Now, let’s turn our attention to the events that occur when the AV node functions as the primary pacemaker. When an impulse originates in the junctional area, the exact location of the ectopic focus strongly influences the resultant electrocardiographic representation of the complex, particularly the P wave. To examine this more closely, let’s go back to the water model we introduced you to in Chapter 6, How to Interpret a Rhythm Strip. Take a look at Figure 21-2. If you were to fill up the AV node area with water and then open up both floodgates, the result would be instantaneous flow of water into both the atria and the ventricles. The wave would travel against the expected flow in the atria (from inferior to superior) and would, therefore, stimulate the atria retrogradely. The ventricles would flood in the usual way (using the electrical conduction system) and would be identical to a normally conducted atrial impulse producing a nice, tight QRS complex.
Figure 21-2 If the lock in the middle of the container were filled with water and both gates were opened, the water would flow into both the atria and the ventricles. The water would spread evenly throughout both sides of the container simultaneously.
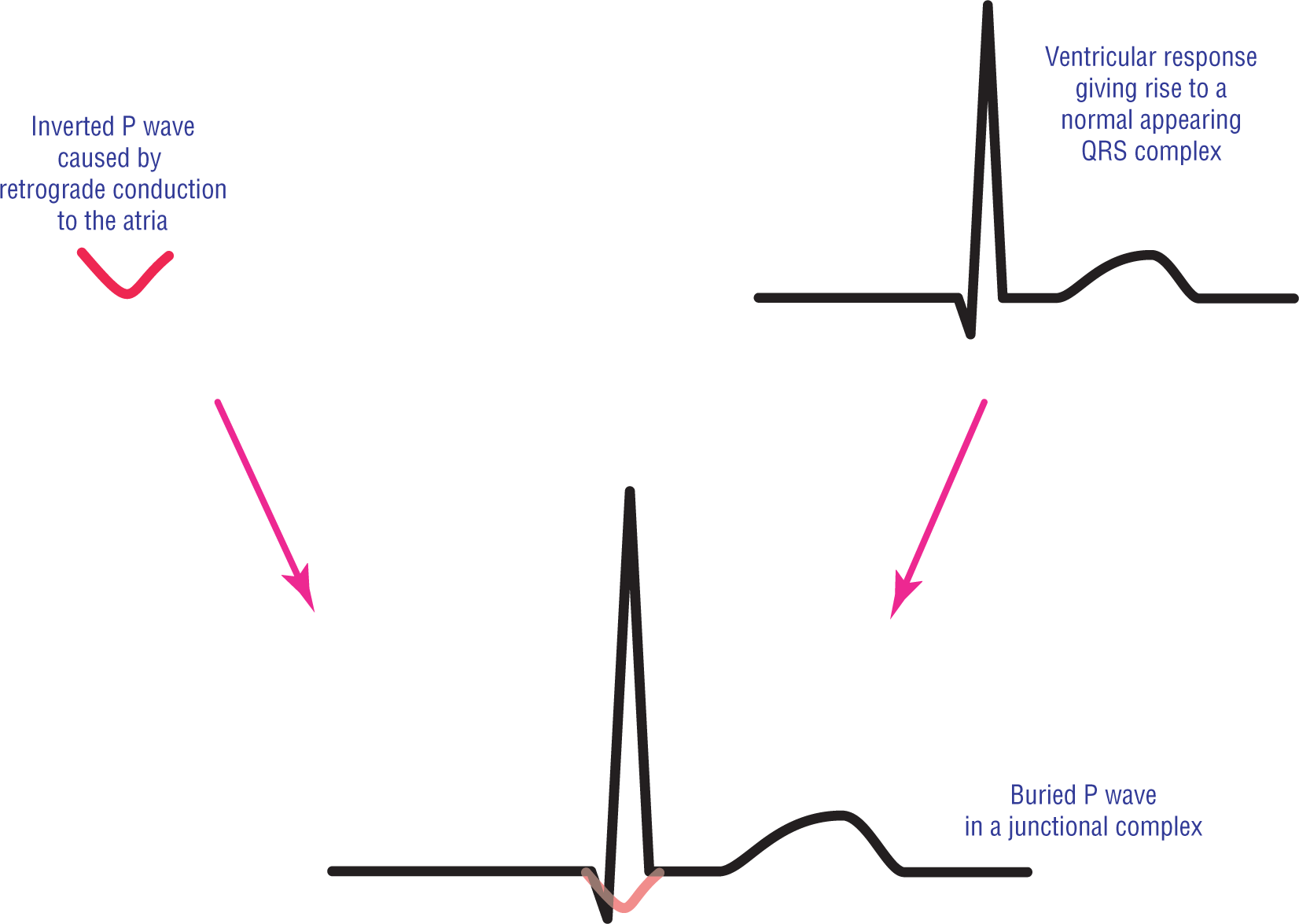
As we saw in Chapter 13, Premature Atrial Contraction, the result of the retrograde conduction of the impulse back to the atria would be an inverted P wave in leads II, III, and aVF. The result of the forward conduction through the normal electrical conduction system throughout the ventricles would be to produce a nice, tight supraventricular QRS complex. In the above example, the P wave and the QRS complex would occur at exactly the same time and the P wave would be buried inside the QRS complex. The net result on the ECG strip is that the P wave would either be invisible or would only account for a small amount of variation in the QRS complex (Figure 21-3). This is a very common presentation for a junctional complex on an ECG strip.
Figure 21-3 The appearance of a junctional complex with a buried P wave.
Now, let’s complicate the issue a little bit further. Suppose that you have an ectopic foci in the lower right atria (represented by the pink star in Figure 21-4). In Chapter 13, Premature Atrial Contraction, we saw that such an ectopic foci would form an ectopic atrial P wave that would be inverted in leads II, III, and aVF and that the complex would have a normal PR interval because forward flow would take it through the AV node and it would have to endure the normal physiologic delay.
