Complete or third-degree AV block is a fairly easy block to understand, but isn’t necessarily easy to spot on a rhythm strip. Just as its name implies, complete or third-degree AV block is a complete and total block of conduction to the ventricles (Figure 28-24). In other words, there is a complete failure of the P waves to reach the ventricles. The conduction block can take place at the level of the AV node or lower on the electrical conduction system. This type of block is not typically caused by refractoriness of the node itself, but it is almost always due to a pathologic or anatomic defect in the ventricular electrical conduction system.
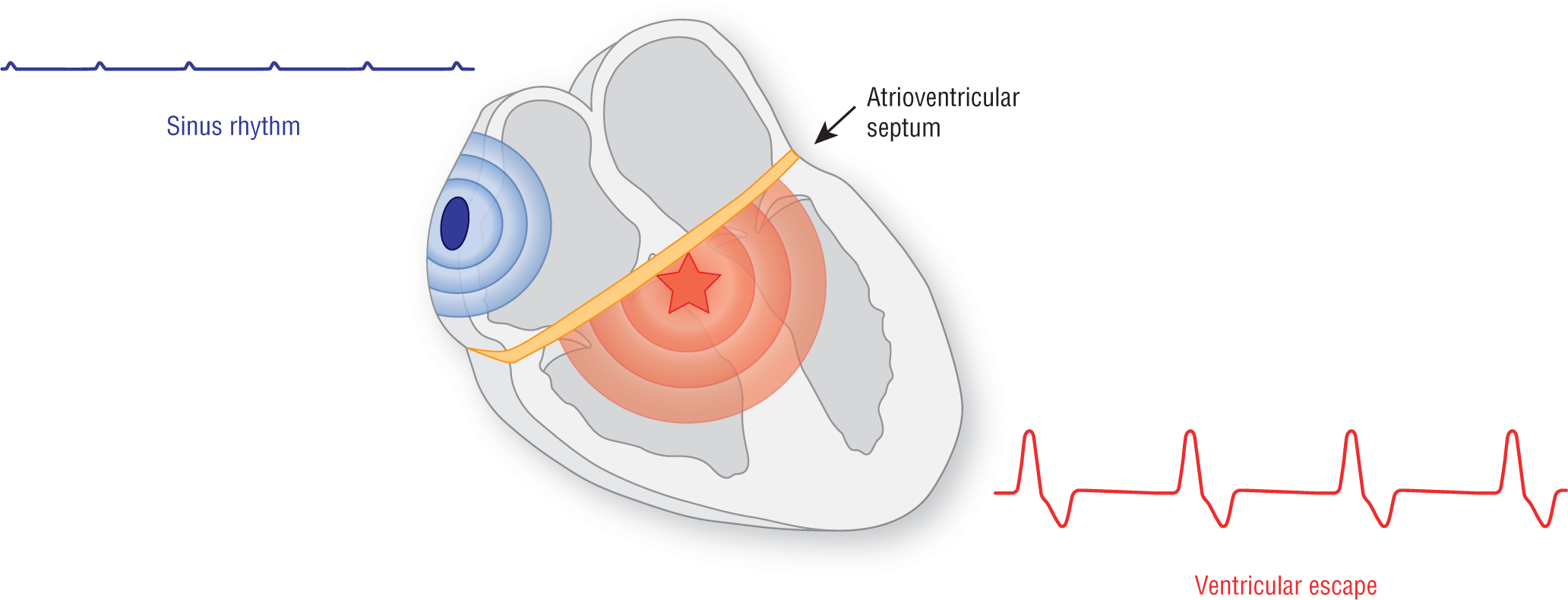
Figure 28-24 When there is a conduction block that is complete, it basically shuts down all communication between the atria and the ventricles. For example, if the AV node is pathologically turned off, a complete block is created at the level of the interventricular septum. The atria and the ventricles are completely oblivious to each other and impulses are generated by two separate pacemakers, one supraventricular and one ventricular. Each pacemaker will keep its own intrinsic rate and control its own respective set of chambers.
