Any patient with significant hemodynamic compromise due a pathologic tachyarrhythmia (one that does not include sinus tachycardia), requires immediate cardioversion or defibrillation to reestablish a normal sinus rhythm. Cardioversion and defibrillation both work instantaneously by administering a small electric current that depolarizes all of the myocardial cells instantaneously. This acts like a computer restart and allows the normal cardiac pacemakers to “reboot” and begin to function normally (see the section on Pacemaker Function in Chapter 1, Anatomy and Basic Physiology). The objective is emergent ventricular rate control and the reestablishment of normal cardiac function and synchronized contractility to maximize cardiac output.
In a narrow-complex tachycardia, the heart rate can be anywhere from 100 BPM to over 360 BPM. Luckily, most SVTs occur in the lower to middle ranges of that rate spectrum. As you can imagine, patients can tolerate the lower end of this rate spectrum much better than they can tolerate the rates at the upper end. There are many reasons for the hemodynamic compromise that occurs in a tachycardia, but the greatest hemodynamic effect occurs because of alterations in the cardiac output.
If you remember from Chapter 1, Anatomy and Basic Physiology, one of the main determinants of blood pressure is the cardiac output. Cardiac output, in turn, is determined by the stroke volume and the heart rate. A rapid tachycardia will affect both the stroke volume and the heart rate negatively. In addition to its direct effects, the heart rate will cause additional problems in ventricular filling, altering the stroke volume even further.
Heart Rate and Hemodynamics
Rapid rates affect the hemodynamic status of the heart in various ways. The most important ones include:
Relative ischemia due to increased myocardial oxygen demand
Decreasing ventricular filling times and decreasing end-diastolic volume
Decreasing atrial kick and ventricular overfilling
Relative Ischemia Due to Increased Myocardial Oxygen Demand
One way that an increase in heart rate causes hemodynamic compromise is by causing an increase in myocardial oxygen demand of the heart muscle itself. This increased oxygen demand, in turn, can lead to a relative myocardial ischemia. The term “relative” here refers to the fact that it is not ischemia due to atherosclerotic heart disease, but rather an imbalance of the amount of oxygen being delivered to the tissue compared to the amount of oxygen that the tissue needs. In other words, the demand for oxygen exceeds the supply of oxygen. The result is that the tissue is ischemic and does not function at its maximum (or even normal) potential.
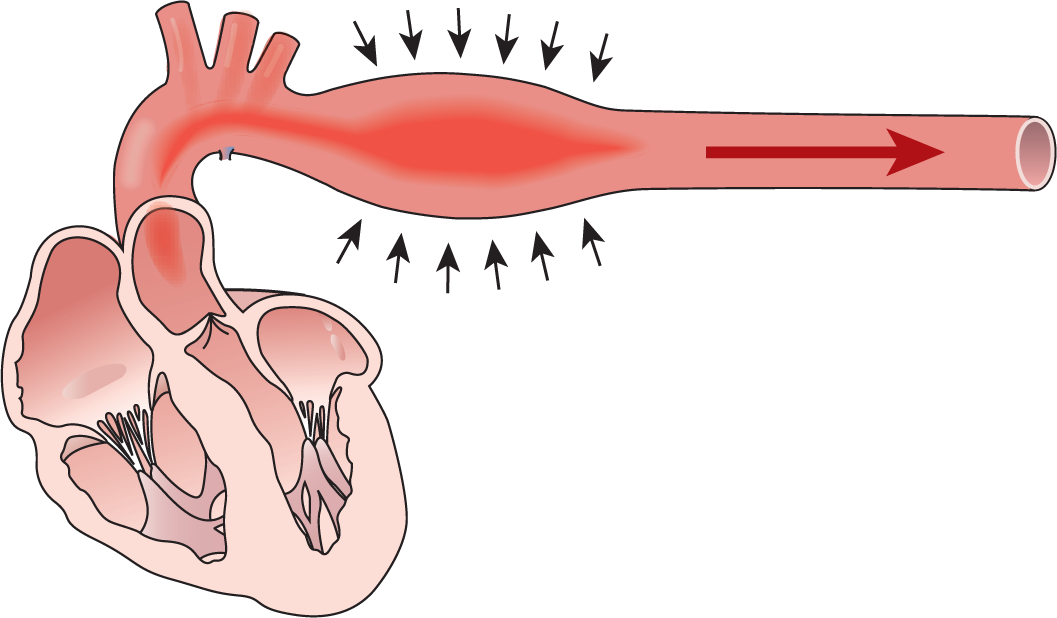
Ischemic muscle does not contract appropriately. This decrease in the contractility of the heart leads to a decrease in the amount of blood ejected by the heart into the aorta. Remember from Chapter 1, Anatomy and Basic Physiology, that it is the ejection fraction of the heart (the amount of blood pumped out with each contraction) that expands the aorta. The elastic recoil of the aorta trying to return to its resting state provides enough constant pressure to push the blood forward throughout the rest of the circulatory system (Figure 27-22). As you can imagine, if the amount of blood ejected is lower, the aorta will not distend as much, and the pressure exerted by the aorta will be lessened. Less pressure equals less perfusion throughout the body tissues and leads to a shock state.