Figure 21-4 Two ectopic foci are represented in this figure. One is a low atrial pacemaker and the other is in the transitional zone of the AV junction. In both cases, the depolarization wave would still have to go through most of the AV node and, thus, the physiologic block. The only big difference is that the complex originating in the transitional zone would have a shorter PR interval.
Now, suppose that the ectopic pacemaker was just a little farther along and just crossed into the transitional zone of the AV node (red star in Figure 21-4). What path would the depolarization wave now have to take? The answer is that this junctional depolarization wave would almost have to travel the same path as the lower atrial ectopic pacemaker! The only difference would be that the physiologic block would be shorter. The P wave would still be retrogradely spread backward into the atria and the forward depolarization wave would still have to undergo most of the normal physiologic block.
What would the resulting complex look like electrocardiographically? The P wave would not be buried in the QRS complex, as it was in the last junctional example we looked at. The P wave would occur before the QRS complex, but the PR interval would be short. Thus, we see that not all complexes that originate in the junctional area look the same. The location of the ectopic pacemaker site along the AV junction dictates the location of the P wave in relation to its QRS complex.
We’ve seen the appearance of the complexes resulting from ectopic pacers firing in the transitional zone and in the compact zone. Now, let’s take a look at what happens if the ectopic pacer is in the area of the bundle of His. In these cases, the depolarization wave is already past the sections that cause the physiologic block. In addition, the impulse is immediately transmitted to the ventricles. In order for the impulse to reach the atria, the impulse has to travel a much longer distance retrogradely through the other areas of the AV junction. Where would you expect the P wave to be in these cases? That’s right, the inverted P wave would come immediately after the QRS complex in the ST segment (Figure 21-5).
Figure 21-5 The appearance of a junctional complex originating in the distal AV junction or bundle of His. Note that the P wave is found after the QRS complex.