In a third-degree block, almost by definition, you need to have two separate pacemakers. The supraventricular pacemaker (either sinus, ectopic atrial, or junctional), since it is a higher-order pacemaker, will usually fire spontaneously. But, a ventricular pacemaker is also mandatory in order to maintain cardiac output and, hence, life. In other words, a lower-order pacemaker from the ventricles must fire and set the ventricular pace in order for the patient to survive.
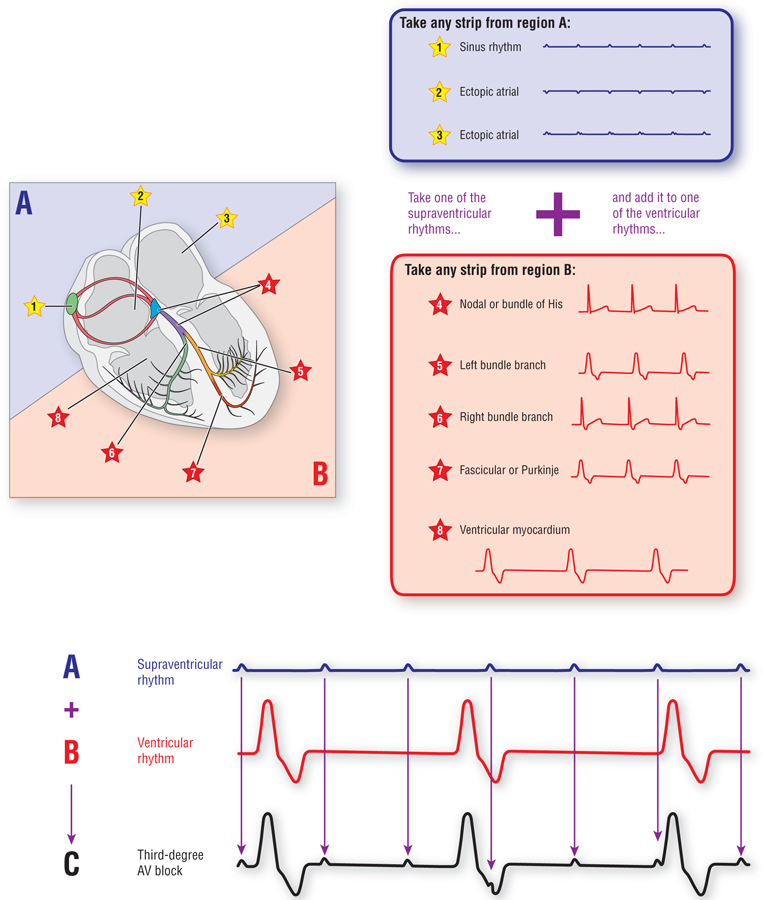
The morphology of the final rhythm will depend on the two individual rhythms that make it up. The two individual rhythms, in turn, depend on the ectopic site of the pacemakers involved (Figure 28-25). If the supraventricular rhythm originates in the sinus node, the morphology of the complexes will be sinus in nature. If they originate in an ectopic site, the morphologic appearances of the supraventricular rhythm will depend on the location of the ectopic focus that created it and the route taken by the atrial depolarization wave to depolarize the actual atrial myocardium. Likewise, the morphologic appearance of the ventricular rhythm will depend on the site of the ectopic focus that created it and the route of transmission that the ventricular depolarization wave will take through the ventricles. An ectopic focus that uses only direct cell-to-cell transmission will give rise to a very wide QRS complex. An ectopic focus that partially uses any part of the electrical conduction system will be narrower, reflecting the faster rate of transmission of the depolarization wave.
Figure 28-25 A pacemaker in the supraventricular area will create a supraventricular rhythm (blue area and blue block). A pacemaker in the ventricular area will give rise to a ventricular rhythm (red area and red block). If you take any one of the supraventricular strips and superimpose it electrocardiographically to any one of the ventricular strips, you end up with a strip showing a third-degree AV block (see Figure at bottom). Note that neither the supraventricular rhythm nor the ventricular rhythm has any influence whatsoever on the other.
