Hint #2: Always Evaluate the P-Wave Morphology and the PR Interval
Inverted P waves can be found in two circumstances: (1) low or distal ectopic foci in the atria and (2) P waves with retrograde conduction to the atria from the AV node or ventricles. We presented the concept of low or distal ectopic foci in the atria in Chapter 13, Premature Atrial Contraction, and we will give you a short review here. In this chapter, we will introduce the concept of retrograde conduction of the P waves from the AV node. This topic will be covered in much greater detail later in the book.
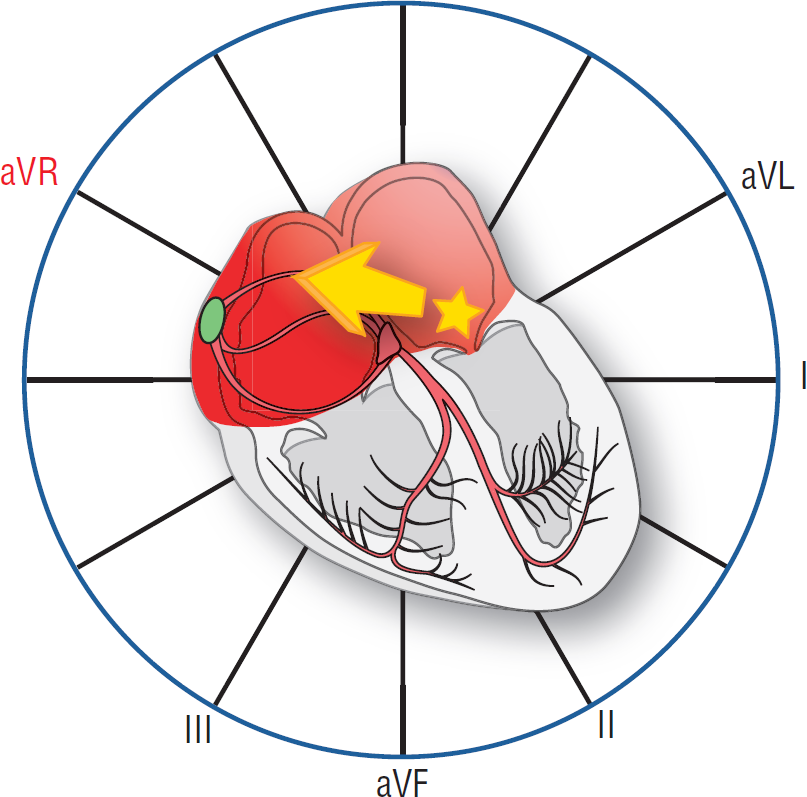
If you remember, a low ectopic focus near the AV septum will cause a depolarization wave to develop that must primarily spread upward toward the upper poles of the atria (Figure 14-5). This depolarization wave gives rise to a vector that heads away from leads II, III, and aVF, causing a negative P wave to appear on the strip in those leads. Since the depolarization wave must still cross the physiologic block produced by the AV node, the PR interval would be normal or slightly different than a sinus complex. This concept, a normal or near normal PR interval, is critical in your differential diagnosis of the origins of a rhythm with an inverted P wave.
Figure 14-5 An ectopic focus and its P-wave vector. This Figure graphically represents the P wave vector as a yellow vector heading superiorly and to the right. Note that the vector is heading toward the positive pole of lead aVR only. P waves produced by this focus would be negative and inverted in leads I, II, III, and aVF.
Now that we understand how a low ectopic atrial pacemaker gives rise to inverted P waves, let’s turn our attention to retrograde conduction through the AV node. Remember, any tissue in the heart can act as a primary pacemaker if the circumstances are just right. The AV node is no exception to this rule. There are many cases in which the AV node functions as a primary pacemaker. If the AV node functions as a primary pacemaker, we call the rhythm a junctional rhythm. We will spend quite a bit of time talking about junctional rhythms in Section 4, but for now, let’s just look at retrograde conduction from the AV node.
