From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 320 BPM |
PR intervals: Not applicable |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
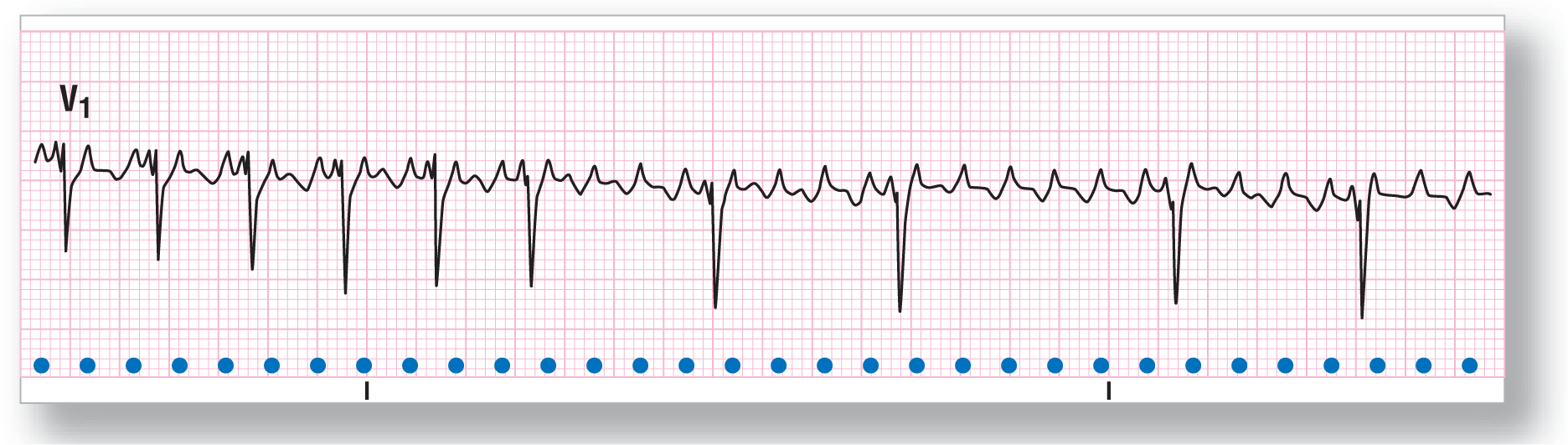
P:QRS ratio: 2:1, 4:1, and 6:1 |
Rhythm: Atrial flutter |
Discussion:
ECG 19-1 shows atrial flutter with varying conduction rates of 2:1, 4:1, and 6:1. The P waves are upright in lead V1, making them easy to spot. The area with 2:1 conduction shows partial fusion of the QRS complexes and ST segments with the F waves. Notice how much easier it is to identify the rhythm at the higher conduction rates. As is usually the case, the R-R interval is an exact variable of the F-F interval.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 320 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
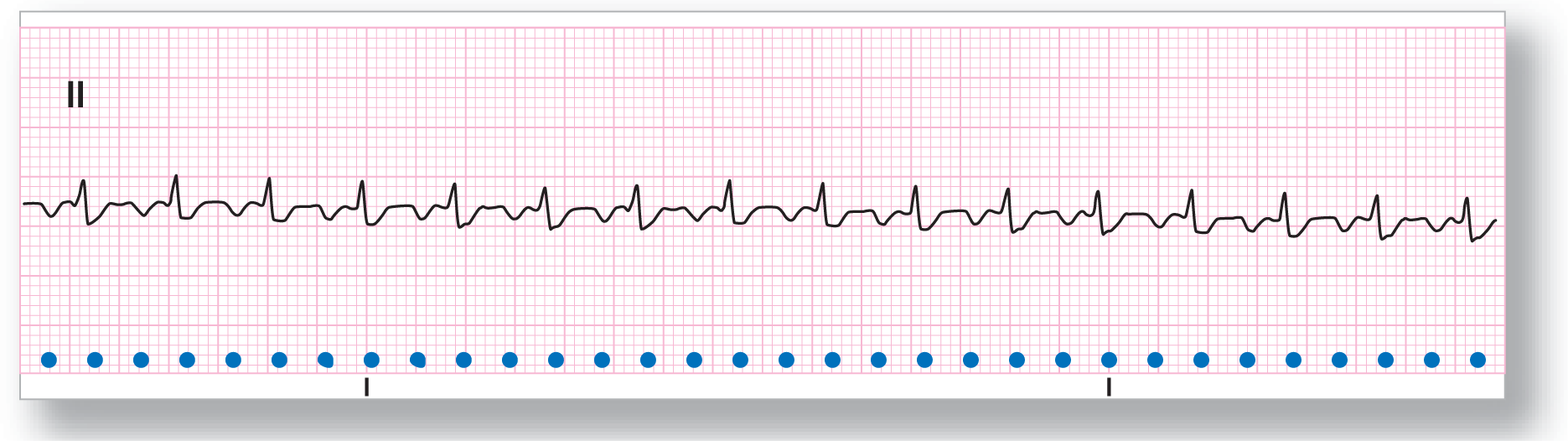
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter |
Discussion:
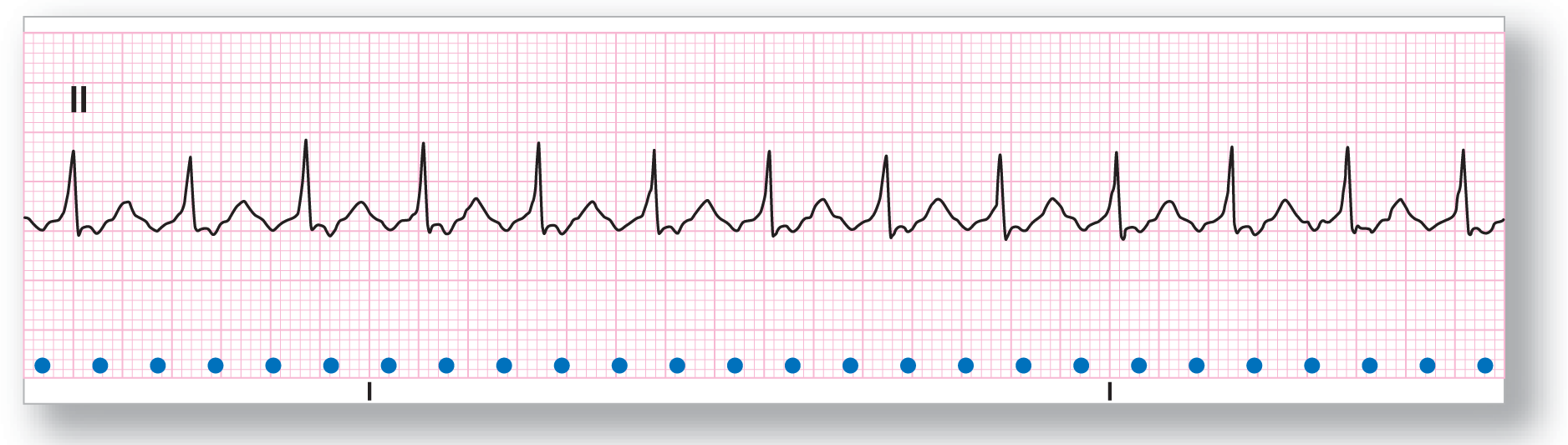
ECG 19-2 is one taken from the same patient as ECG 19-1, but in lead II. The patient was in consistent 2:1 conduction. Notice how the diagnosis is not as evident as in lead V1. The key to making the diagnosis in this lead is