Third-degree AV block represents a failure of all of the P waves to be conducted to the ventricles. The rate of the subsidiary ventricular rhythm will depend on the ectopic site of origin for the pacemaker creating the rhythm. A junctional pacemaker will typically have narrow QRS complexes that are between 40 and 60 BPM. A ventricular pacemaker will typically have wide QRS complexes and a rate between 30 and 45 BPM. Occasionally, the ventricular rate will be very slow, sometimes occurring in the 30s or lower. That said, remember that any pacemaker can have accelerated automaticity or may trigger a reentry circuit. In those cases, the ventricular rhythm may be tachycardic.
The width of the QRS complex can help you somewhat with the site of the block. Narrow complexes originate in either the AV node or the bundle of His in over 90% of the cases. Wide complexes (≥ 0.12 seconds) can originate in the AV node or bundle of His if there is a preexisting bundle branch block, aberrancy, electrolyte disturbance, or some other predisposing condition. If they do not have any of these preexisting conditions, then the site of origin is usually infra-Hisian.
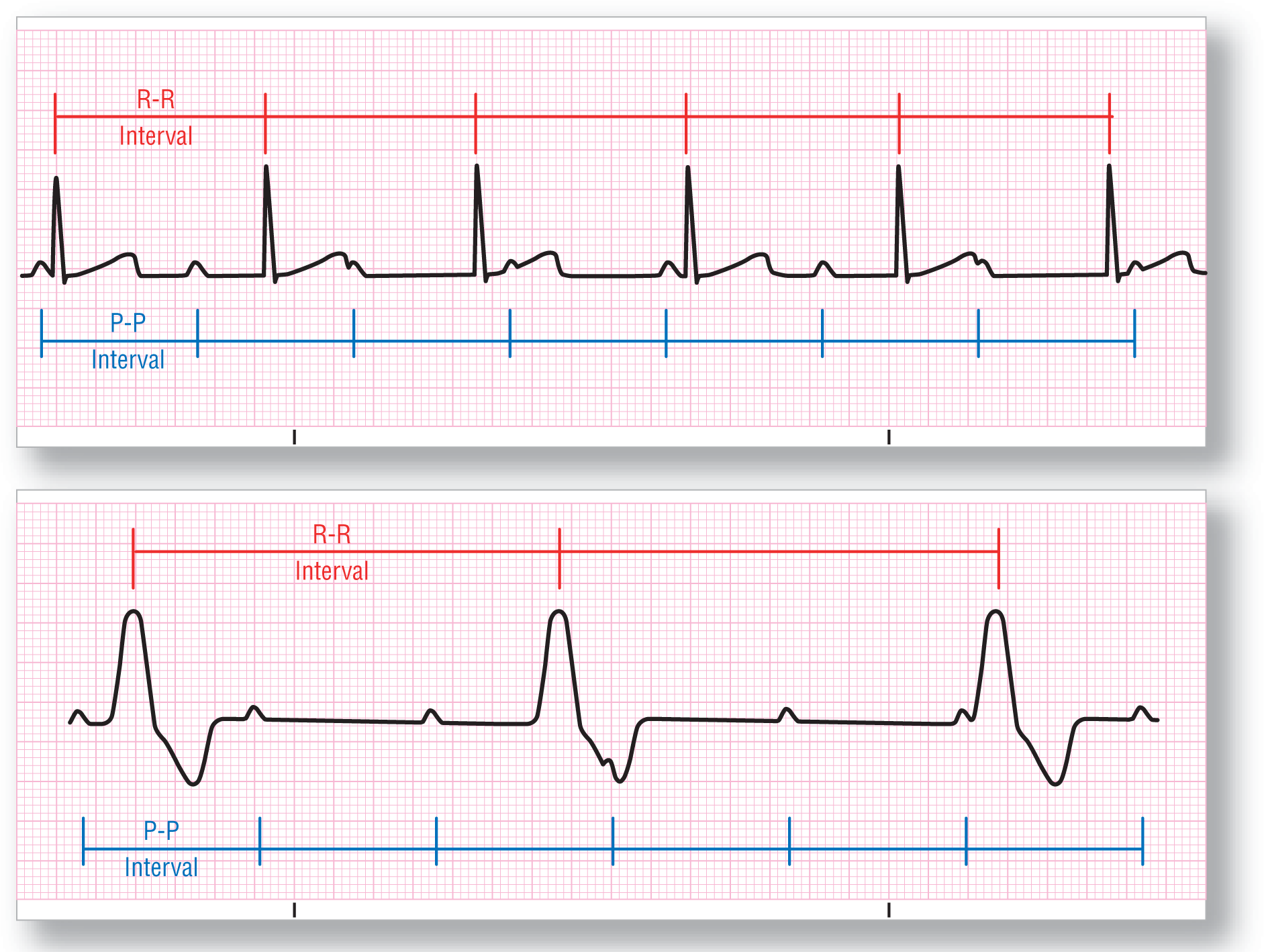
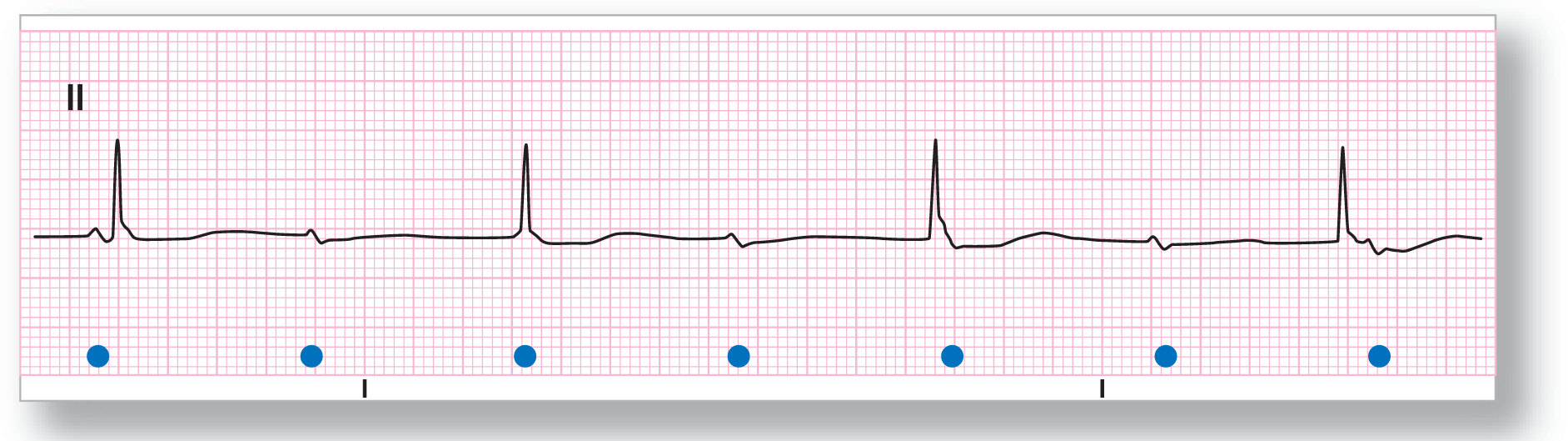
In third-degree AV block, the P-P intervals of the supraventricular rhythm and the R-R intervals of the ventricular rhythm will both be constant (Figure 28-26). They will, however, have no association whatsoever with each other. Each beats to its own drummer . . . or pacemaker. The net result is that the PR interval is completely changing and never exactly repeats throughout the entire strip. Recognizing the consistency of the individual components and the complete lack of any association between the two is the key to diagnosing a third-degree AV block.
Figure 28-26 Two examples of third-degree or complete AV block. Note that the P-P intervals and R-R intervals are consistent in each strip. There is, however, no communication at all between the supraventricular and the ventricular components of each strip. This is indirectly demonstrated by the ever-changing PR intervals.
Ventriculophasic AV dissociation refers to a variation of third-degree AV block. In this variation, the P-P interval narrows slightly whenever a QRS complex falls between two P waves. The P-P intervals that do not have a QRS complex are not narrowed. The result is that the strip appears to have two different P-P intervals, one when there is a QRS involved and a different one when there is no QRS involved (Figure 28-27).
