From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
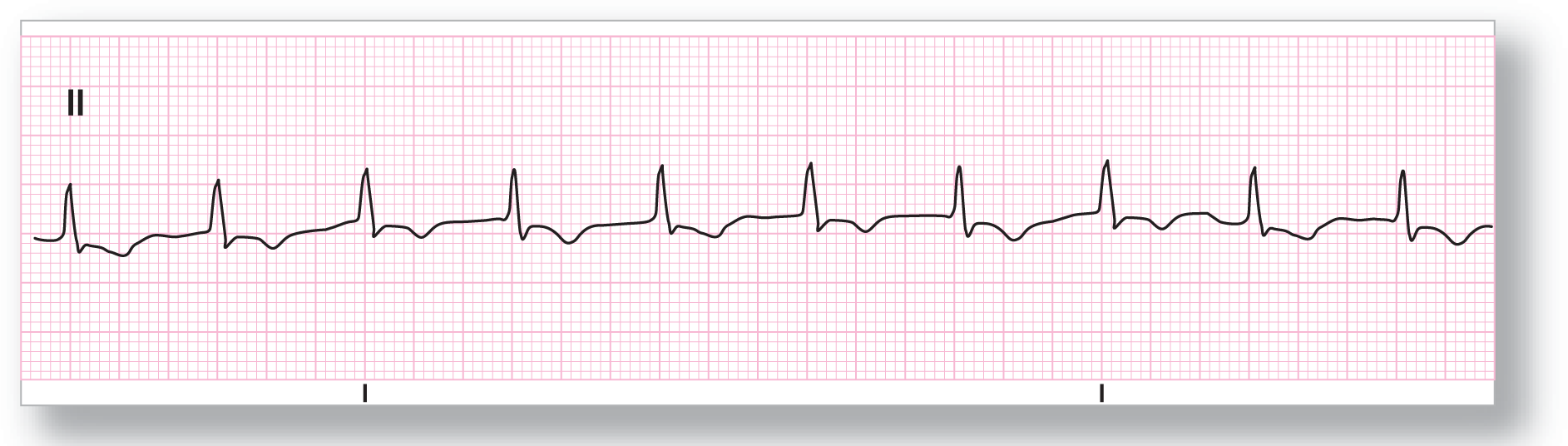
Rate: About 98 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Accelerated junctional |
Discussion:
ECG 24-1 shows an accelerated junctional rhythm at about 98 BPM. Since it is just under 100 BPM, we are not calling it junctional tachycardia. Note the absence of P waves, the regularity of the rhythm, and the narrow, supraventricular QRS complexes. The ST segments and symmetrically inverted T waves could easily represent ischemia or the reciprocal changes of a lateral AMI. Since accelerated junctional is associated with AMIs, clinical and electrocardiographic correlation would be a good idea.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 85 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wider than 0.12 sec. |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Accelerated junctional |
Discussion:
ECG 24-2 shows a wide-complex rhythm that is regular and has no apparent P waves. The width of the complex brings up a dilemma: Is this a ventricular rhythm or a junctional rhythm? Correlation with old strips and 12-lead ECGs showed a preexisting bundle branch block with the same morphology as the ones in the strip in lead II, making this a junctional rhythm. Note that in some cases, inverted P waves may widen the QRS complex slightly, leading to a misdiagnosis of a bundle branch block.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 78 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wider than 0.12 sec. |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Accelerated junctional |
Discussion:
ECG 24-3 is also an example of a wide-complex accelerated junctional rhythm. This patient also had a preexisting right bundle branch block, which accounted for the wide complexes on the ECG. Once again, comparison with old ECGs, was crucial to determine the diagnosis and to evaluate if the small q wave and the R wave were not buried P waves. Never discount the usefulness of old ECGs, and always try to save a strip for posterity. You never know when you will need an old one to compare.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present (pseudo-S wave) Morphology: Pseudo-S wave Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Junctional tachycardia |
Discussion:
ECG 24-4 is the first example of junctional tachycardia that we have shown you. (The rate of 135 BPM is right at the borderline between junctional tachycardia and AV nodal reentry tachycardia, and either one is technically correct.) Are there any P waves on this strip? The answer is yes! The blue arrow is pointing to an inverted P wave that is occurring immediately after the QRS. This is a common finding in junctional tachycardias, known as the pseudo-S wave. It is called a pseudo-S because it is not a true S wave but is due to the inverted P wave. Comparing the morphologies with an old strip will clarify the question of S wave or pseudo-S wave.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present (pseudo-S wave) Morphology: Pseudo-S wave Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Junctional tachycardia |
Discussion:
ECG 24-5 shows a junctional tachycardia at about 135 BPM. (The rate of 135 BPM is right at the borderline between junctional tachycardia and AV nodal reentry tachycardia, and either one is technically correct.) The QRS complexes are narrow and obviously supraventricular in origin. There are no obvious P waves before the QRS complexes. Comparison with old strips confirmed the presence of a pseudo-S wave in lead II, which was not there on a strip with normal sinus rhythm. The pseudo-S wave was due to an inverted, retrogradely conducted P wave.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present (pseudo-R’ wave) Morphology: Pseudo-R’ wave Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Junctional tachycardia |
Discussion:
ECG 24-6 was taken on the same patient as in ECG 24-5, but the lead was switched to V1. In this example, we see a pseudo-R’ wave clearly. It is called a pseudo-R’ wave because there is a small “actual” or “true” R wave present at the start of the complex. Remember, the first positive complex after an S wave is known as the R’ wave.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Junctional tachycardia |
Discussion:
ECG 24-7 is another example of a junctional tachycardia at about 135 BPM. (The rate of 135 BPM is right at the borderline between junctional tachycardia and AV nodal reentry tachycardia, and either one is technically correct.) This strip has no obvious P waves and narrow, supraventricular QRS complexes.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 112 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Junctional tachycardia |
Discussion:
ECG 24-8 is a junctional tachycardia at about 112 BPM. The QRS complexes are narrow and supraventricular in appearance. There may be a slight indentation at the end of the QRS complex, which could be indicative of a retrogradely conducted, inverted P wave, but this cannot be completely diagnosed from this strip. Comparison with an old strip will help identify the morphologic appearance of the complexes and any possible buried waves.