that the presumed PR interval is fairly wide and the presumed “P” waves are inverted. Taking half of this “P-P” interval demonstrates another inverted “P” wave at the exact halfway point. The rate and regularity make this atrial flutter and the “P” waves are actually F waves.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 270 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
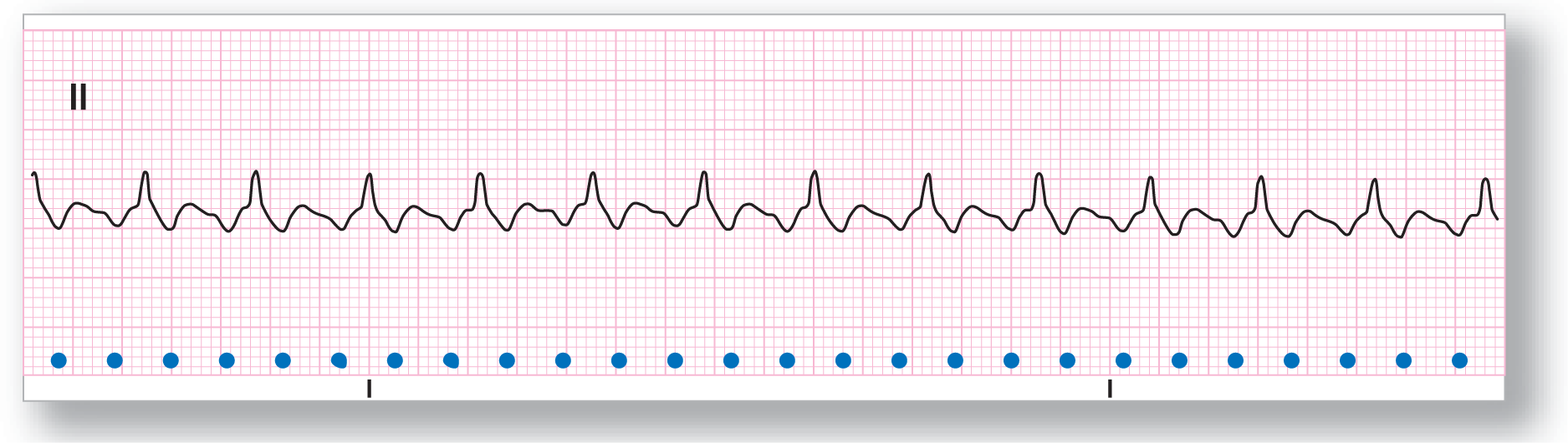
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter |
Discussion:
ECG 19-3 shows an atrial flutter with 2:1 conduction. The fusion of the QRS complex and ST segment with the saw-tooth pattern of the F waves makes the rhythm difficult to identify. Use your mind’s eye to remove the QRS complexes from the strip. The resulting saw-tooth pattern is evident. Once again, as in ECG 19-2, the key to the diagnosis is the rate, the inverted “P” waves, and the buried F waves found exactly halfway between the visible F waves. Use your calipers often!
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 300 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
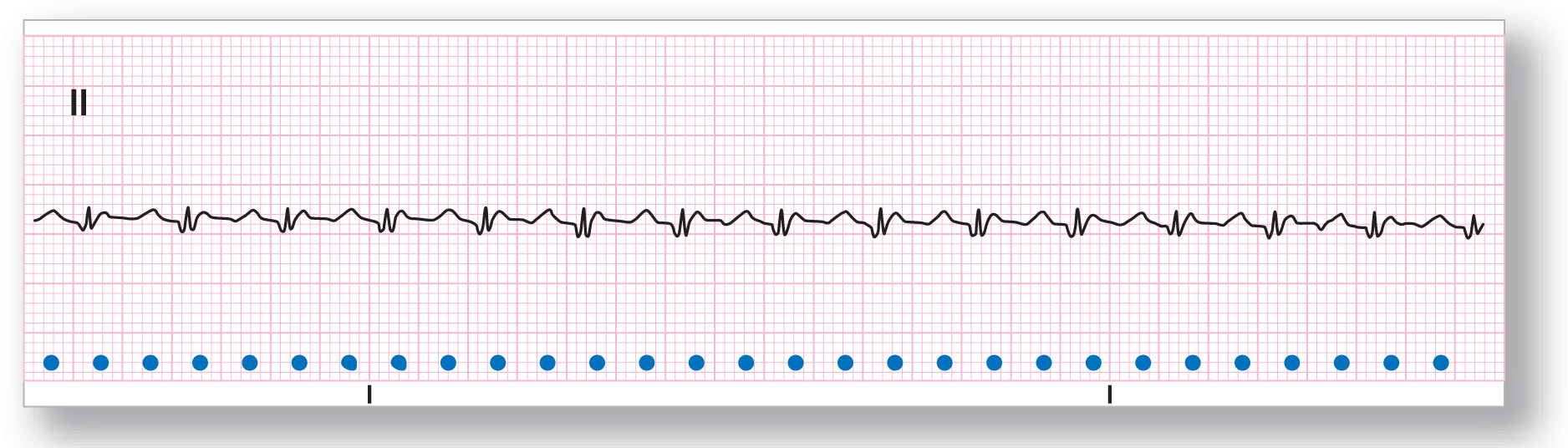
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter |
Discussion:
ECG 19-4 is very difficult to correctly identify. A little extra care and some mental manipulation of the strip should help you make the diagnosis. The ventricular rate is 150 BPM. That rate should immediately raise a red flag in favor of atrial flutter. Mentally removing the QRS complexes will show you the saw-tooth pattern of the underlying F waves. Take your calipers and measure the “F-F” interval. Divide that distance in half and map the rhythm strip. The buried F waves should be fairly easy to spot now.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 260 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter |
Discussion:
ECG 19-5 shows an atrial flutter with a very shallow saw-tooth pattern. It is difficult to see the constant undulation of the flutter waves on this ECG, but it is there. The key to identifying the undulation is the slow rise of the QRS complex, the very prominent T waves, and the apparent ST depression. The slow upstroke of the R wave and the prominent T waves are caused by a fusion of the positive end of the flutter waves. The ST depression is caused by the negative F waves.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 320 BPM |
PR intervals: Not applicable |
|
Regularity: Regular with two events |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter |
Discussion:
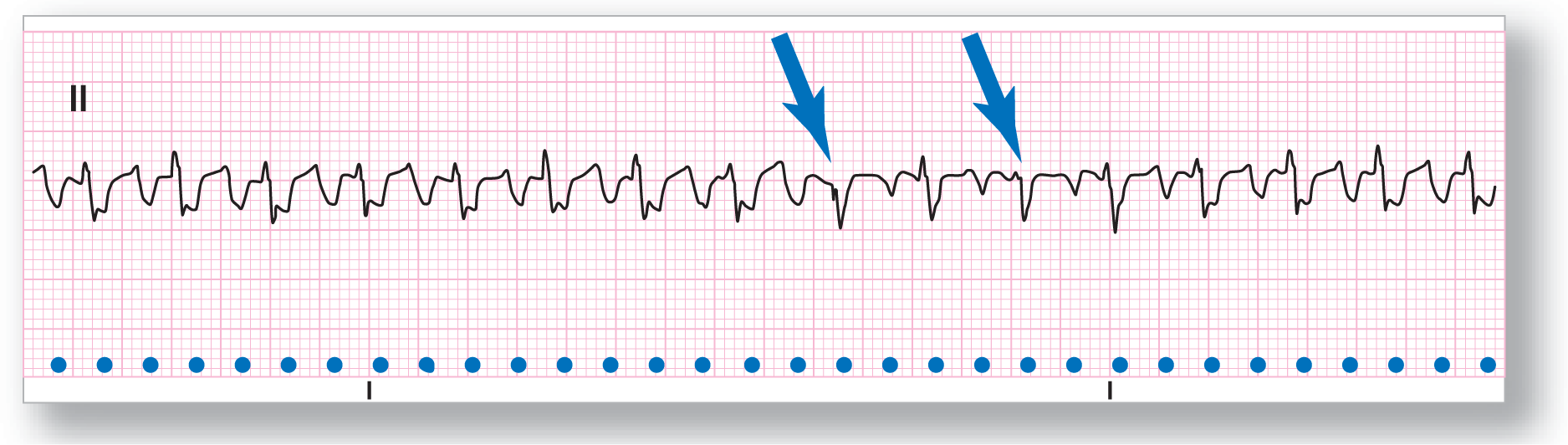
ECG 19-6 shows an atrial flutter with 2:1 conduction. There are two events visible on the strips, which we have highlighted with blue arrows. Can you figure out what they are? They occur later than expected, so they would have to be escape beats. They are narrow and follow the general morphology of the other QRS complexes, so they need to be atrial or junctional escape complexes. The less-than-prominent R waves in those beats are due to fusion with the underlying F waves.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 300 BPM |
PR intervals: Not applicable |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: Present |
|
Dropped beats: Present |
|
|
P:QRS ratio: Variable |
Rhythm: Atrial flutter |
Discussion:
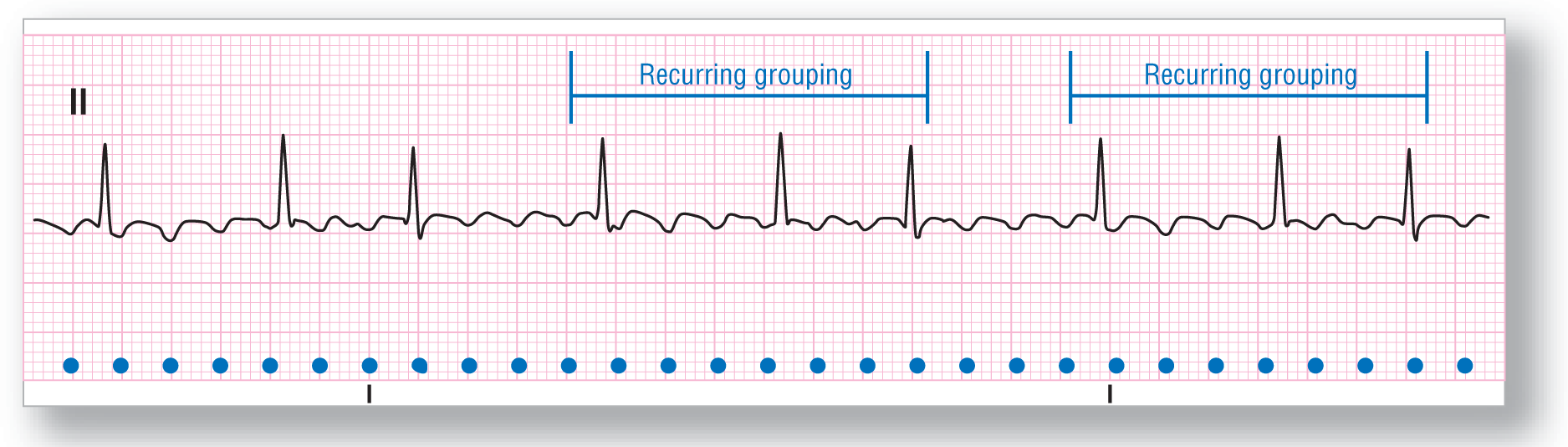
