From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
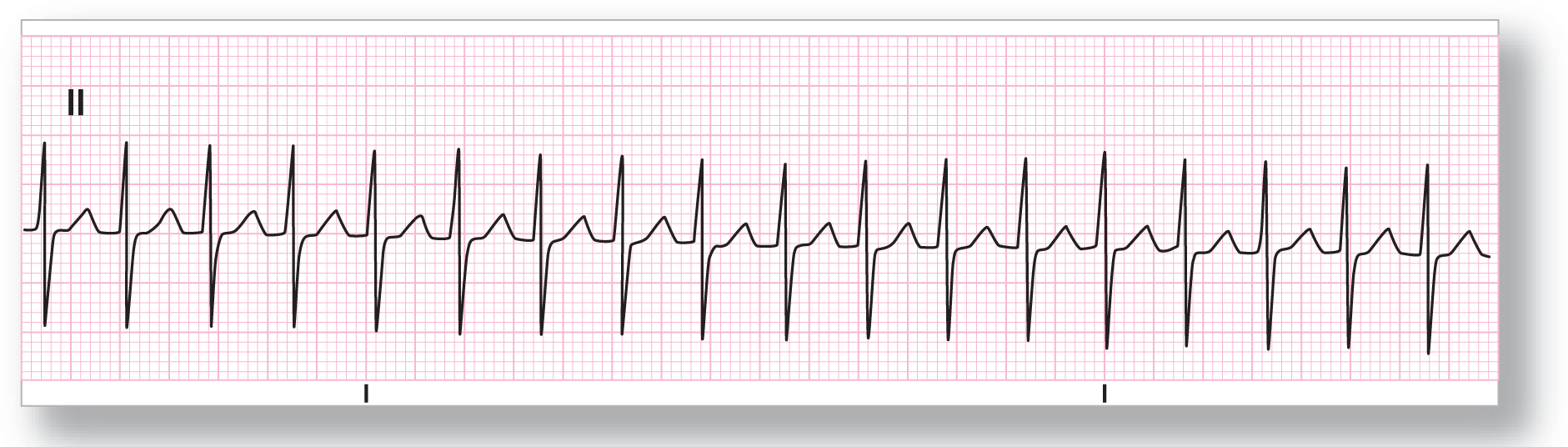
Rate: About 180 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: AVNRT |
Discussion:
ECG 25-1 shows a narrow-complex tachycardia that is very regular and has no visible P waves anywhere on the strip. There is no evidence of any pseudo-S pattern on the strip. A narrow-complex tachycardia at this rate is AVNRT until proven otherwise.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
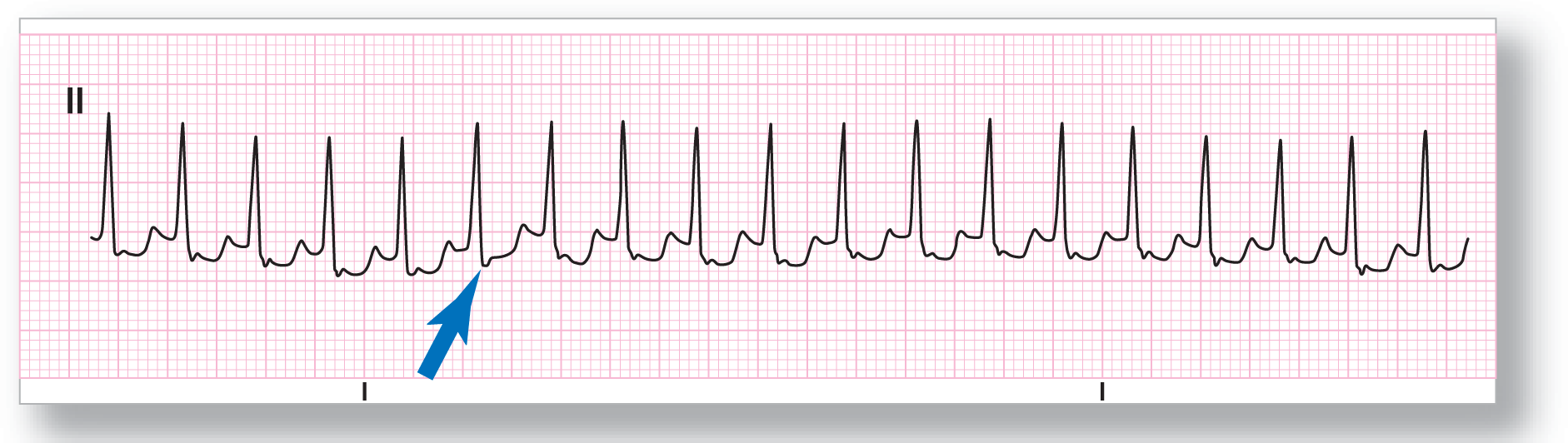
Rate: About 200 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Pseudo-S Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: AVNRT |
Discussion:
ECG 25-2 shows a very rapid rhythm at about 200 BPM. The QRS complexes are narrow and there are no discernible P wave. There is, however, a small s wave noted at the end of the QRS complex, which was not there on old ECGs. This is a pseudo-S wave (blue arrow) and is representative of an inverted P wave. The ST segment is depressed, as is common in rapid tachycardias. This could be due to relative endocardial ischemia due to the rapid rate, but the cause is usually unclear.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
