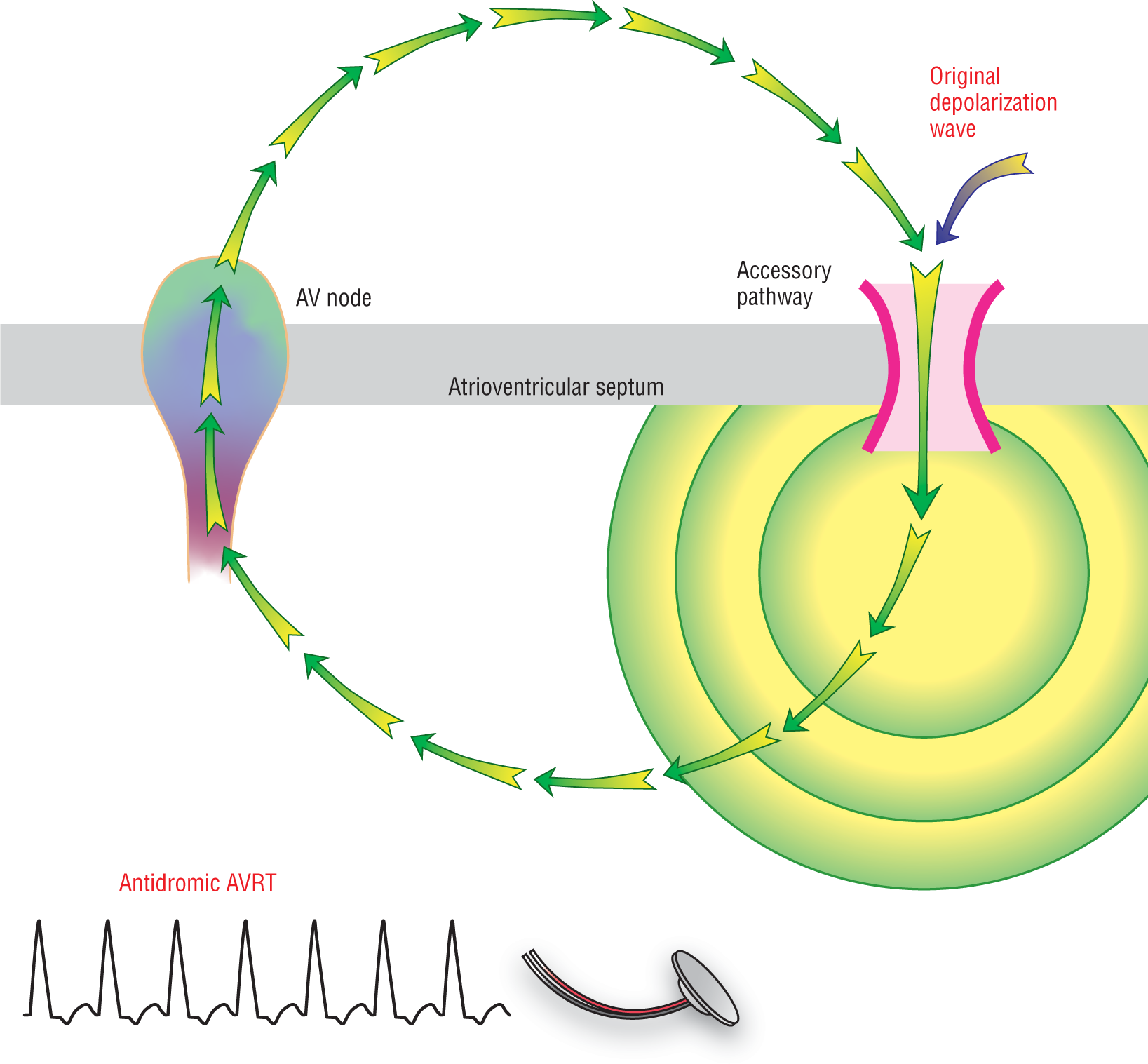
Antidromic AVRT is created by a macroreentry circuit in which the impulse first travels down the accessory pathway to stimulate the ventricles (Figure 26-6). The impulse then moves across the ventricles by direct cell-to-cell transmission of the impulse, giving rise to a wide, bizarre QRS complex. Once the impulse reaches the area of the AV junction, it travels retrogradely through the AV node to restimulate the atria. When that impulse once again reaches the accessory pathway, the circuit will restart and continue in a looping manner giving rise to a wide-complex tachycardia.
