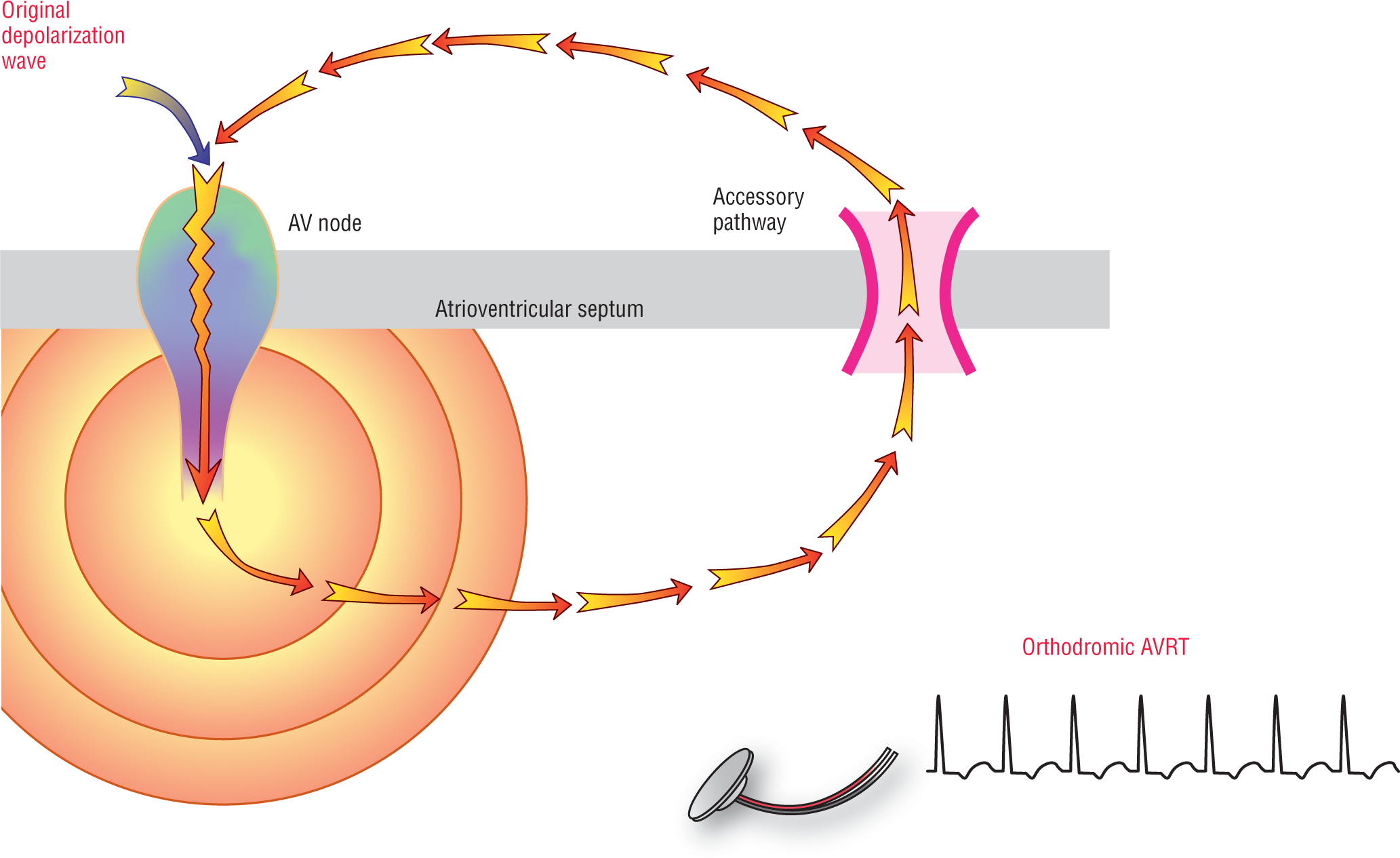
Orthodromic AVRT is created by a macroreentry circuit in which the impulse travels down through the AV node and returns retrogradely through the accessory pathway to the atria. Since the impulse travels down the AV node and depolarizes the ventricles through the normal conduction system, the tachycardia that is produced by this circuit is narrow complex (Figure 26-4).
Figure 26-4 Orthodromic AVRT. In this form of AVRT, the impulse proceeds down to the ventricles via the AV node and the normal electrical conduction system. The net result is that the tachycardia is “controlled” by the AV node and the QRS complexes are narrow.
Just as in AV nodal reentry tachycardia (AVNRT), the initiating impulse is usually a premature atrial contraction (PAC). In AVRT, however, the initiating impulse can also be a premature ventricular contraction (PVC). The PVC can cause a transient block in the His-AV node area that does not allow the spread retrogradely through the AV node. However, the accessory pathway would not be blocked and would conduct the impulse retrogradely to the atria to trigger the reentry loop.