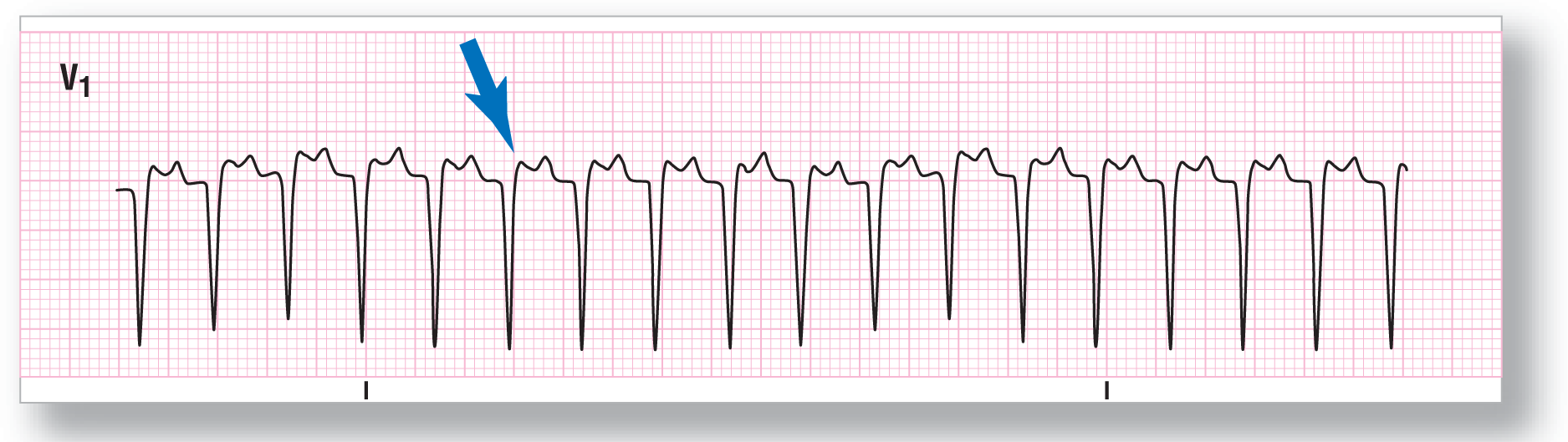
Rate: About 200 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Pseudo-R’ Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: AVNRT |
Discussion:
ECG 25-3 was obtained from the same patient as in ECG 25-2, except that this is lead V1. The extra lead was obtained in order to evaluate the patient for a pseudo-R’ wave, which is present, at the end of the QS wave (blue arrow). Electrical alternans is obvious on the strip with an undulating pattern of longer and shorter QS waves. This is very common in very rapid tachycardias and does not represent any secondary pathologic processes, such as pericardial effusion. Clinical correlation is indicated, however.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
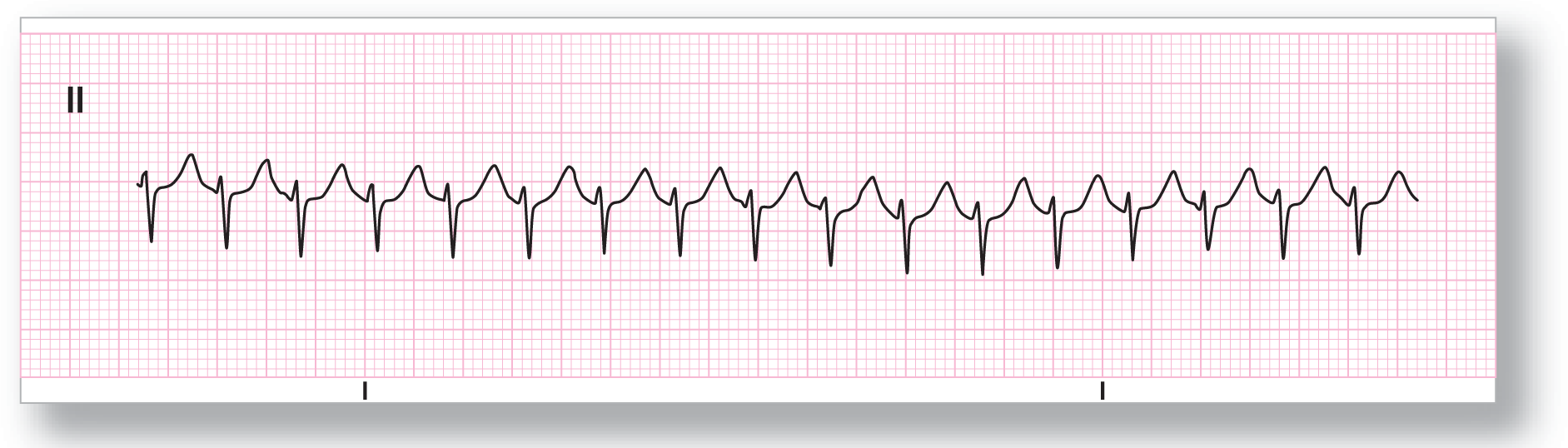
Rate: About 195 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: AVNRT |
Discussion:
ECG 25-4 shows a rapid, narrow-complex tachycardia with negative QRS complexes in lead II. The negative complexes are composed of deep S waves, making any pseudo-s pattern difficult, if not impossible, to visualize. There is some undulation in QRS size, which is compatible with most rapid tachycardias.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 195 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Pseudo-R’ Morphology: Not clear Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: AVNRT |
Discussion:
ECG 25-5 is, once again, a strip of the same patient, but in lead V1. Here the pseudo-R’ pattern is more evident (blue arrow). This finding clinches the diagnosis of AVNRT. Please note that in all of these examples, the regularity of the rhythm is uncanny. This is due to the reentry mechanism, which causes clockwise precision in the regularity of the rhythm.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 200 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: AVNRT |
Discussion:
ECG 25-6 shows a narrow-complex tachycardia at about 200 BPM. The QRS complexes are negatively oriented and there appears to be a small deflection at the end of the S wave, which could indicate a pseudo-S pattern. There is some variation in the height of the R wave, which is compatible with electrical alternans seen in many rapid tachycardias. AVNRT is the diagnosis of this rhythm abnormality.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 190 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: See discussion below Morphology: See discussion below Axis: See discussion below |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: See discussion below |
Rhythm: AVNRT |
Discussion:
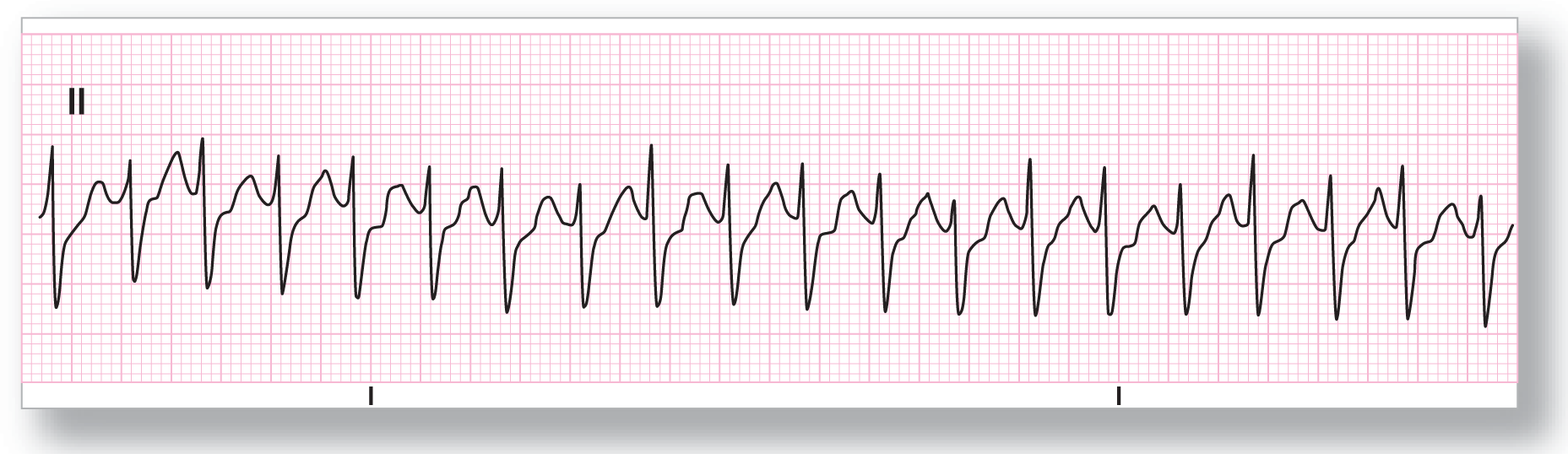
ECG 25-7 is a rapid tachycardia at about 190 BPM with a narrow complex by initial appearance. The problem is that there is ST-segment depression and a possible pseudo-S pattern or slurred S-wave pattern (typically seen in bundle branch block). The narrowness of the initial R wave makes the diagnosis of ventricular tachycardia less likely. Comparing this strip to an old ECG or to one taken when the rhythm is broken is critical in deciding the final diagnosis. If the patient is unstable, he or she should be cardioverted or defibrillated emergently. Treatment with vagal maneuvers or adenosine initially would be appropriate if the patient were stable.