ECG 19-7 and ECG 19-8 have some information for advanced students. The first thing to note is the very obvious atrial saw-tooth pattern consistent with atrial flutter. The atrial rate is 300 BPM, which is a common rate for atrial flutter. The rhythm is regularly irregular, with associated grouping of the ventricular complexes. The regularity of the ventricular response means that this strip is not a true variable block. The grouping and the irregularity are instead classic for Wenckebach grouping (see Chapter 28, Atrioventricular Blocks).
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 300 BPM |
PR intervals: Not applicable |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: F waves present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: Present |
|
|
P:QRS ratio: Variable |
Rhythm: Atrial flutter |
Discussion:
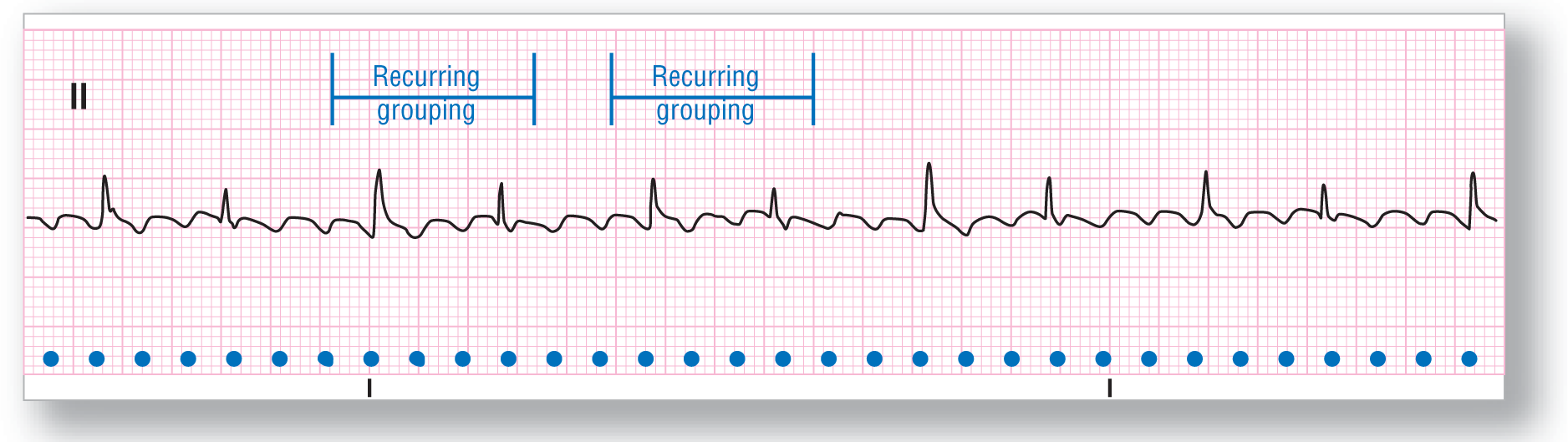
Once again, the saw-tooth pattern of atrial flutter is obvious on ECG 19-8. The QRS morphology of every other beat is slightly different than the others. Some grouping recurs throughout the strip. This could be consistent with Wenckebach grouping. In addition, the varying QRS morphology may be due to aberrancy, or fusion with the F waves, or they could represent escape complexes. Clinical correlation and a longer strip for study are indicated.