Figure 28-27 Ventriculophasic AV dissociation with the intervals that include a QRS complex at 0.8 seconds and the intervals without a QRS complex at 0.96 seconds.
The presence of ventriculophasic AV dissociation is not clinically relevant, but it can sometimes cause a diagnostic dilemma. Awareness of this variation and close measurement of the intervals with an eye on the presence of QRS complexes will facilitate the diagnosis of the rhythm.
An easy way to remember it is that the QRS complex “pulls in” the P waves surrounding it. Another good memory aid is to think of a field goal in football (Figure 28-28). The QRS complex would be the football, which is being kicked between the two goal posts (the P waves). Making the field goal pulls the goal posts into each other. Missing the field goal doesn’t do a thing.
Figure 28-28 Ventriculophasic AV dissociation is like a field goal. When the football makes it, the goalposts shake from the cheering and come in toward each other. When you don’t make it, nothing happens.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 65 BPM Ventricular: 35 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Wide
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
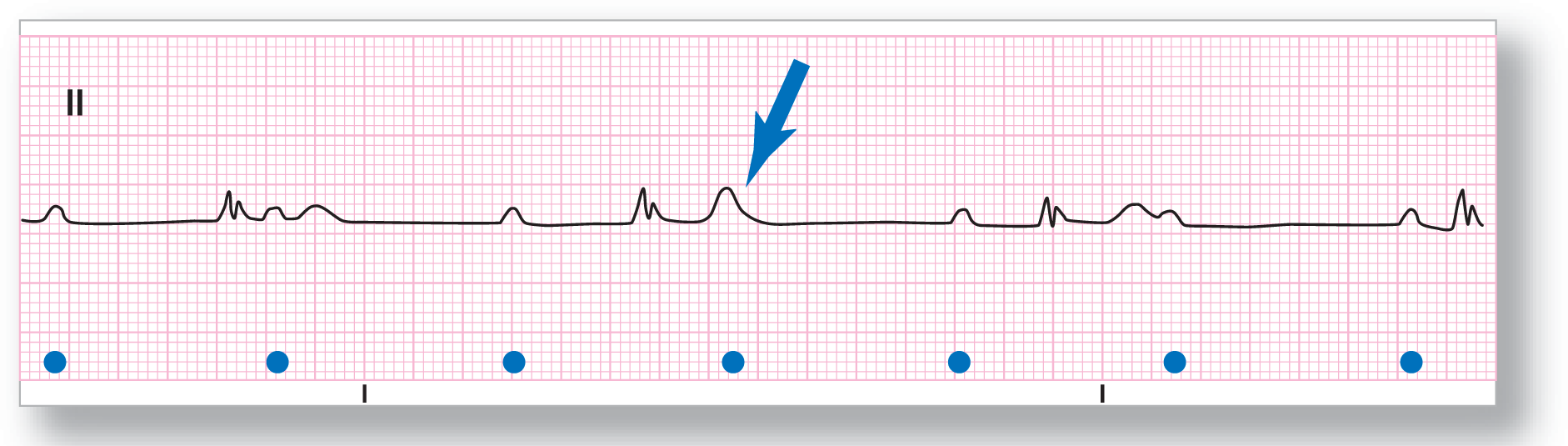
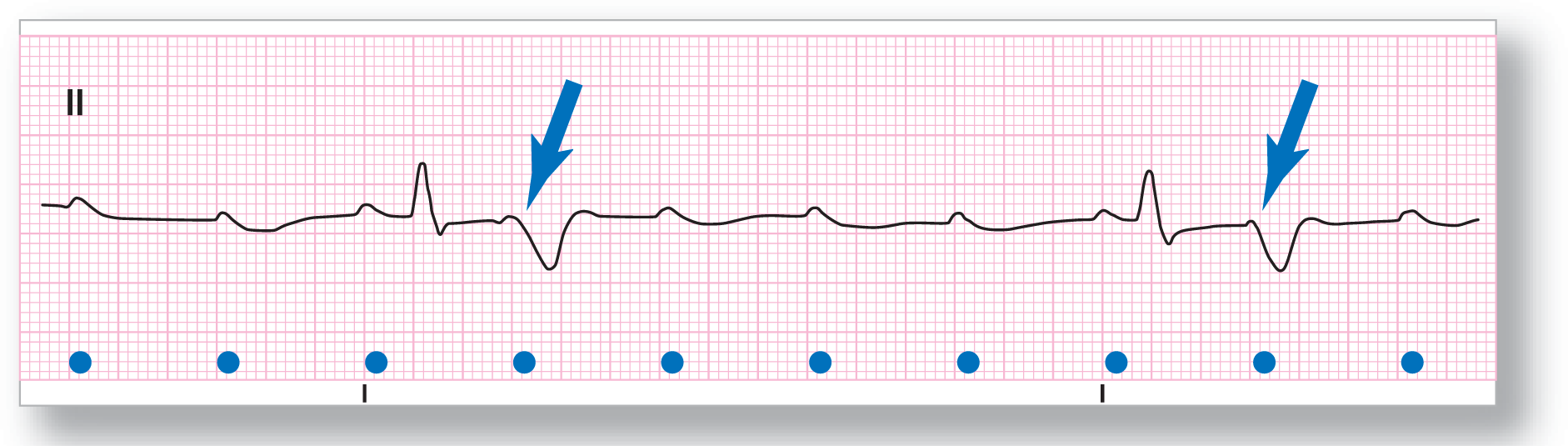