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 185 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: See discussion below Morphology: See discussion below Axis: See discussion below |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: AVNRT |
Discussion:
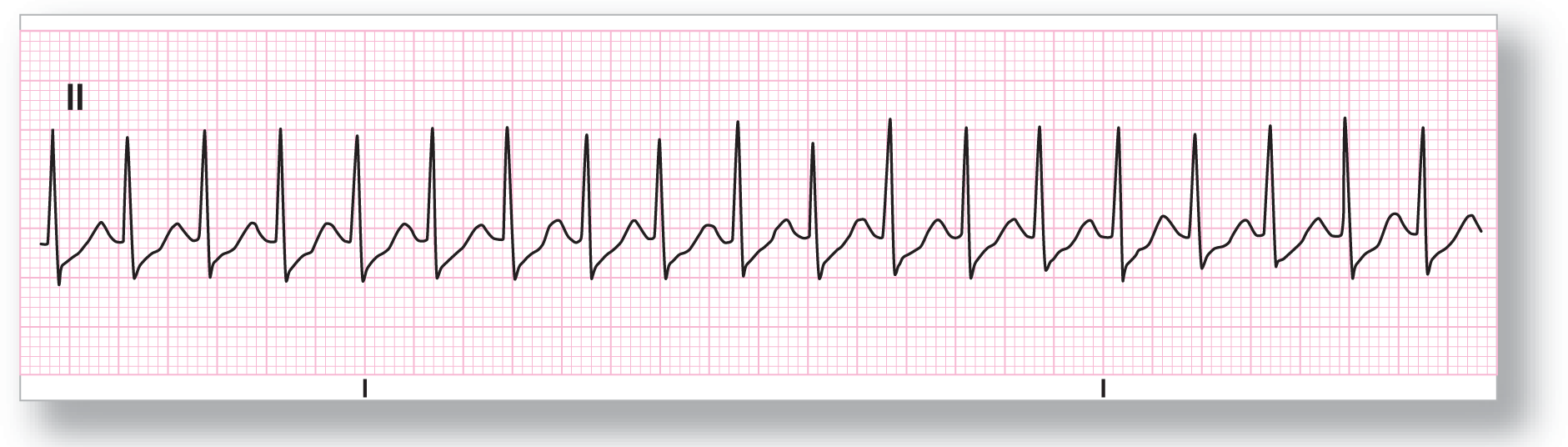
ECG 25-8 also has ST-segment depression, which could be from the tachycardia or ischemia (relative or endocardial). Clinical correlation is indicated to evaluate this finding. There is a small s wave, which could be an actual part of the QRS complex or could be due to a pseudo-s wave pattern. Comparison with an old ECG would be helpful. The variation in QRS size is due to electrical alternans and is probably due to the tachycardia.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 210 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: AVNRT |
Discussion:
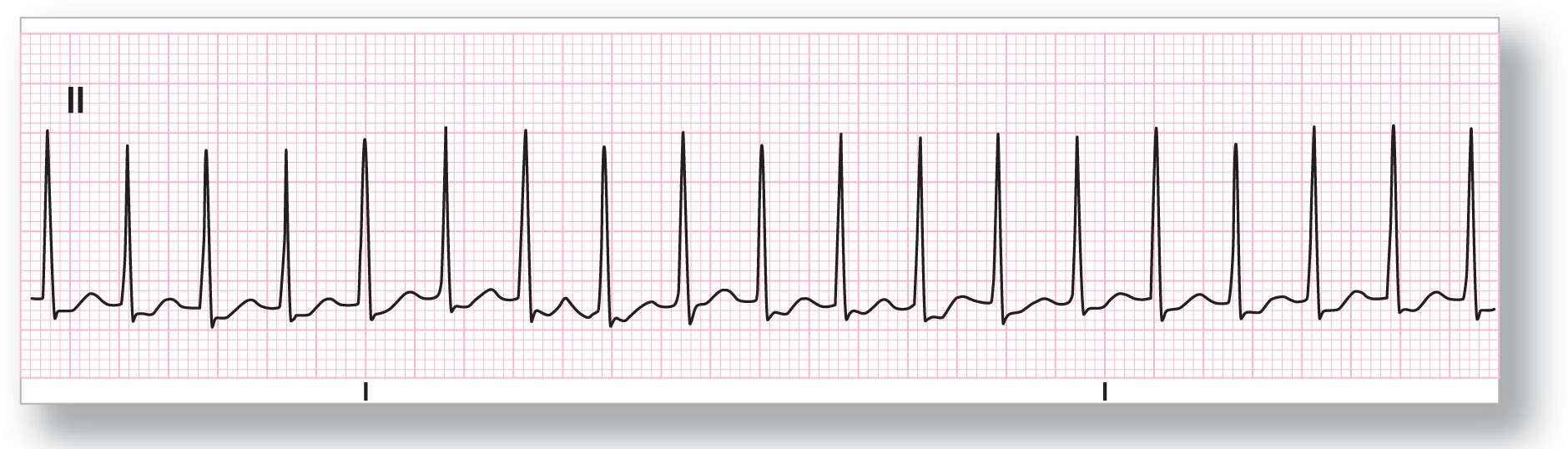
ECG 25-9 shows a rapid, narrow-complex tachycardia at about 210 BPM. The QRS complexes are pretty clearly defined and the ST segments are depressed and have a scooped-out appearance. This pattern of ST depression may