Figure 27-22 Imagine that the bolus of blood that shoots out of the heart is the red area in this figure. Notice how the aorta is distended outward by the additional bolus. As the bolus begins to mix with the rest of the blood, the built-up pressure on the arterial walls is still there and pushing the walls inward toward the lumen. This happens because the elastic walls want to return to their resting state of relaxation. This pressure causes the blood to move forward smoothly and continuously. The process is repeated over and over with each cardiac contraction.
In general, the faster the tachycardia, the greater the oxygen demand of the myocardial cells. That is why patients tend to tolerate the slower rates along the SVT spectrum without much difficulty. The faster rates, however, can lead to catastrophic hemodynamic compromise and may even lead to death.
Decreasing Ventricular Filling Times and Decreasing End-Diastolic Volume
The heart rate also affects the cardiac output by affecting the stroke volume of the patient. Normally, the ventricles fill during the resting phase of the heart (diastole). As we saw in Chapter 1, Anatomy and Basic Physiology, ventricular filling occurs both passively and actively. It is in fact during the passive filling phase that most of the blood enters the heart, and passive filling occurs during diastole (Figure 27-23). The active phase of filling also occurs during diastole and is caused by atrial contraction. (Note that since most SVTs have abnormalities in the atrial rate, this atrial kick is also greatly altered in many SVTs.)
Figure 27-23 Normal ventricular filling.
This Figure shows the heart in late systole. The atria are full but the ventricles are empty.
In early diastole, the AV valves open, allowing a large amount of blood to rush into the ventricles. This is the rapid filling phase of diastole.
In mid-diastole, the ventricles are full. Notice that the ventricular walls, however, are not distended in any way.
The atrial contraction allows an extra amount of blood to enter the ventricles, causing them to stretch and overfill. The slight stretch in the ventricular muscle caused by the atrial kick will maximize stroke volume and cardiac output.
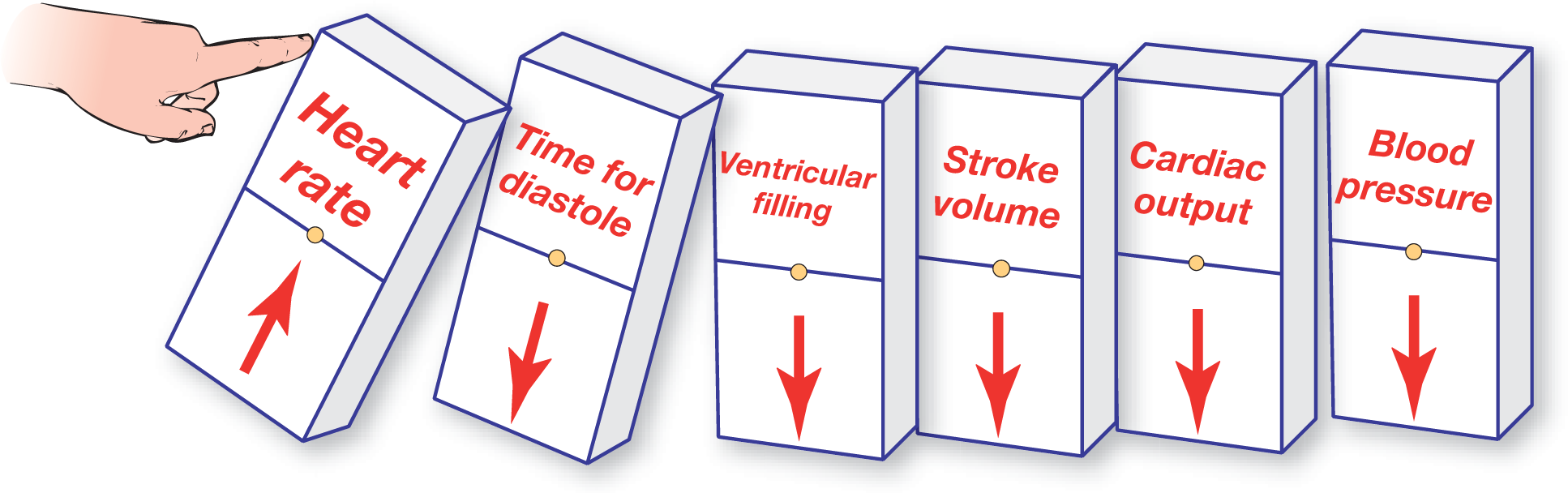
In a tachycardia, both systole and diastole are affected. The problem is that diastole is usually greatly shortened, while systole is only minimally affected. Since ventricular filling occurs during diastole, the amount of blood that actually enters the ventricles is greatly decreased. Clinically, this translates as a markedly decreased cardiac output. Therefore, the lower the end-diastolic blood volume, the lower the cardiac output. In simple terms, the faster the rate, the shorter the period of diastole. The shorter the period of diastole, the lower the ventricular filling. The lower the ventricular filling, the lower the stroke volume. The lower the stroke volume, the lower the blood pressure (Figure 27-24).