ECG 28-22 shows a third-degree AV block with a sinus rhythm and ventricular escape. The P waves are upright and map consistently throughout the strip. The blue arrow points out a buried P wave lying inside the T wave of the second complex. There is some slight irregularity of the P-P interval, which is ventriculophasic in nature. The P-P intervals without any QRS complexes are very consistent. The P-P intervals with QRSs inside them vary slightly in width, which is atypical.
ECG 28-23
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 100 BPM Ventricular: 20 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Wide
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
ECG 28-23 shows an underlying sinus tachycardia, which is completely blocked from reaching the ventricles. The ventricles are paced by a ventricular escape rhythm at about 20 BPM. Notice the wide QRS complexes with abnormal ST segments and T waves. The blue arrows point out buried P waves in the T waves of the ventricular complexes. Note the inconsistencies in the PR intervals shown, which is indicative of the complete AV block in this patient.
ECG 28-24
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 57 BPM Ventricular: 39 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Narrow
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
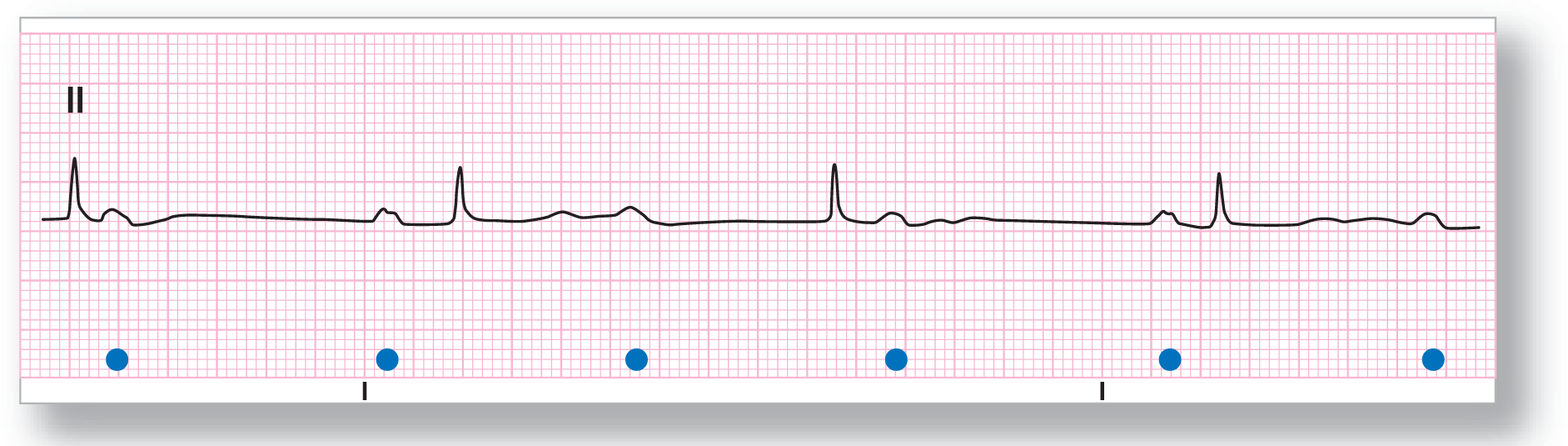
ECG 28-24 shows a complete or third-degree AV block with a sinus bradycardia and a junctional escape rhythm at a rate of about 39 BPM. The lack of communication between the atria and ventricles is obvious from examining the strip. Note that the PR intervals in front of the second and fourth QRS complexes are not the same.