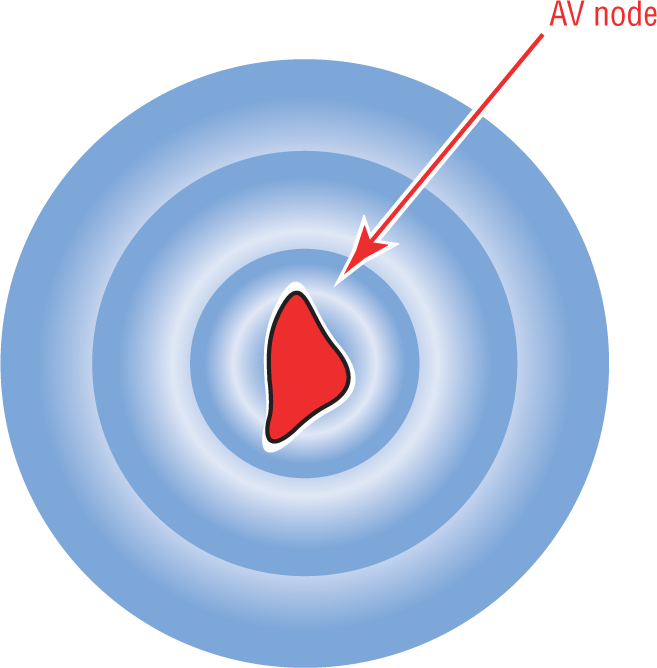
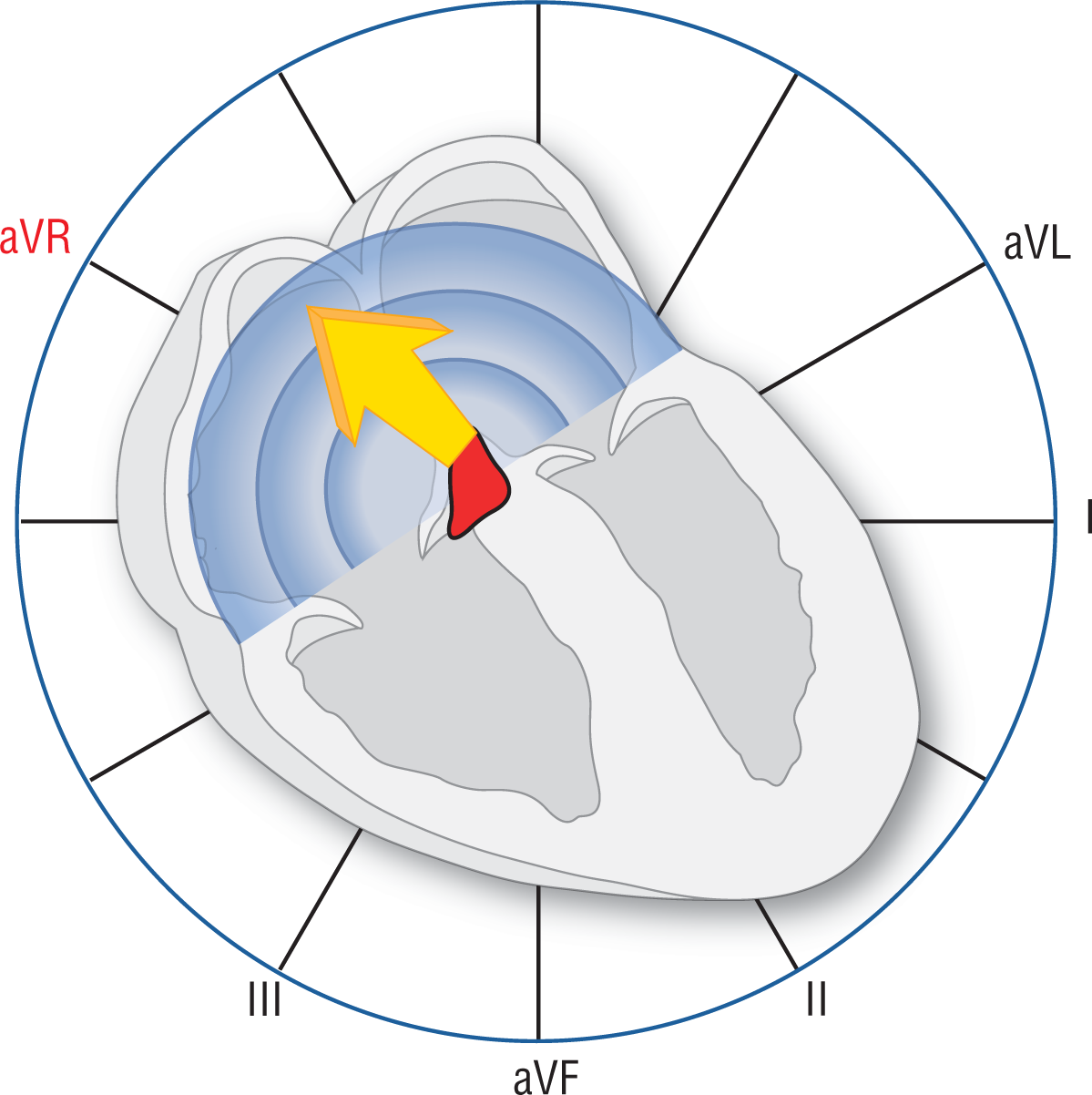
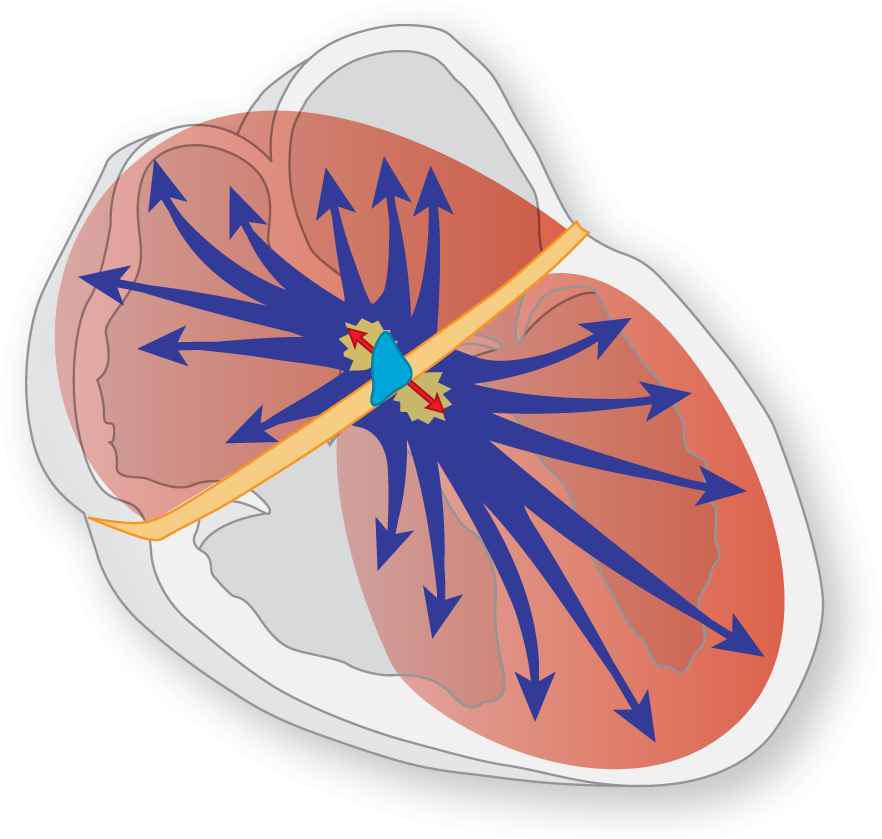
Picture in your mind a complex originating in the AV node. In which direction would the depolarization wave spread? The answer is that the impulse would spread in a circular fashion radiating outward from the primary focus (Figure 14-6). In the case of the ventricles, it would proceed down the electrical conduction system as it normally should. This gives you a nice, tight QRS complex. How about the atria? Well, the impulse would radiate upward and outward through the atria, giving you a vector that is directed superiorly away from leads II, III, and aVF (Figure 14-7).
Figure 14-6 Depolarization wave originating in the AV node. An impulse originating in the AV node creates a depolarization wave that moves outward in all directions.
Figure 14-7 Retrograde conduction of the P wave. The depolarization wave travels outward through the atria by direct cell-to-cell transmission, giving rise to a vector directed upward. This causes a negative deflection on the rhythm strip in leads II, III, and aVF. Since the impulse travels backward from the AV node through the atria, it is called retrograde conduction. The impulse progresses normally (antegrade) through the ventricles via the electrical conduction system.
So, why did we introduce the concept of junctional complexes and their inverted P waves at this time? Because it is almost impossible to tell whether an inverted P wave originated in the atria or the AV node based on its morphology alone. To make the correct diagnosis, we need to look at “the company it keeps.” We need to look at the PR interval. By convention, if the PR interval is equal to or greater than 0.12 seconds in a complex with an inverted P wave, it is considered to be atrial in origin. If the PR interval is less than 0.12 seconds, then the complex is considered to have originated in the AV node. This is critical information that you will need to use over and over again.
