires (see red X) but that depolarization wave does not reach the atrial tissue and does not form a P, QRS, or T wave (see purple complex). However, the sinus rate or cadence is not interrupted by the block and it continues to fire on schedule. The pause is two times the normal P-P interval. If two complexes were blocked, the pause would be three times the normal P-P interval, and so forth. The key is that the pause is always an exact multiple of the P-P interval (Figure 12-2).
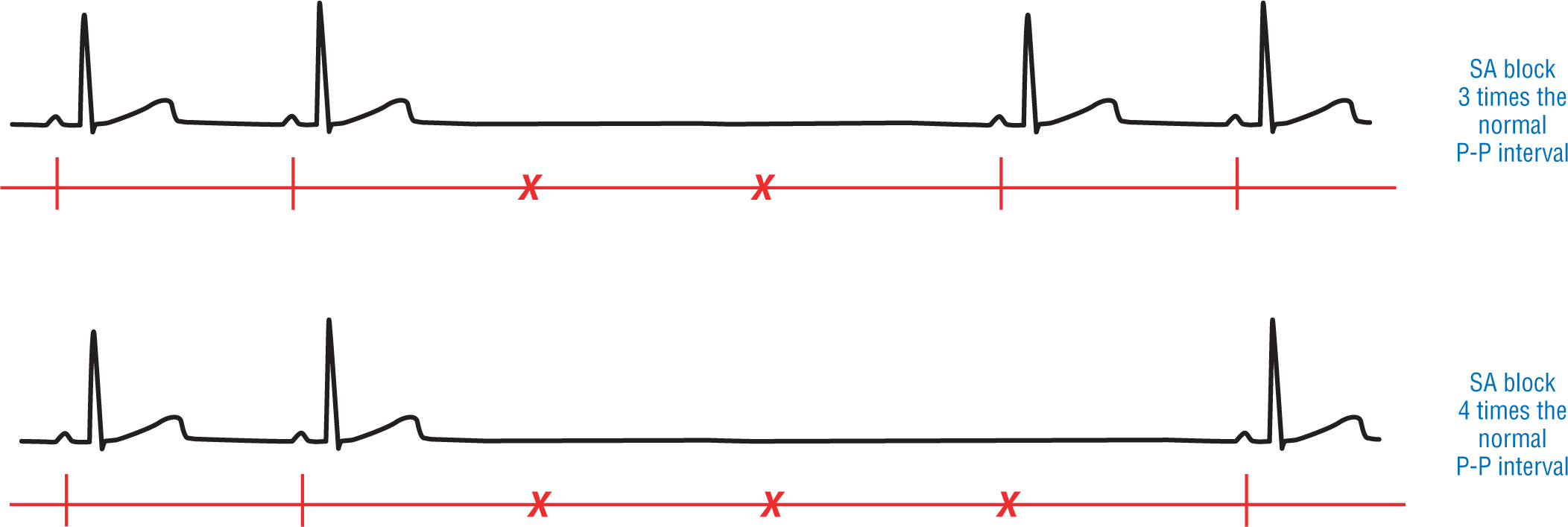
Figure 12-2 Other examples of sinus block. The top one shows a strip where two consecutive sinus impulses were blocked from reaching the atria. The bottom strip shows a strip where three consecutive sinus impulses were blocked from reaching the atria. Note that the pause is always a direct multiple of the normal P-P interval.
There is one thing that commonly occurs and can mimic a sinus block: a blocked premature atrial contraction (PAC; see Chapter 13, Premature Atrial Contraction). Basically, another sinus pacemaker or an ectopic atrial pacemaker fires earlier than expected. That impulse depolarizes the atria but is blocked by the AV node from ever reaching the ventricles. The net result is that you have a P wave but no QRS or T waves. Sometimes that P wave will fall on and fuse with the previous T wave. Note, however, that there is always a P wave in a PAC, blocked or not. In sinus blocks, there are no P waves because the impulse never reaches the atria and, therefore, does not depolarize the atrial tissue to form a P wave.
The sinus blocks can occur intermittently on the same strip and can sometimes be mistaken for a severe sinus bradycardia (Figure 12-3). Obtaining a longer strip in these patients will be very helpful in making the diagnosis.
Figure 12-3 Two nonconsecutive sinus blocks on the same strip. Note that the middle and end of this strip could easily be mistaken for a sinus bradycardia. One clue to the presence of block would be that sinus bradycardia is formed slowly by a gradual slowing of the rate and does not occur as abruptly as that seen in Figure 12-2.