ECG 28-25
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 90 BPM Ventricular: 45 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Wide
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
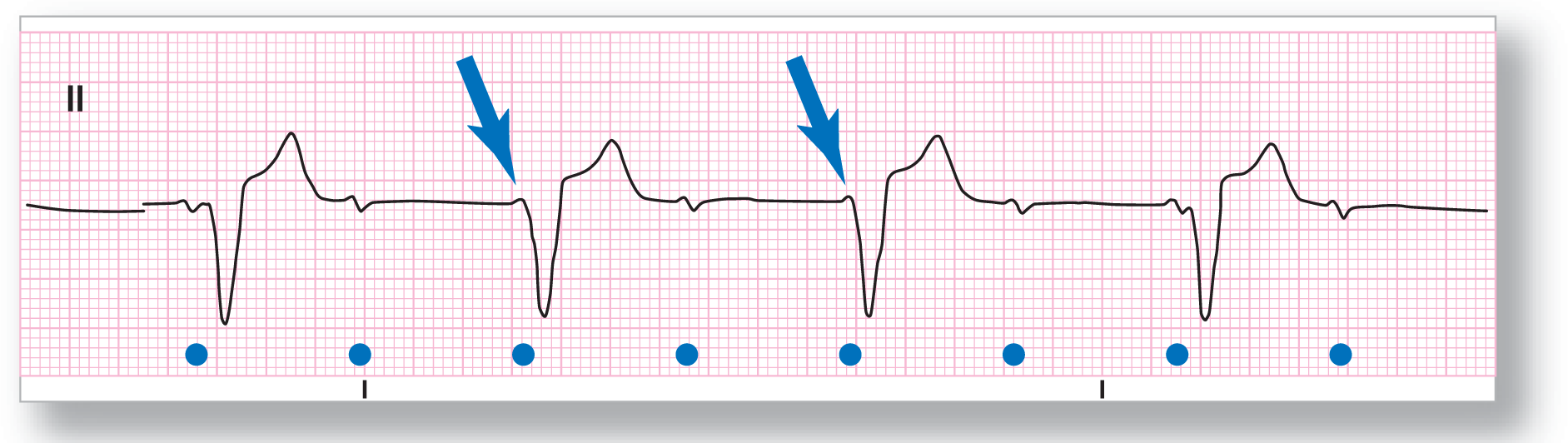
ECG 28-25 shows a probable sinus rhythm with biphasic P waves. The ventricular rhythm is about 45 BPM, which could fall into the realm of either a junctional rhythm with a preexisting left bundle branch block or a more likely ventricular escape rhythm. An old ECG would be invaluable in confirming the final diagnosis. The presence of the third-degree AV block, however, cannot be disputed. The blue arrows point to the presence of two buried P waves.
ECG 28-26
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 79 BPM Ventricular: 44 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Narrow
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
ECG 28-26 shows a third-degree AV block with an underlying sinus rhythm and a junctional escape. Note how the first two QRS complexes are taller than the others. This is probably due to the fusion with the underlying P waves that just happen to fall at the same time. Using your calipers to map out a P-P interval width and then walking it back and forth across the strip is your best way to evaluate these rhythms and isolate the respective waves.