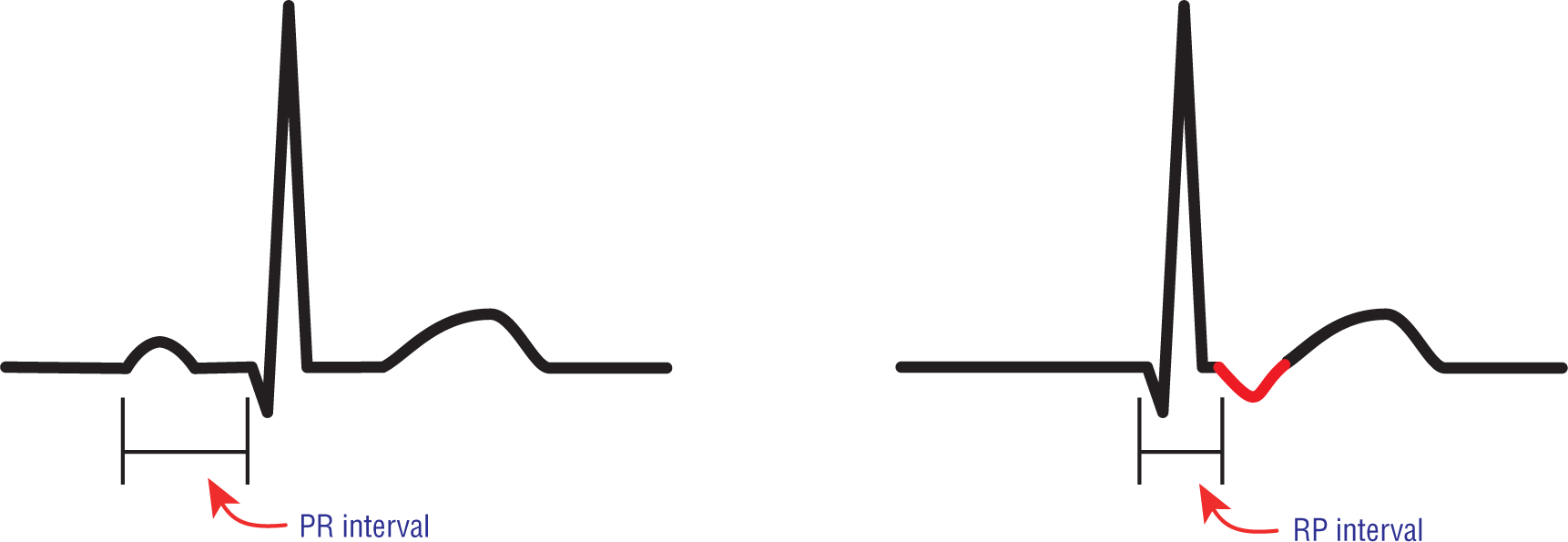
When the P wave is retrogradely spread to the atria and comes after the QRS complex, we speak of the RP interval instead of the PR interval (Figure 21-6). The RP interval is measured from the tip of the QRS complex to the beginning of the next conducted P wave.
