
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
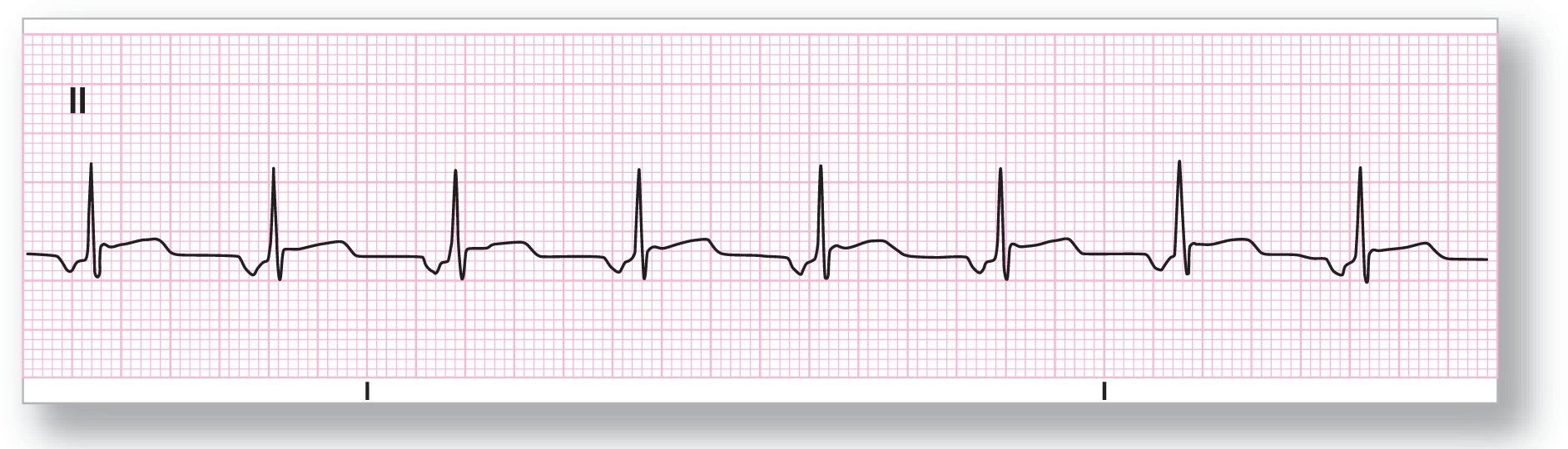
Rate: About 75 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
ECG 14-1 is a typical example of ectopic atrial rhythm. First, let’s look at the rate. In this case it is about 75 BPM. Next, look at the P-wave morphology. In this case, it is easy to see that the P waves are inverted in lead II, which is grossly abnormal. The inverted P waves rule out the possibility of a normal sinus rhythm. Since inverted P waves can be seen in both junctional rhythms and ectopic atrial rhythms, we have a decision to make. To help us with this decision, we look at the PR interval. In this case, the PR interval is within the normal range, making the diagnosis of ectopic atrial rhythm likely.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
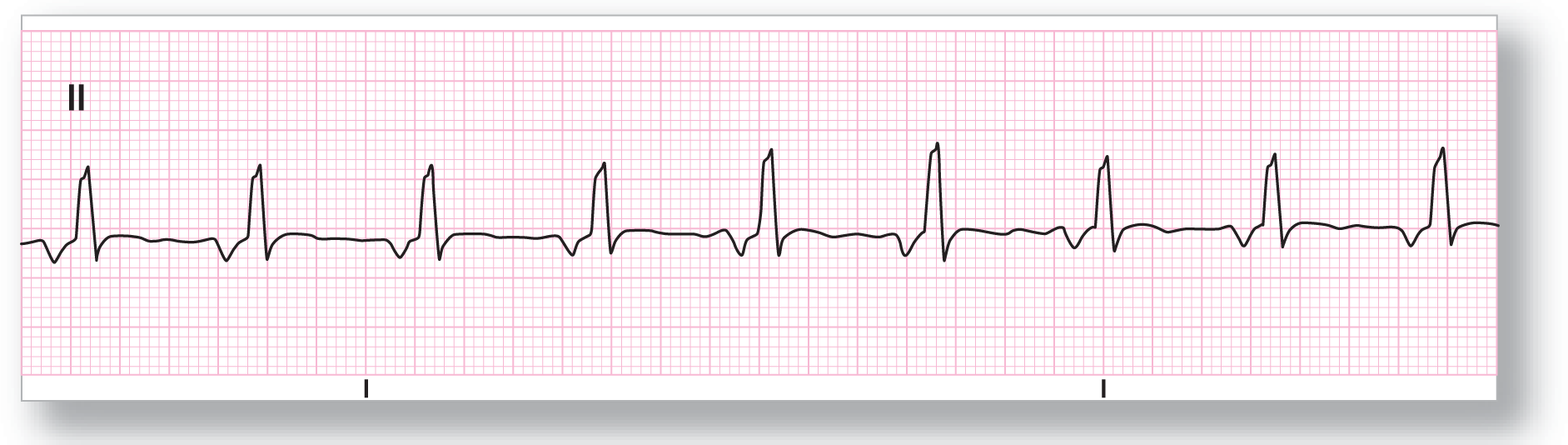
Rate: About 80 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
ECG 14-2 is also a good example of an ectopic atrial rhythm. Following the same logic as above, the inverted P waves and the normal PR intervals clinch the diagnosis. Should you get a regular 12-lead ECG on this patient? Yes, you should because of the presence of a rhythm abnormality and the ST-segment elevation. Remember, it is better to be safe than sorry!

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 50 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
ECG 14-3 poses more problems than the previous ones. Why? Because the rate is so slow. It is about 50–55 BPM. This rate could very easily fit with a junctional rhythm, which is usually about this range. Once again, our saving grace is the presence of a normal PR interval. The normal PR interval makes the diagnosis of ectopic atrial rhythm more likely. Medications can often cause a significant bradycardia, and you should evaluate this and other possibilities as well for your patient.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 75 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
The inverted P waves and the normal PR interval make the diagnosis in ECG 14-4. By now, you should be feeling a bit more comfortable with the possibility of an ectopic atrial rhythm. Remember, however, to always try to obtain an old ECG to verify your suspicions and confirm your diagnosis.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 85 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
ECG 14-5 is a bit troubling because the QRS complexes appear to be wider. But are they? Using your calipers and some careful measuring, you will note that the QRS complexes are not wider than 0.12 seconds. Therefore, the inverted P waves, normal PR interval, and normal QRS complexes make the diagnosis of ectopic atrial rhythm the correct diagnosis. Comparison to an old ECG or rhythm strip would be, as always, very helpful in confirming your suspicions.
Now, suppose that the QRS complexes were wider than 0.12 seconds. What should you do differently if that were the case? The first thing to check is whether the patient had a bundle branch block of some sort in the past. The next possibility would be aberrancy in the conduction of the impulse to or through the ventricles. The aberrancy could be rate related, and a long rhythm strip may show the aberrancy coming and going as the patient’s heart rate changes. The aberrancy can also be caused by ischemia or a diseased portion of the conduction system, which causes longer refractory periods in that area. Electrolyte imbalances can often cause aberrancy or rhythm abnormalities to develop. After you have exhausted these possibilities, there could be some other rhythms that can cause a similar picture, but that is for later on in the book.