Under normal circumstances, an atrial impulse will hit the AV node and the accessory pathway fairly close together, temporally speaking (Figure 26-1). The net result of this atrial depolarization wave is that the impulse begins to move through both the AV node and the accessory pathway almost simultaneously. The AV node slows conduction briefly by applying the physiologic block. The impulse traveling through the accessory pathway, however, is unimpeded and begins to depolarize the ventricles immediately. The impulse traveling through the accessory pathway, however, moves very slowly through the ventricular myocardium because it has to travel by direct cell-to-cell transmission. Electrocardiographically, this very slow conduction through the ventricles leads to a wide, bizarre appearance at the start of the QRS complex. That wide, bizarre area of the QRS is called a delta wave (Figure 26-2).
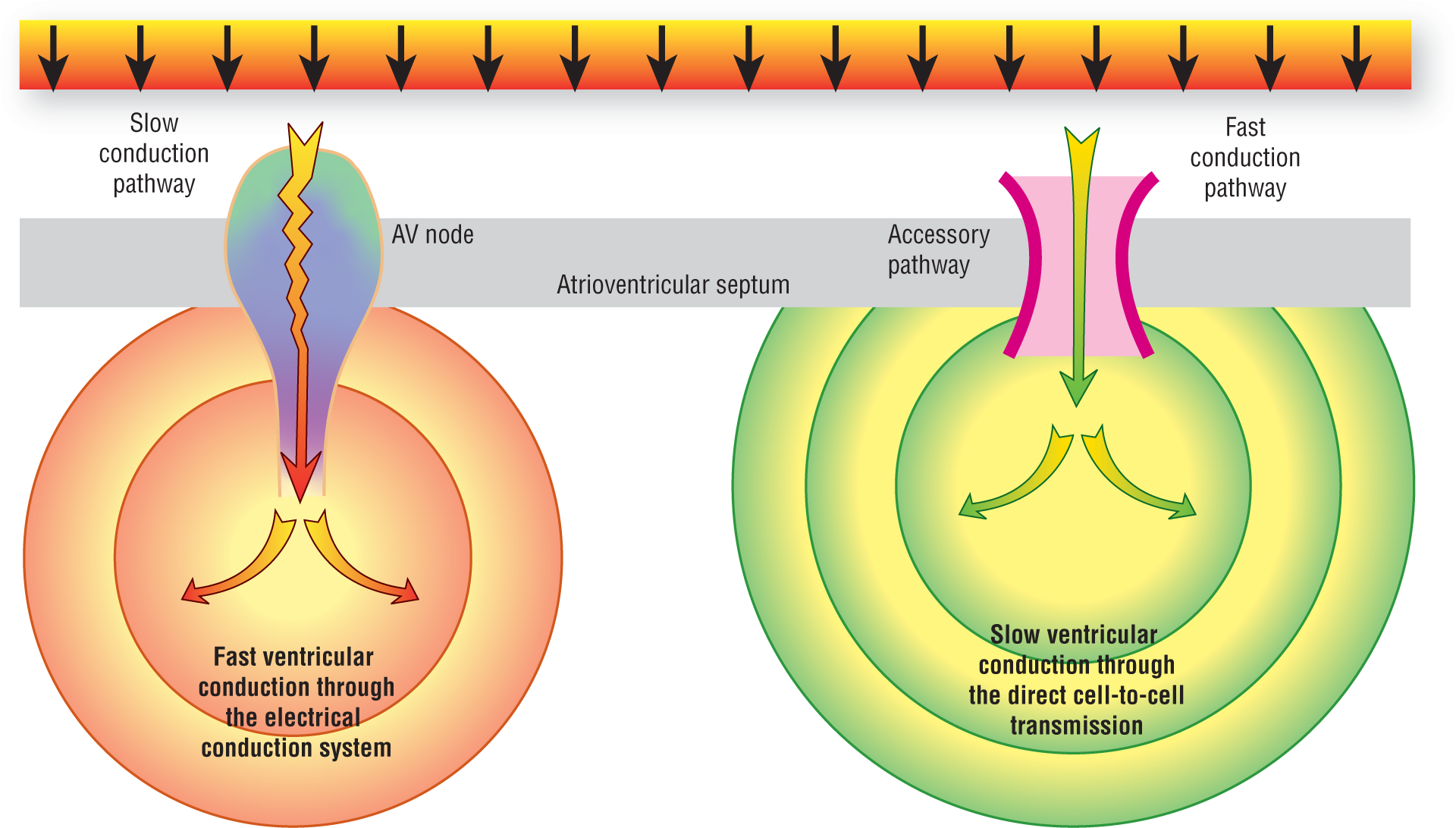
Figure 26-1 When an accessory pathway is present, the impulse has two ways of getting to the ventricles. The usual way of using the AV node is slower because of the presence of the physiologic block. The accessory pathway is not subject to the physiologic block and transmits the impulse instantaneously. Therefore, the ventricular myocardium around the accessory pathway will begin to depolarize quicker but ventricular activation will have to occur by direct cell-to-cell transmission.
Once the physiologic block is completed in the AV node, the impulse is quickly spread throughout the majority of the ventricular myocardium via the electrical conduction system. Since transmission through the normal conduction system is much faster than direct cell-to-cell transmission, the normally conducted impulse quickly overtakes and surrounds the impulse originating in the accessory pathway.
The two wavefronts eventually meet and cancel each other out. The large amount of myocardium depolarized by the normal wave causes a sharp stop to the delta wave. Electrocardiographically, this is represented as the end of the delta wave and the formation of a normal appearing mid- and terminal portion of the QRS complex. Note, however, that the QRS complex is still wide because the duration of the delta wave has to be added to the total QRS interval. As we can see from Figure 26-2, the added width of the QRS interval does come at the expense of the PR interval.
Electrocardiographically, the net result of this dual conduction is a short PR interval (because of the immediate transmission of the impulse through the accessory pathway), a delta wave, and a wide QRS complex (greater than 0.12 seconds). To round off this discussion, transmission through accessory pathways also alters the ST segment and the T wave by altering the repolarization pattern of the ventricle. This electrocardiographic pattern is presently named after the investigators who discovered it and is known as Wolff-Parkinson-White (WPW) pattern.
An additional clinical point: If a patient with the WPW pattern also has symptoms or any clinical manifestations of rapid tachycardias, then the correct terminology for this clinical syndrome is Wolff-Parkinson-White syndrome. The word “syndrome” is used to focus on the pathologic inclusion of life-threatening arrhythmias into the picture.