Orthodromic AVRT has one major advantage over its evil twin, antidromic AVRT—the AV node still has tremendous influence over the rates and conduction speeds. The AV node exerts its influence because it still has a functional physiologic block and responds to medications as it would under normal circumstances. This means that the rates of the tachycardia are more stable and are usually in the range of 150 to 250 beats per minute (BPM; although variability does occur) and are reasonably tolerated by most patients. The additional fact that the ventricles are contracting smoothly and synchronously because of the use of the electrical conduction system adds to the hemodynamic stability in orthodromic vs. antidromic AVRT.
The sympathetic system exerts control over the rate by altering the conduction speed through the AV node. The higher the sympathetic tone, the higher the rate. Likewise, pharmacologic agents that slow conduction through the AV node will also control or terminate the arrhythmia.
The P Wave and AVRT
A very important diagnostic clue to decide whether a rapid tachycardic rhythm is either AVNRT or AVRT is the location of the inverted P wave. As we saw in Chapter 25, AV Nodal Reentry Tachycardia, the inverted P wave in AVNRT is either immediately before, during, or immediately after the QRS complex. In AVRT, the inverted P wave is usually pretty far away from the QRS complex. Can you think of why this would be?
Additional Information
Concealed Conduction Pathways
Many times the delta wave is not formed or is so small that it is almost imperceptible. This typically occurs when the atrial depolarization wave hits the AV node before it hits the accessory pathway. The normally conducted ventricular depolarization wave will then cancel out the one traveling through the accessory pathway very quickly, before it ever becomes electrocardiographically significant. This type of conduction is, therefore, electrocardiographically silent and there is no way (short of electrophysiologic testing) to identify the presence of these silent conduction pathways. The term used to describe this silent or hidden potential conduction is concealed conduction pathway. This type of conduction is the most common presentation for patients with accessory pathways.
Concealed conduction pathway emphasizes the lack of electrocardiographic findings in these patients under normal circumstances. We stress the words “under normal circumstances” because the pathologic process is still there and it can surface instantaneously, creating a life-threatening tachyarrhythmia by forming a reentrant circuit. Finally, some patients will intermittently move back and forth between the WPW pattern and concealed conduction on the same rhythm strip.
Clinically, patients with concealed conduction pathways are commonly encountered. A high index of suspicion is needed to correctly identify these patients and assure proper acute and definitive treatment, because their resting ECGs are completely normal. If you have any patient with a tachycardia that resembles AVRT, referral to a cardiologist or an electrophysiologist is critical.
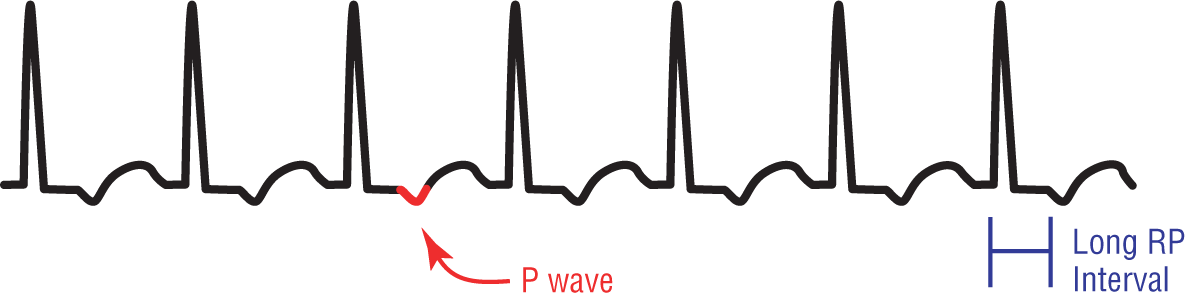
As we have seen throughout this text, if a wave has to travel farther, it will be longer. In patients with accessory pathways, the distance between the two pathways (the AV node and the accessory pathway) is relatively great in most cases. The time that the depolarization wave spends traversing those distances significantly lengthens the RP interval.
We can use the long RP interval found in orthodromic AVRT to help us in our differential diagnoses of narrow-complex tachycardias (Figure 26-5). In other words, if you have a narrow-complex tachycardia and you are trying to decide between AVRT and AVNRT, the location of the inverted P wave could be very helpful.
Figure 26-5 The inverted P wave is found at a longer RP interval than that found in AVNRT. This is because the macroreentry loop has to travel longer distances between the two pathways. Longer distance means longer intervals. This fact will be very helpful in evaluating the differential diagnoses of the narrow-complex tachycardias.
Orthodromic AVRT is the most common reentrant tachycardia found in WPW syndrome. It is found to be the mechanism involved in about 95% of the reentrant tachycardias found in WPW and is very commonly seen in patients with concealed pathways.
Wide-complex orthodromic AVRT can sometimes be seen in cases of aberrancy, electrolyte abnormalities, or preexisting bundle branch blocks. These cases are nearly impossible to distinguish from antidromic AVRT (as we shall see shortly) and should be treated with extreme caution, both in diagnosis and treatment strategies.
It is important to note that the delta wave is not visible during orthodromic AVRT because there is no fusion of impulse from the two pathways. Instead, the impulse travels in a sequential macroreentrant loop between the two pathways. Electrical alternans is frequently seen in these patients, just as it is in most tachycardias. ST-segment depression is also commonly seen, even in young, healthy individuals.