ECG 28-27
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 88 BPM Ventricular: 33 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Wide
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
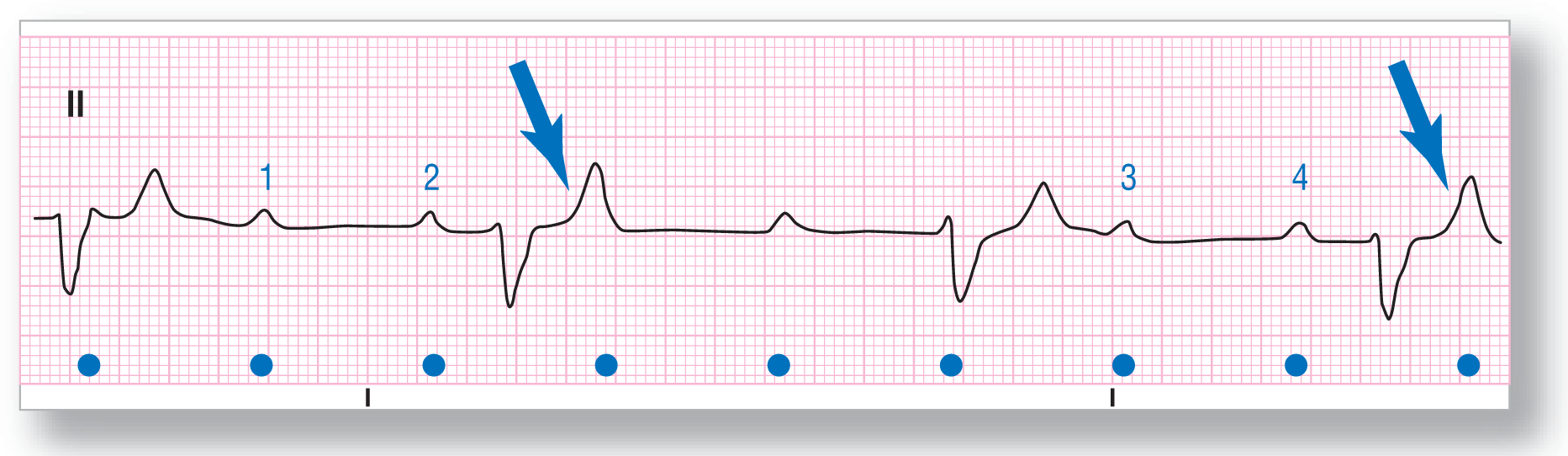
ECG 28-27 shows a complete heart block with an underlying sinus rhythm at about 88 BPM and a ventricular escape rhythm at 33 BPM. This ECG facilitates the diagnosis of the complete block by letting us see clearly two P waves occurring side by side with no QRS complexes. These P waves are labeled 1,2, 3, and 4. Mapping out the distance between waves 1 and 2 and then walking the calipers over to waves 3 and 4 points out the consistency of the atrial rhythm. The blue arrows point to buried P waves.
ECG 28-28
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 70 BPM Ventricular: 36 BPM
PR intervals: Variable
Regularity: Regular
QRS width: Narrow
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
ECG 28-28 shows a third-degree AV block with an underlying sinus rhythm and a junctional escape. The second and third QRS complexes have buried P waves associated with them. A clinical pearl: Whenever you have a P wave fall right in between two QRS complexes, always try to find the buried P wave. In this case, the search is simplified by the appearance of the first P wave right before the first QRS complexes. Walking this distance forward will clearly show the buried P waves.
ECG 28-29
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Rate: Atrial: 60 BPM Ventricular: 115 BPM
PR intervals: Variable
Regularity: Regularly
QRS width: Wide
P waves: Normal
Morphology: Normal
Axis: Normal
Grouping: None
Dropped beats: Present
P:QRS ratio: Variable
Rhythm: Third-degree AV block
Discussion:
ECG 28-29 shows a very unfortunate patient who went from a 2:1 AV block into a complete AV block with ventricular standstill. Unfortunately for him, neither a junctional nor a ventricular pacemaker took over the pacing function for the ventricles. This patient highlights the lesson which we mentioned before, that all patients with serious AV blocks should have either a transcutaneous pacemaker or a transvenous pacemaker available at all times and ready to use. In these patients, time is critical.