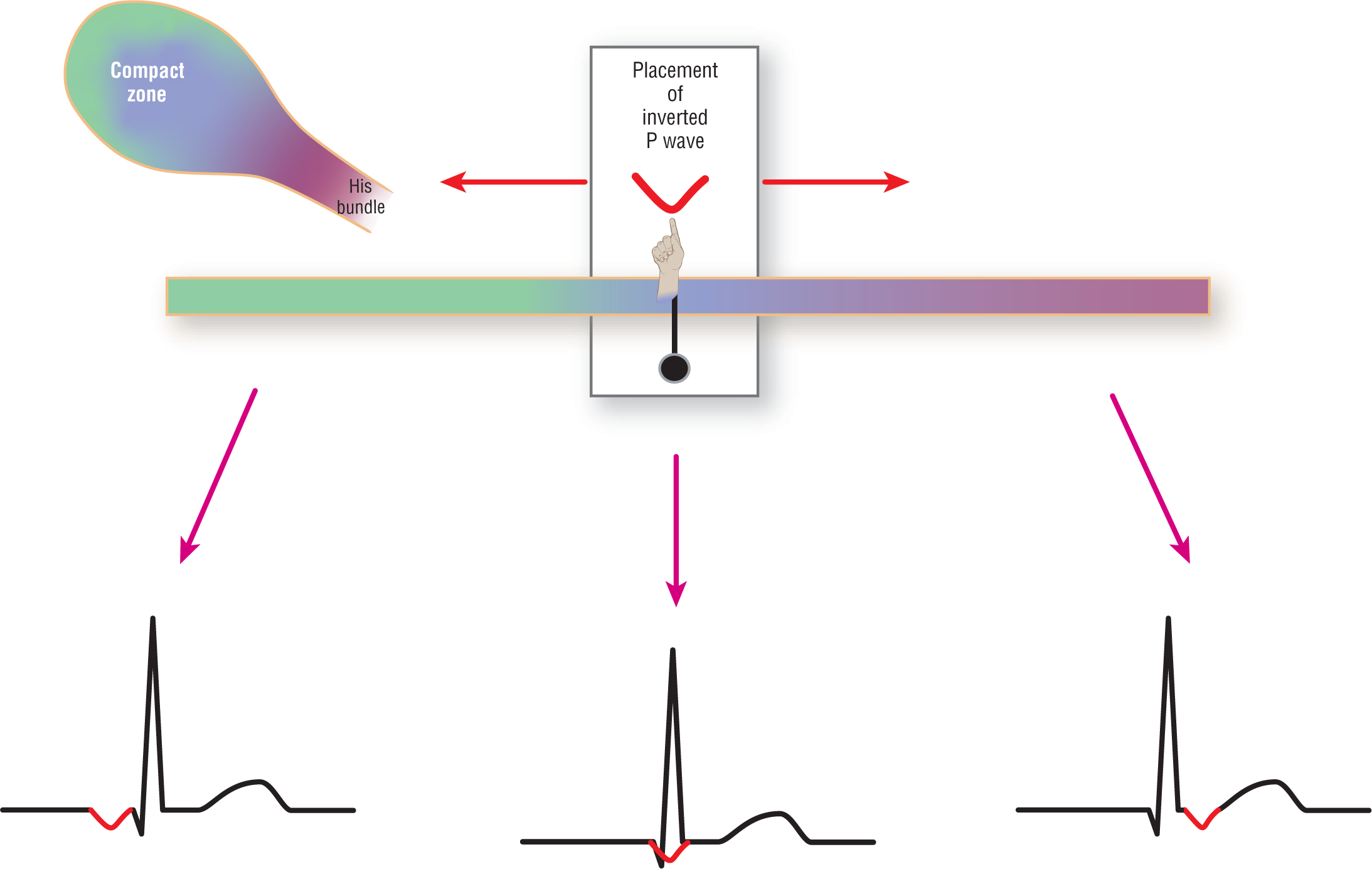
When you think about the appearance of the P wave in a junctional beat or rhythm, think of a continuum. This continuum is based on the exact location of the ectopic pacemaker and its relation to the rest of the AV junction, to the atria, and to the ventricles. Figure 21-7 is a graphic representing a clear slider with a P wave superimposed on it. As you move the slider along the color gradient representing the AV junction, you will see the placement of the P wave and its relationship to the QRS complex.
Figure 21-7 The relationship of the inverted P wave to the QRS complex is represented as a continuum. The P waves could be anything from before the QRS complex with a shortened PR interval, to buried within the QRS complex, to occurring slightly after the QRS complex.
Remember, when you see an inverted P wave in front of the QRS complex, take a look at the PR interval. If the PR interval is normal or prolonged, you should consider it an ectopic atrial complex. If the PR interval is short, you are probably dealing with a junctional complex. If you follow these rules, you will be correct in most cases. Exceptions do occur, and you should be aware of their possibilities to be completely correct.