Figure 26-6 Antidromic AVRT. The original impulse travels down the accessory pathway. A reentry circuit is formed when the ventricular depolarization wave, being spread by direct cell-to-cell contact, reaches the AV node. It then moves retrogradely up through the AV node to restimulate the atria. The circuit is completed when the retrogradely conducted atrial impulse reaches the accessory pathway, once again restarting the circuit. The resulting QRS complexes are wide and bizarre due to the slow ventricular conduction. Also note the absence of AV nodal control over the rate. The RP interval remains long in this form of AVRT.
The circuit can be initiated by either a PAC or a PVC and is usually associated with rates between 150 and 250 BPM (but can be as high as 360+ BPM). Note, however, that there is no AV nodal conduction control over the rate in antidromic AVRT. There is no physiologic block to help keep the rate to a ceiling of just 250 BPM. For example, what happens when the patient has an underlying atrial flutter rate at 300 BPM? What would the ventricular rate be? If you guessed 300 BPM, you are correct. Now, can you guess what happens if the patient is in atrial fibrillation? The patient will be at very, very rapid ventricular rates and could very easily enter ventricular fibrillation. As you can imagine, antidromic AVRT is a very dangerous rhythm.
This brings us to a very important clinical discussion. Pharmacologic agents that slow conduction through the AV node but do not affect the accessory pathway are very dangerous in patients with accessory pathways. Administration of these drugs will cause the atrial impulses to travel preferentially down the accessory pathway and avoid the physiologic control exerted by the AV node. This is the main reason why certain calcium channel blockers, parasympatheticomimetic agents, beta-blockers, digitalis, vagal maneuvers, and even adenosine can be so dangerous in patients with WPW. In addition, digitalis, calcium channel blockers (especially verapamil), and adenosine can shorten the refractory period of the accessory tract and help increase conduction down the accessory pathway even farther. In a patient with WPW or a concealed pathway, these agents could turn a fairly stable arrhythmia into a very highly unstable disaster.
Remember, it is the ventricular rate and contractility that is one of the major components of the cardiac output and hemodynamic stability. A patient in atrial flutter or atrial fibrillation who is treated with the agents outlined earlier could easily go into a very rapid ventricular tachycardia, ventricular flutter, or ventricular fibrillation and die if he or she has a hidden accessory pathway. Be careful of wide-complex tachycardias! Always treat them as if they are ventricular tachycardia until proven otherwise; approach them very, very carefully and remember that they could also represent an antidromic AVRT.
Additional Information
Wide-Complex Tachycardias
The differential diagnosis of wide-complex tachycardias includes some very dangerous rhythms, including ventricular tachycardia, ventricular flutter, torsade de pointes, and antidromic AVRT. We shall be studying these in detail in the next section. It also includes the rhythms we have seen up to this point in the text when they are associated with preexisting bundle branch block, electrolyte abnormalities, or aberrancy. When you are approaching a patient with a wide-complex tachycardia, you should always assume the worst-case scenario. You should never assume an aberrant presentation of a more benign rhythm because the criteria that we use in surface electrocardiography are not always conclusive.
If you see an irregularly irregular rapid wide-complex tachycardia at rates over 250 BPM, it is usually going to be atrial fibrillation in a patient with an accessory pathway until proven otherwise. Ventricular tachycardia is usually regular after the first few seconds after the onset. Be careful of what drugs you give WPW patients! In a hemodynamic emergency, remember that electrical defibrillation or cardioversion is always a possibility. A complete discussion on the treatment of WPW is beyond the scope of this text.
Here are two major clinical pearls:
If the ventricular rate exceeds 200 BPM in atrial fibrillation, it is probably an atrial fibrillation in a patient with an accessory pathway or WPW syndrome.
In general, as the ventricular rate exceeds 250 BPM, the possibility that you are dealing with an accessory pathway increases.
ARRHYTHMIA RECOGNITION
AV Reentry Tachycardia
Rate:
150 to 250 BPM (can be higher in antidromic AVRT)
Regularity:
Regular
P wave:
Morphology:
Upright in II, III, and aVF:
Inverted
Different
No
P:QRS ratio:
1:1 or absent
PR interval:
None (RP interval is prolonged)
QRS width:
Normal in orthodromic AVRT
Wide in antidromic AVRT
Grouping:
None
Dropped beats:
None
DIFFERENTIAL DIAGNOSIS
AV Reentry Tachycardia
Only seen in patients with accessory pathways, either concealed conduction or WPW.