be due to the tachycardia, ischemia, or digitalis effect. Clinical correlation and comparison to an old ECG are critical in arriving at the final diagnosis. Remember, however, treat the tachycardia first, and then worry about the final diagnosis. AVNRT should be the first thing on your differential diagnosis list.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
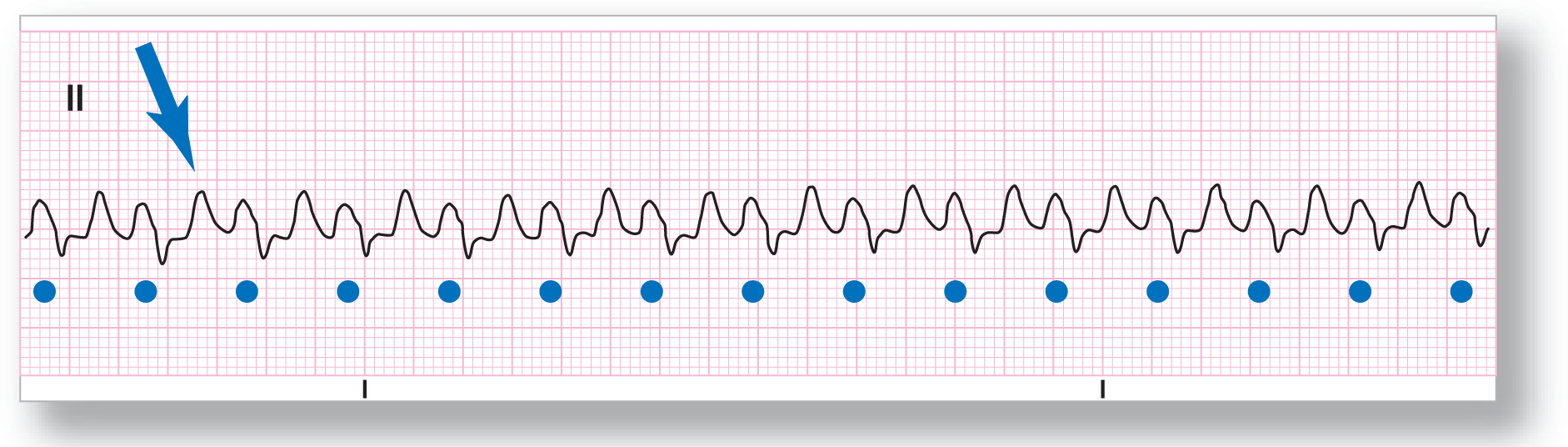
Rate: About 145 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: AVNRT |
Discussion:
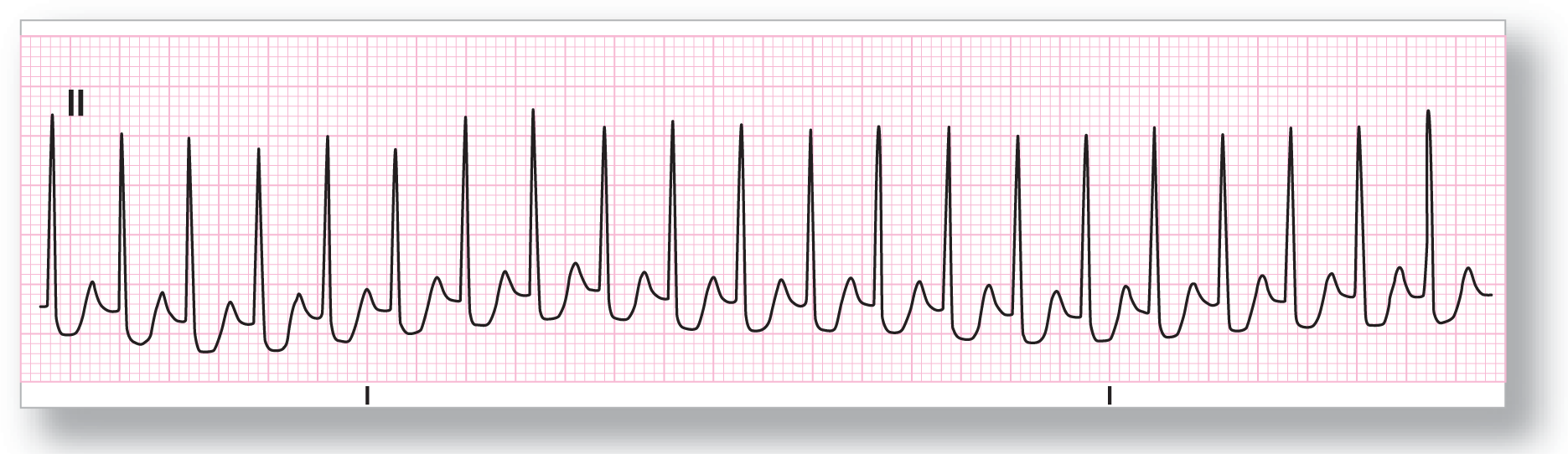
ECG 25-10 is a real diagnostic dilemma. This is a wide-complex tachycardia that is regular and has no observable P waves. This could very easily be ventricular tachycardia and the patient should be treated for this possibility until proven otherwise. Differential diagnosis includes junctional tachycardia, AVNRT, AV reentry tachycardia, and ventricular tachycardia. Comparison with an old ECG showed a preexisting bundle branch block with similar morphology, clinching the diagnosis as AVNRT. The QRS complexes are labeled with the blue dots, and the T wave is labeled with the blue arrow.