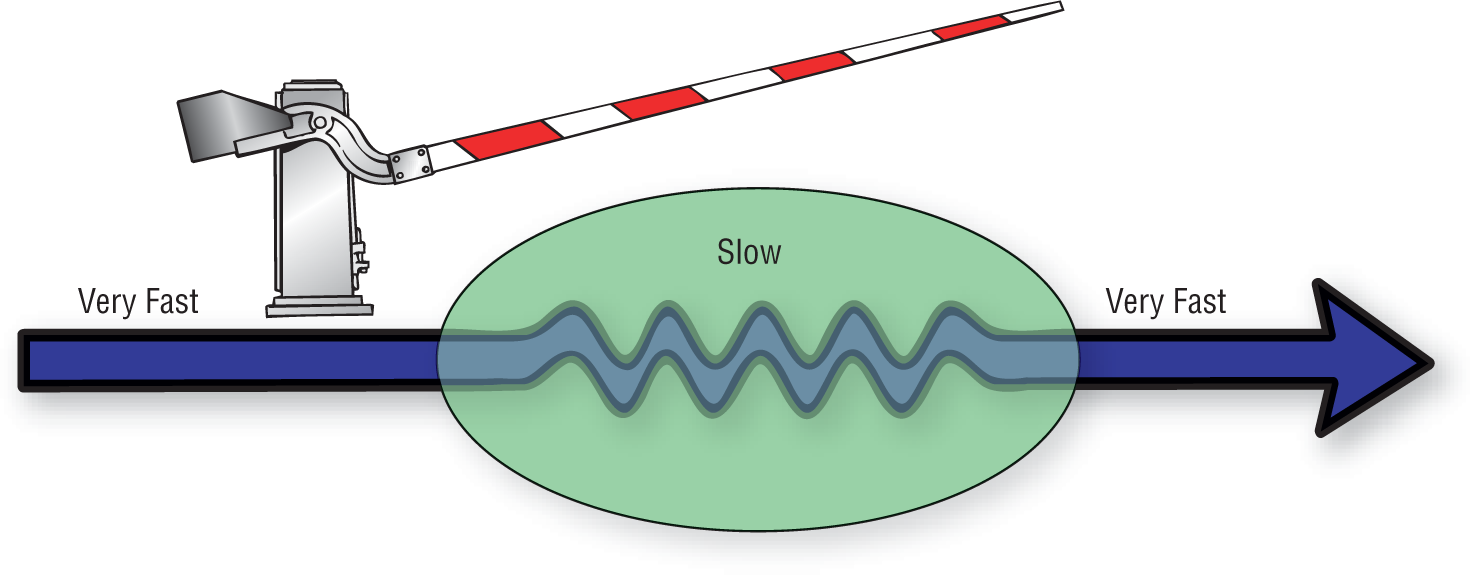
In Chapter 1, Anatomy and Basic Physiology, we talked about the concept of the AV node being like a guardhouse causing the physiologic block (Figure 14-8). Continuing with this analogy, let’s suppose that an impulse originated in the atria. That impulse would have to undergo the physiologic block imposed by the AV node before moving on to the ventricles. The physiologic block would make the PR interval fall into the normal or slightly prolonged range.
Figure 14-8 The AV node functions as a gatekeeper between the atria and the ventricles. An atrial impulse would have to undergo the physiologic block imposed by the AV node before moving on to the ventricles.
Now, suppose that the impulse originated in the AV node itself, as occurs in a junctional complex. Would the impulse have to undergo the physiologic block to get back to the atrium? No, because the physiologic block only slows conduction antegradely (from the atrium to the ventricles). It doesn’t cause the slowing effect retrogradely at all. The impulse would spread almost instantaneously to the atria and the ventricles (Figure 14-9). The PR interval would be shorter than normal or the P wave would be buried within the QRS complex itself.
Figure 14-9 An impulse that originates in the AV node bypasses most or all of the physiologic block, making the PR interval much shorter or nonexistent.
The take-home point of this discussion is that if you have an inverted P wave in leads II, III, or aVF, you need to look at the PR interval for some additional information before assigning a name to the rhythm in question. If the PR interval is normal or prolonged (≥ 0.12 seconds), then the origin of the impulse can be assigned to the atria and the rhythm is an ectopic atrial rhythm. If the PR interval is shorter than normal, then the origin is probably in the AV node and the rhythm is junctional until proven otherwise.