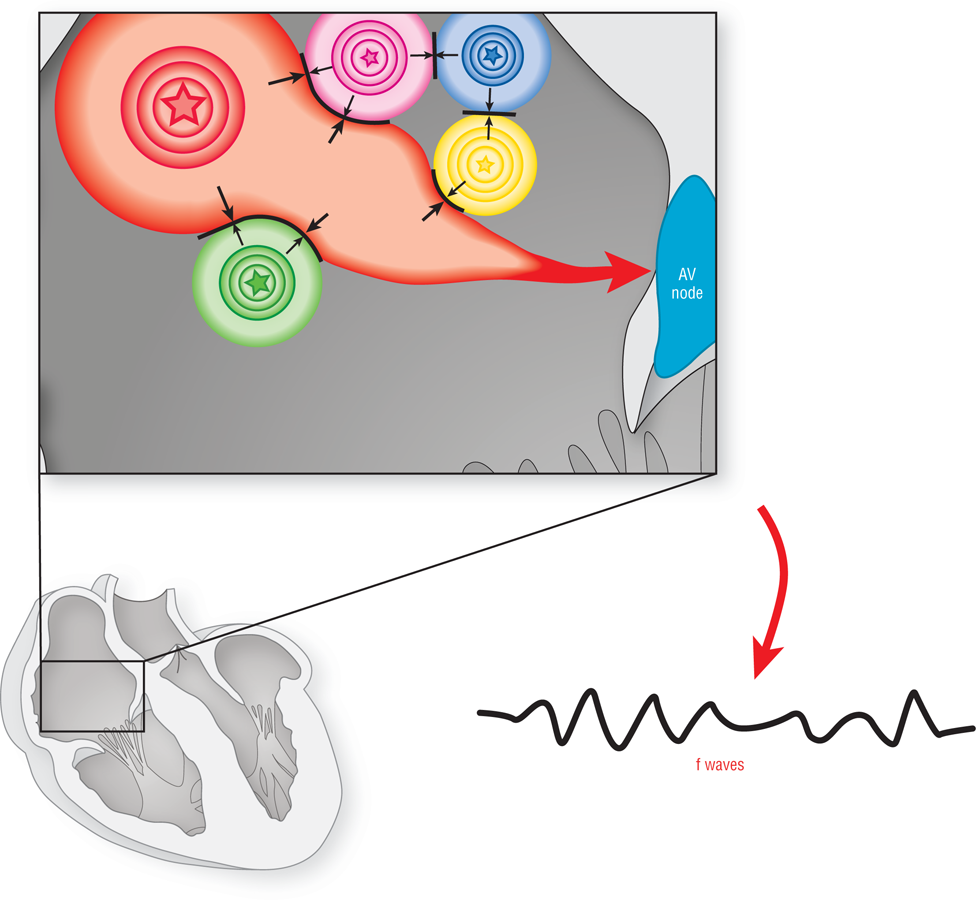
Let’s take a closer look at how f waves are made. Figure 20-2 shows a section of atrial myocardium during atrial fibrillation. Typically, there are multiple ectopic pacemakers all firing at the same time. The typical number of ectopic foci can be anywhere from the single digits to many tens of sites. These sites are in a constant struggle over which one will dominate.
Figure 20-2 In the atrial tissue there could be many, many individual ectopic foci acting as pacemakers at the same time. Most of these small islands of depolarization throughout the atria cancel each other out. These depolarization “wavelets,” however, create a small vector that shows up on the ECG strip as minimal deflections from the baseline. Since there are between 400 and 600 wavelets per minute, the resulting electrocardiographic changes are very small waves, known as f waves, which occur completely at random throughout the baseline.
As each focus fires, it causes the surrounding area of atrial myocardium to depolarize. Slowly, a localized depolarization wavelet begins to develop. They are called wavelets because they are very small and never become larger waves. These localized depolarization wavelets never make it big because they crash into the refractory areas created by the surrounding wavelets from other foci. Since each wavelet affects only a small amount of myocardium, they barely make a blip on the ECG strip. These wavelets, therefore, are the source of the vectors that are represented on the ECG strip as the f waves.
As you can imagine, the amount of atrial tissue involved dictates the size of the vector produced by any one wavelet. If there are only a few ectopic pacemakers causing the atrial fibrillation, then the amount of tissue involved (and their resulting vectors) will be bigger. The larger vectors cause larger f waves to appear on the ECG, resulting in a type of fibrillation known as coarse atrial fibrillation (Figure 20-3). If there are many ectopic pacemakers causing the rhythm, then the amount of tissue (and their vectors) involved in creating any one wavelet will be smaller. This leads to small f waves and fine atrial fibrillation. Some authors also talk about medium atrial fibrillation, but you should be aware that fibrillation can be anything from a straight line to a very aggressive random f-wave pattern. In other words, there can be an entire spectrum of possibilities and combinations that can develop with f-wave morphology. Present-day thought is that there is no clinical significance to the type of f waves involved.