Figure 27-24 The hemodynamic consequences of high heart rates.
Hemodynamic stability is, therefore, strongly related to the rate of the tachycardia. At the slower end of the SVT spectrum, the amount of blood that fills the ventricles during ventricular diastole is greater than at faster rates, since there is more time for the blood to enter the ventricles. The increased ventricular filling time translates to an increased ejection fraction and a stronger cardiac output. As the rates become faster, ventricular filling is decreased because, as mentioned previously, the diastolic component of the cardiac cycle is shortened disproportionately. Decreased filling time leads to lower end-diastolic blood volume and lower ejection fractions, causing a weaker cardiac output. At very rapid rates, there is hardly enough time for any significant amount of blood to enter the ventricles and hardly any blood is ejected by the heart. At these rates, the blood pressure drops dramatically.
We saw earlier how the heart rate affects the stroke volume directly. Now let’s turn our attention to how a tachycardia affects the stroke volume indirectly. The amount of blood in the ventricle at the end of diastole will greatly affect how the ventricle contracts. What does this mean? In general, the ventricle contracts in almost a “wringing” motion. The wringing motion is like squeezing a toothpaste tube: You start from the bottom and squeeze toward the top. The synchronized contraction allows for maximal ejection of the end-diastolic blood volume.
As mentioned earlier, synchronized depolarization leads to a synchronized and organized contraction and maximum ejection of whatever blood is present in the ventricles at that time. The synchronized “wringing” contraction can occur only because the electrical conduction system conducts the signal to depolarize, almost instantaneously, to every cell in both ventricles. As we shall see, this synchronization of the ventricular depolarization and organized contraction found in the narrow-complex tachycardias is a major factor in the inherent hemodynamic stability of the SVTs, except at extremely high heart rates.
Decreasing Atrial Kick and Ventricular Overfilling
The atrial kick is the last important point we will look at when considering the hemodynamic effects of any tachycardia. Remember that atrial kick refers to the little extra amount of ventricular overfilling that occurs due to atrial contraction. Some patients can tolerate the loss of the atrial kick without difficulty. Unfortunately, many cannot.
The loss of the atrial kick decreases the end-diastolic ventricular blood volume by not allowing the overfilling of the ventricle. This underfilling decreases the extra “stretch” placed on the ventricular muscle that is needed to maximize contraction strength. The decreased contractility leads to a decreased stroke volume, which in turn leads to a decrease in cardiac output and blood pressure. We discussed this in Chapter 1, Anatomy and Basic Physiology, where we saw that a little overstretching of the ventricular wall causes more forceful contraction of the ventricles.
Retrograde contraction of the atria, as occurs in many SVTs, does not add the atrial kick because the atrial contraction is occurring at the exact same time as ventricular contraction. The net result of a retrograde contraction is negated by contracting against closed valves. As a matter of fact, this retrograde contraction against the obstacle formed by the closed valves pushes blood away from the heart, leading to an interesting physical exam finding—cannon A waves (see the earlier Additional Information box on cannon A waves).
As we have seen in the previous chapters in this section, some of the SVTs have normal, though rapid, atrial contraction, and some do not have any organized atrial activity associated with them at all. In either case, the loss of the atrial kick adds further hemodynamic instability to many tachycardias.
A Few Extra Seconds
The lack of synchronized ventricular activation is one of the main causes of hemodynamic instability that we see with wide-complex tachycardias. In contrast, the SVTs are usually well tolerated by patients in the short run unless the rates are very, very fast. The main reason behind this extra hemodynamic tolerance in the SVTs is that the ventricles are still contracting symmetrically and in a synchronized fashion due to the normally functioning electrical conduction system. The synchronized activation maintains the normal geometry of the ventricles and allows for maximal “wringing” action to occur in these cases. In addition, the atrial kick is often maintained in many of the SVTs.
The extra hemodynamic stability present in many of the SVTs allows us to spend a few extra seconds or minutes correctly identifying the rhythm involved. As we shall see, correctly identifying the rhythm will allow us to focus our treatment and maximize our efforts to improve patient outcome. This is a luxury that is often missing when dealing with a wide-complex tachycardia.
Remember, the faster you treat a patient with any tachycardia, the better it is for the patient. We are not advocating taking more time before treatment. In general, however, with an SVT, you could safely spend a couple of extra seconds analyzing the strip a bit more carefully, as long as the patient remains hemodynamically stable. If the patient is unstable, remember the old adage: “Electricity is our friend.” Electricity, in this case, refers to direct electrical cardioversion or defibrillation, whichever is needed.